1. Earlier in December I had the privilege to speak at the Cardiovascular Collaborative Medicine Conference in Manhattan on the role of catheter ablation post CABANA. I thought I'd present that talk via tweetorial. I'm not sure how well it will adapt to this form, but here goes.. 

2. As we work our way through this presentation I want you to keep in mind this patient profile. Specifically we are going to frame the conversation around a young patient with recurrent AF despite the use of AAD therapy as this is the profile where the evidence is most robust.

3. Why do we care about Atrial Fibrillation? Firstly, it is an important clinical problem. It is increasingly common as the general population ages (and by extension our patients). The estimated lifetime-risk of developing AF is 22-26% for individuals 40-55 years of age.

4. Beyond this high prevalence, AF is an expensive clinical problem. Acute care of AF accounted for ~1% of the overall NHS budget in 2000. And that doesn't take into account lost productivity, premature mortality, or nursing home costs. On average an AF patient costs $6,692/year.

5. A big driver of the health care utilization (and acute care costs) comes back to the simple observation that AF patients are (generally) symptomatic. When you compare healthy controls (open bars) to AF patients (solid) it is clear that quality of life is impaired.

6. One of the pillars of AF management is entered on symptomatic improvement. To this end RCTs have demonstrated that treatment initiation (RATE or RHYTHM control) results in symptomatic improvement across multiple domains.

7. These RCTs have also demonstrated that, in minimally symptomatic patients, a strategy of RATE control is non-inferior to RHYTHM control in terms of "hard" endpoints such as "all-cause" or "cardiovascular" mortality.


8. So, if RATE control improves symptoms and does not adversely affect mortality, then why do we pursue RHYTHM control?

9. We pursue RHYTHM control because being in sinus rhythm is associated with improved symptoms compared to being in rate controlled AF. In this example there is benefit from rate control, but the magnitude of symptomatic improvement is greatest in sinus.

11. This symptomatic benefit in sinus rhythm is a consistent finding across multiple "Rate vs. Rhythm" RCTs.
To quote the RACE Study "the presence of sinus rhythm (SR) at the end of follow-up, rather than the assigned strategy, was associated with QoL improvement."
To quote the RACE Study "the presence of sinus rhythm (SR) at the end of follow-up, rather than the assigned strategy, was associated with QoL improvement."

12. Reason two why we pursue sinus rhythm relates to "reverse remodelling" and physiological improvement. But rather than repeat myself, just keep this in mind as we'll come back to it later.

13. Reason three is the "suggestion" of an association between sinus rhythm and a mortality benefit. The large Quebec cohort study suggests that a time horizon longer than the duration of f/u in the RvR trials (dashed lines) is needed to see the RHYTHM mortality advantage

14. There is a suggestion that RHYTHM control may reduce stroke risk (ie dronedarone trial). We know that AF burden is related to stroke event rates, but this was not shown in RvR trials. However, like mortality, Quebec data suggests the time horizon to see it needs to be long.

