Ok so Omni and I have agreed that I’m gonna use this as an opportunity to talk about Pre-Hospital Care for Pelvic Fractures.
Buckle up,
A thread is forming....
1/
Buckle up,
A thread is forming....
1/
Ok so.
Pelvic fractures - they’re HIGHLY vascularised bones surrounding super vascular tissues. Fractures = bad ?
Got it
Perfect
Moving on
There’s a few things to be concerned about.
0. Pain
1. Bleeding
2. Clotting (and disorders of clotting)
3. Nerves
4. Organs
5. Other stuff
Pelvic fractures - they’re HIGHLY vascularised bones surrounding super vascular tissues. Fractures = bad ?
Got it
Perfect
Moving on
There’s a few things to be concerned about.
0. Pain
1. Bleeding
2. Clotting (and disorders of clotting)
3. Nerves
4. Organs
5. Other stuff
So.
How do I know if the patient had broken their pelvis?
Well. If they tell you they’ve broken their pelvis that’s usually a fairly reliable indicator.
Well, if both you and the patient aren’t sure; whilst they’re lying down, see if they can lift their own leg straight up.
3/
How do I know if the patient had broken their pelvis?
Well. If they tell you they’ve broken their pelvis that’s usually a fairly reliable indicator.
Well, if both you and the patient aren’t sure; whilst they’re lying down, see if they can lift their own leg straight up.
3/
Straight leg raise is a fantastic rule out tool for pelvic fracture in the awake and alert patient
ncbi.nlm.nih.gov/m/pubmed/29132…
ncbi.nlm.nih.gov/m/pubmed/29132…
You’ll notice I haven’t talked about actually touching the pelvis and that the caveat here was “if both you and the patient don’t know.”
Why?
If either you or the patient THINK the pelvis is broken- treat it as if it is.
Either way touching (or worse: rocking) is a useless exam
Why?
If either you or the patient THINK the pelvis is broken- treat it as if it is.
Either way touching (or worse: rocking) is a useless exam
Trying to determine whether a circular complex bony structure is broken by touching two points is like ... well, it’s just not good.
don’t do it.
So
We think the pelvis is broken or the patient isn’t fully alert to tell us.
What do we do now?
don’t do it.
So
We think the pelvis is broken or the patient isn’t fully alert to tell us.
What do we do now?
We bind it.
Like a book.
An Open book if you will
Like a book.
An Open book if you will
So what’s the evidence on pelvic binders?
Yeah im not going to lie to you it’s not amazing.
Frankly a lot of people with ploy trauma die so it’s difficult to test this well.
But we are pretty sure that pelvic binders contribute some benefit and minimal harms.
So please use them.
Yeah im not going to lie to you it’s not amazing.
Frankly a lot of people with ploy trauma die so it’s difficult to test this well.
But we are pretty sure that pelvic binders contribute some benefit and minimal harms.
So please use them.
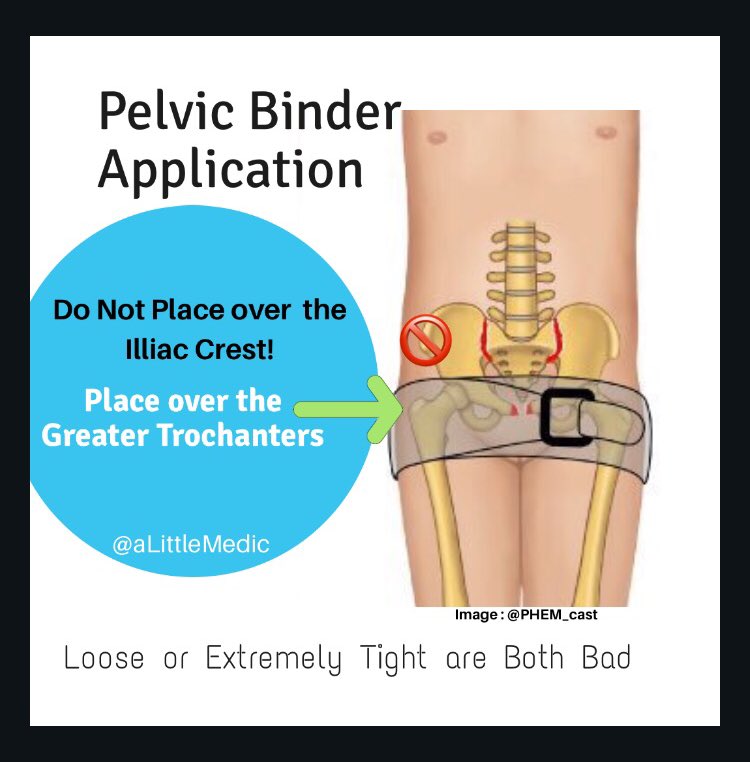
How do we use them?