15. So, if there is a reason to pursue RHYTHM control, then what is the best way to achieve it?

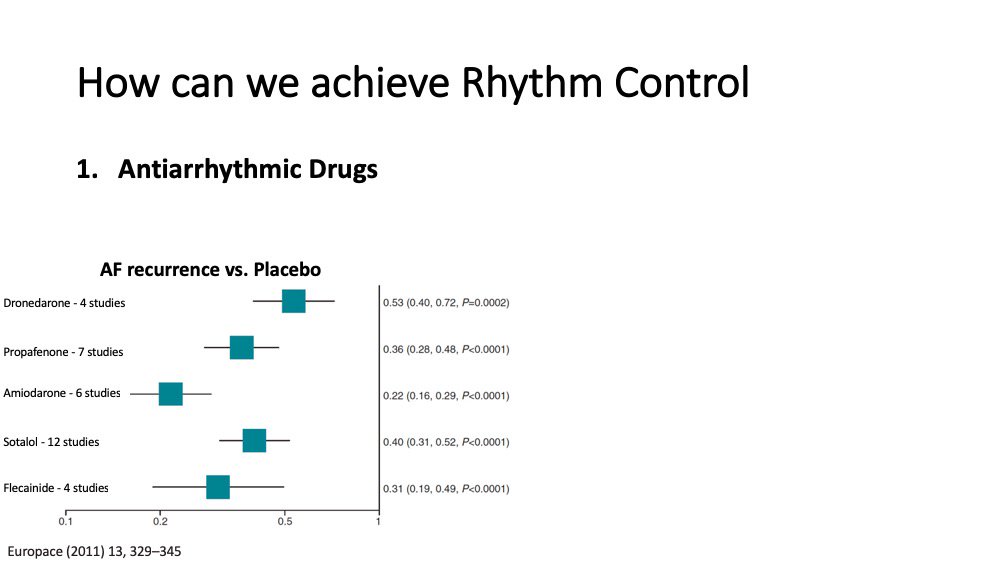
16. The cornerstone of rhythm management is the use of AAD therapy.
These medications have been studied in multiple placebo controlled RCTs.
Each of the 5 agents is superior to placebo at controlling rhythm (ie AF suppression). But...
These medications have been studied in multiple placebo controlled RCTs.
Each of the 5 agents is superior to placebo at controlling rhythm (ie AF suppression). But...
17. Despite being superior to placebo, AAD therapy is of limited efficacy. Which is a problem of the RATE vs. RHYTHM RCTs, in the sense that the Rhythm control group was in AF >20% of the time, and the rate group was in AF ~40% of the time.

18. Why does it matter? If we look at AFFIRM we see that the beneficial effect of AADs (eg, 46% mortality improvement with maintenance of SR) may be offset by the impact of their adverse effects (40% decrease in survival due to toxicity, morbidity, and mortality).
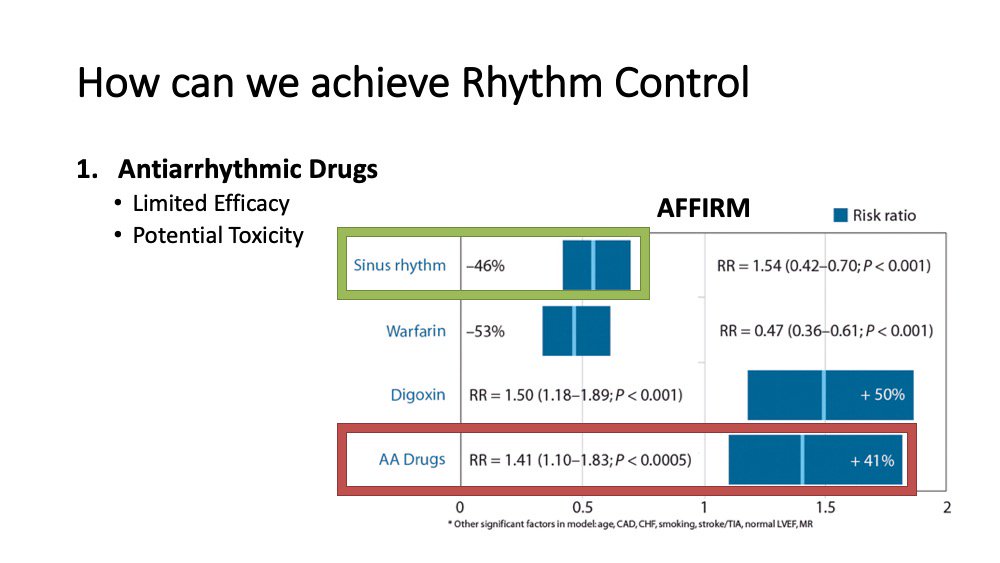
19. To quote the AFFIRM analysis authors "If an effective method for maintaining SR with fewer adverse effects were available, it might be beneficial."

20. We know that ablation effectively manages the arrhythmia. Presented here are a selection of 8 ILR tracings showing an absence of AF following the pulmonary vein isolation procedure. But the plural of anecdote is anecdotes, not evidence...