1. Take their clothes off.
Binder goes against skin! Always.
2. Apply it at the top of the legs, NOT the pointy part of the hips.
3. firm. Snug. Like you’re supporting a broken bone - not tight like mooring a boat or soft like applying a blanket.
1. Take their clothes off.
Binder goes against skin! Always.
2. Apply it at the top of the legs, NOT the pointy part of the hips.
3. firm. Snug. Like you’re supporting a broken bone - not tight like mooring a boat or soft like applying a blanket.
Ok.
Binder is on.
Wait.
Hang on a second.
HOW did we get it on?
Ok.
A few ways.
1. Use a SCOOP stretcher to get the patient off the ground and place them on a bed. Think ahead and have already laid the binder out underneath them on the bed. Put the patient on top and bind.
Binder is on.
Wait.
Hang on a second.
HOW did we get it on?
Ok.
A few ways.
1. Use a SCOOP stretcher to get the patient off the ground and place them on a bed. Think ahead and have already laid the binder out underneath them on the bed. Put the patient on top and bind.
2. Wiggle it up gently underneath their legs until it’s in the right place. Do this slowly and gently. Movement hurts.
3. Log roll the patient like a normal trauma patient and smoosh all the broken bone fragments together in a painful, often unnecessary, and harmful manoeuvre.
3. Log roll the patient like a normal trauma patient and smoosh all the broken bone fragments together in a painful, often unnecessary, and harmful manoeuvre.
Ok.
The pelvis has been bound.
We’ve fixed their fracture right?
Not quite.
See, pelvic binders are good at some things but they aren’t a panacea.
What they do well:
✅ motion restriction = less pain
✅ reduce bony / venous bleeding
✅ lessen clot disruption
✅ visual warning
The pelvis has been bound.
We’ve fixed their fracture right?
Not quite.
See, pelvic binders are good at some things but they aren’t a panacea.
What they do well:
✅ motion restriction = less pain
✅ reduce bony / venous bleeding
✅ lessen clot disruption
✅ visual warning
What pelvic binders do not achieve:
❌ total pelvic stabilisation
❌ arterial tamponade
❌ potent analgesia
❌ fix coagulopathy
❌ total pelvic stabilisation
❌ arterial tamponade
❌ potent analgesia
❌ fix coagulopathy
So,
That means we still need to do some things:
✳️ minimise movement as much as possible to reduce pain and clot disruption
✳️ provide multimodal analgesia (I’ll come to this further down)
✳️target coagulopathy (TXA, warmth, don’t dilute with massive crystalloid bolus)
That means we still need to do some things:
✳️ minimise movement as much as possible to reduce pain and clot disruption
✳️ provide multimodal analgesia (I’ll come to this further down)
✳️target coagulopathy (TXA, warmth, don’t dilute with massive crystalloid bolus)
What else?
They need a fully capable trauma centre.
A place with CT scanners, orthopaedic surgeons, AND interventional radiology - some pelvises need embolisation (radiologists plugs the holes) before, instead, or in combo with ortho.
The Local ER might not cut it 🤦🏻♀️
They need a fully capable trauma centre.
A place with CT scanners, orthopaedic surgeons, AND interventional radiology - some pelvises need embolisation (radiologists plugs the holes) before, instead, or in combo with ortho.
The Local ER might not cut it 🤦🏻♀️
Let’s talk about analgesia.