21. So we turn to RCTs. In each of these large, multi-centre, randomized controlled trials we see that Ablation is universally superior to AADs (which were previously shown to be superior to placebo). This was also shown in CABANA, which returned an entirely consistent result.


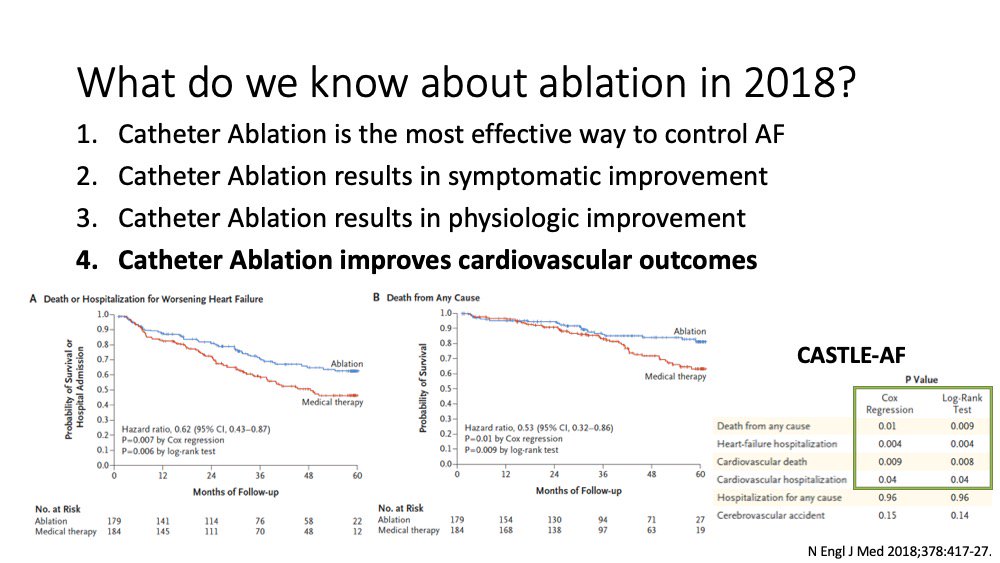
22. Beyond the "time to first event" we also know that AF ablation reduces the "burden" of AF (or amount of time someone spends in AF). While we have known that stroke outcomes are related to AF burden, recent data suggests mortality and hospitalisation are as well (CASTLE-AF).

23. Moreover, we know that Ablation significantly improves symptoms and HRQOL compared to AAD therapy. While this data isn't placebo controlled, we have to remember that previous studies have compared AAD therapy to placebo and to rate control.

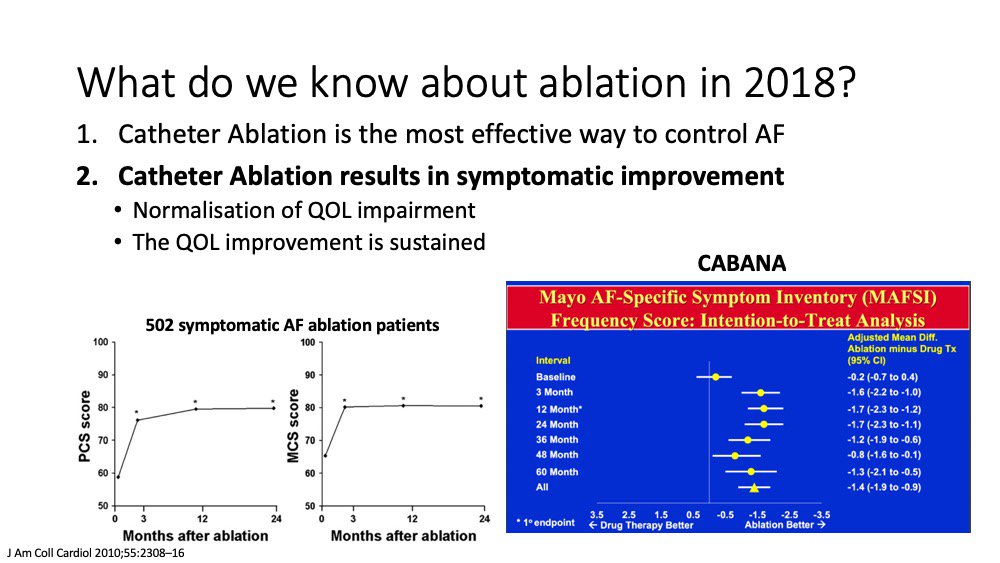
24. These previous studies showed rate control/AAD therapy does improve HRQOL/Symptoms, but the improvement with ablation is: 1) superior to medical therapy, 2) sustained, and 3) results in "normalization" of HRQOL.
Medical therapy does improve, but not normalize symptom status.
Medical therapy does improve, but not normalize symptom status.

25. This sustained improvement has been shown in multiple studies, including CABANA. In data presented at this past @escardio congress we see that ablation is superior to medical therapy at all time points up to 60 months post procedure, potentially arguing against placebo effect
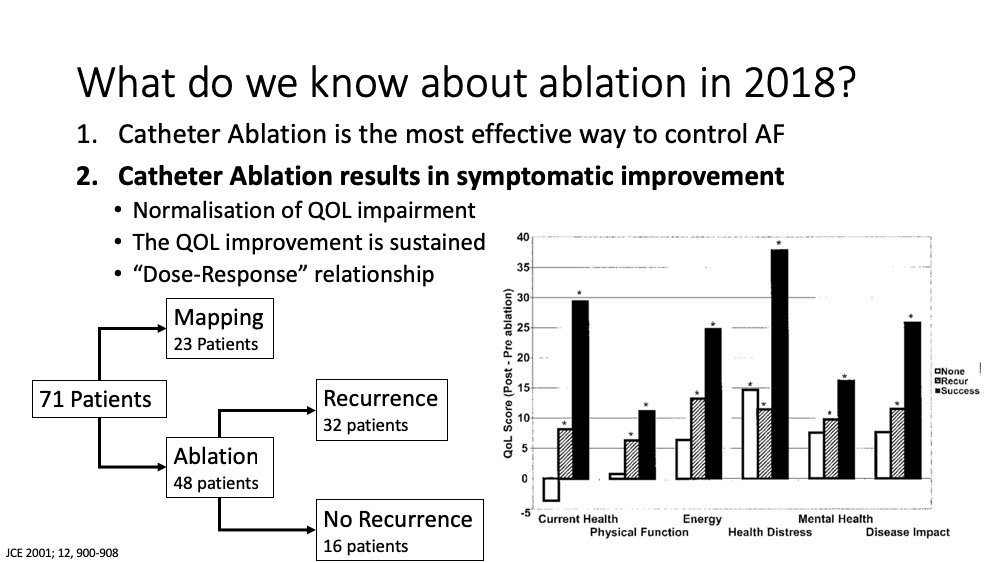
26. Likewise, studies have related these outcomes to the procedure and outcomes. In this series from @Ed_Gerst outcomes were worse in the ~1/3 of patients underwent mapping alone (no ablation), intermediate in the 20% who had recurrence, and best in 35% with successful ablation.
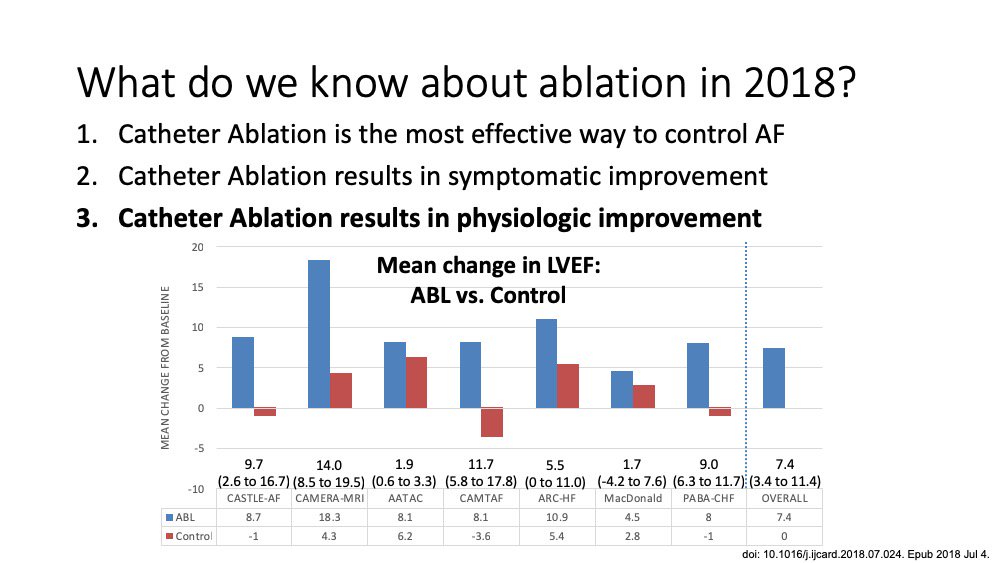
27. From a physiology standpoint, we know that ablation improves outcomes such as left atrial appendage velocity, BNP, VO2 max, and LVEF. For the latter, the improvement is substantial and consistent across multiple randomised trials suggesting the observed effect is real.