What are the options?
First up: opioids.
This is not the time to single handedly fix America’s opioid crisis. Be generous.
Adjuncts:
Ketamine (its twitter, can’t leave it out), IV paracetamol, Nitrous Oxide, NSAIDS are contentious.
And....
What are the options?
First up: opioids.
This is not the time to single handedly fix America’s opioid crisis. Be generous.
Adjuncts:
Ketamine (its twitter, can’t leave it out), IV paracetamol, Nitrous Oxide, NSAIDS are contentious.
And....
Regional Anaesthesia !
That’s right.
You can do a nerve block!
How?
Well, there’s two kinds of Fascia Illiaca Compartment Blocks*:
infra-inguinal and supra-Inguinal
(Below or above the inguinal ligament)
The traditional *FICB can be done blindly below the ligament ...
That’s right.
You can do a nerve block!
How?
Well, there’s two kinds of Fascia Illiaca Compartment Blocks*:
infra-inguinal and supra-Inguinal
(Below or above the inguinal ligament)
The traditional *FICB can be done blindly below the ligament ...
Problem is, this really only hits the femoral nerve which is a bit too far down for us.
We really want to be hitting the obturator Nerve and as high up into the plexus as possible to block as much pelvic pain innervation as possible.
So, we really need to go above the ligament.
We really want to be hitting the obturator Nerve and as high up into the plexus as possible to block as much pelvic pain innervation as possible.
So, we really need to go above the ligament.
Going above the ligament for a Supra-Inguinal FICB is dangerous unless you’re using ultrasound (tiger territory - could hit important things).
Now.
The patient might be sore on one side (good - do it on this side)
Or they might be sore on both sides (this makes things trickier)
Now.
The patient might be sore on one side (good - do it on this side)
Or they might be sore on both sides (this makes things trickier)
So, we are going to block the sore side.
Using ultrasound.
Above the inguinal ligament.
Remember that fascial plane Blocks are VOLUME blocks.
So use 40-50mls of dilute local anaesthetic.
Lidocaine is always a safe option.
If you wanna get fancy then ropivicaine is good.
Using ultrasound.
Above the inguinal ligament.
Remember that fascial plane Blocks are VOLUME blocks.
So use 40-50mls of dilute local anaesthetic.
Lidocaine is always a safe option.
If you wanna get fancy then ropivicaine is good.
But what if both sides hurt?
Technically speaking you *could* do bilateral FICBs using reduced doses and dilute solutions, dual Fem Nerve blocks are done for elective procedures in some places.... but I’m not sure I’d be too keen to jump on that bandwagon just yet.
Technically speaking you *could* do bilateral FICBs using reduced doses and dilute solutions, dual Fem Nerve blocks are done for elective procedures in some places.... but I’m not sure I’d be too keen to jump on that bandwagon just yet.
What we do know however is that pain relief matters.
Trauma patients are at a HIGH (up to 1 in 3) risk of developing post traumatic stress reactions and persistent neuropathic pain syndromes.
Analgesia is crucial.
Trauma patients are at a HIGH (up to 1 in 3) risk of developing post traumatic stress reactions and persistent neuropathic pain syndromes.
Analgesia is crucial.
And speaking of high risk,
Let’s mention that pelvic fractures in the over 65yo age group can be more common, require less force, and be more subtle to detect
Let’s mention that pelvic fractures in the over 65yo age group can be more common, require less force, and be more subtle to detect
So
TL;DR
Pelvic Fractures:
✅Be suspicious
🆕Straight leg raise to rule out low risk patients
‼️Bind against skin, not hip pointy bits
🛑Minimise movement
🌀Give analgesia
☢️Take to IR & Surgery Capable facility
💔Target coagulopathy if needed
🚷Don’t stand them up!
TL;DR
Pelvic Fractures:
✅Be suspicious
🆕Straight leg raise to rule out low risk patients
‼️Bind against skin, not hip pointy bits
🛑Minimise movement
🌀Give analgesia
☢️Take to IR & Surgery Capable facility
💔Target coagulopathy if needed
🚷Don’t stand them up!