28. From a cardiovascular outcome perspective, we know that ablation improves outcomes such as mortality and hospitalization in higher risk populations, such as those with HF (as demonstrated in CASTLE).
But the reduction in hospitalization/mortality was also seen in CABANA ITT.
But the reduction in hospitalization/mortality was also seen in CABANA ITT.

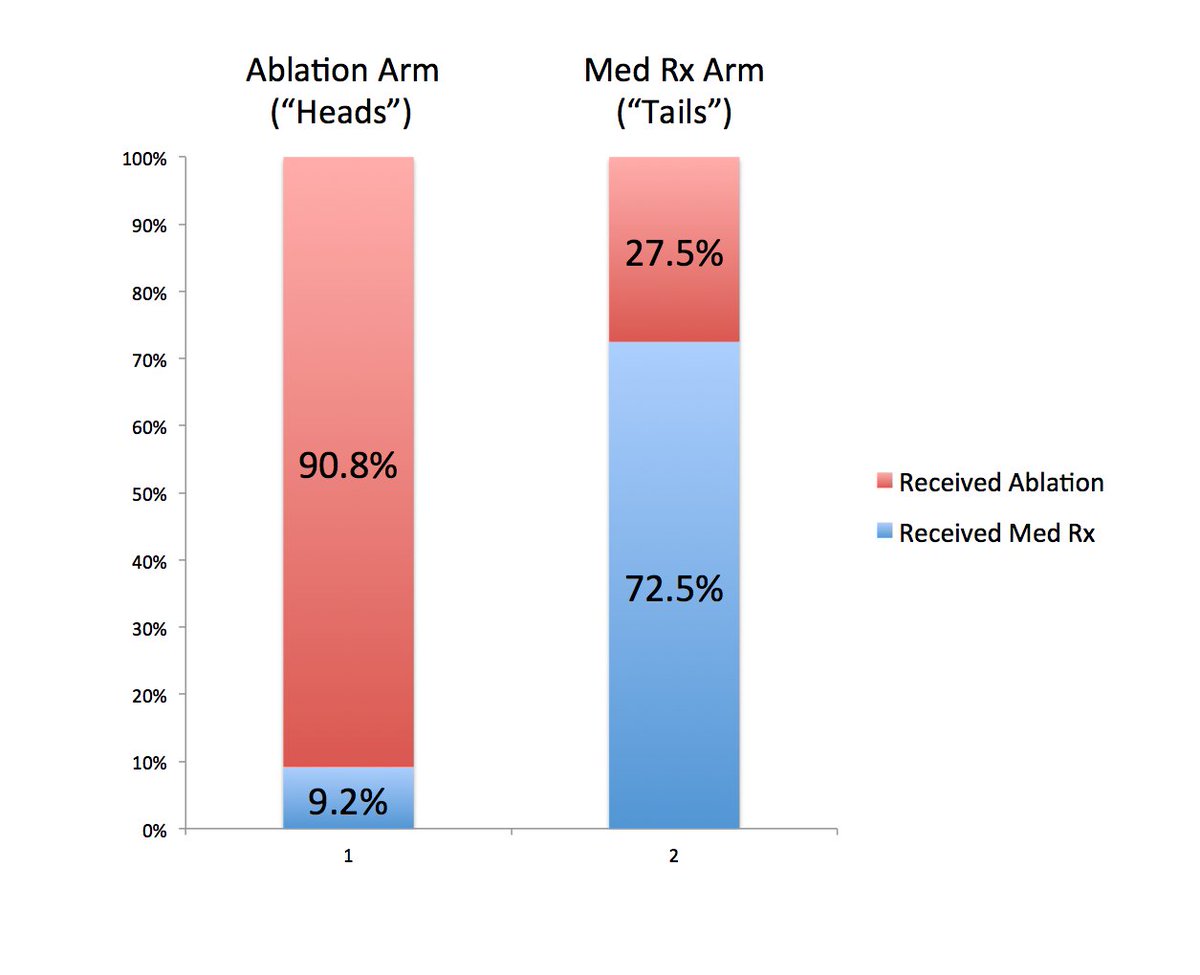
29. But beyond this CABANA gets a bit murky as different outcomes were seen looking at the ITT analysis, vs. protocol analysis, vs. Treatment received analysis. Unlike HF Trials, there was no run in period for CABANA meaning cross-overs were substantial.

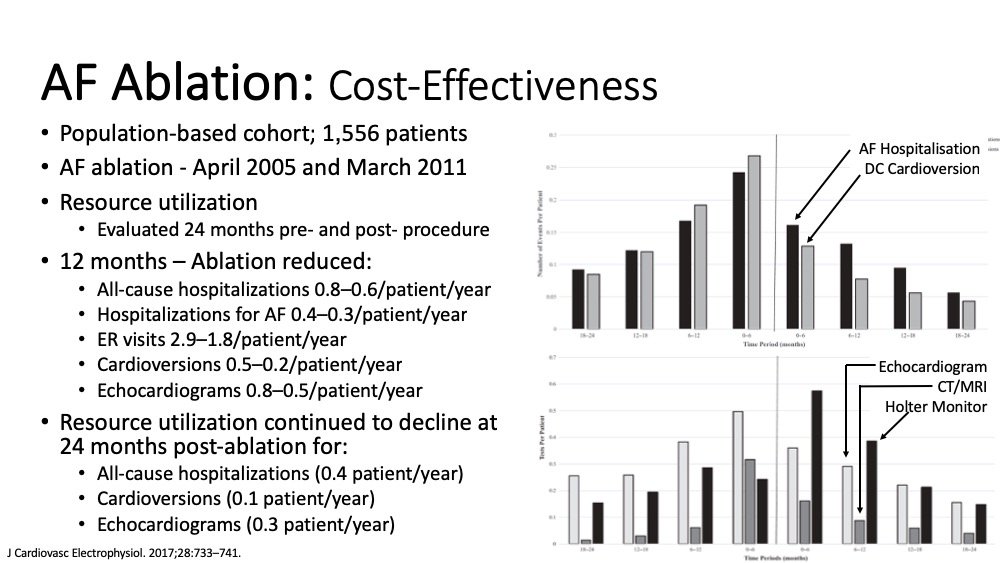
30. Last, to circle back, ablation is cost-effective. A large analysis evaluated resource utilization 24 months pre- and post- procedure. Ablation reduced ER visits, hospitalizations, and cardioversions. The only cost increase was Holter monitors, because of vigilant surveillance
31. So, to summarize:
- Ablation is better than AAD therapy (which was previously shown to be better than placebo) at reducing AF recurrence/improving quality of life.
- Ablation improves physiologic outcomes (not influenced by placebo effect)
- Ablation is cost-effective vs AAD
- Ablation is better than AAD therapy (which was previously shown to be better than placebo) at reducing AF recurrence/improving quality of life.
- Ablation improves physiologic outcomes (not influenced by placebo effect)
- Ablation is cost-effective vs AAD