,
42 tweets,
10 min read
Read on Twitter
For those unable to register for today’s webinar, I will be live tweeting developments from the National Academies meeting on quinism beginning at 1 p.m. I have shared my disappointment with the meeting organizers that registration was closed early and at the limited space here. 

One notable observation as we begin is that despite in-person registration having been closed to veterans due to capacity there are plenty of uniformed military personnel observing and plenty of empty seats. Let the record note that several veterans wished to attend but couldn’t.

Dr. Savitz has called the meeting to order. He has invited veterans to offer statements at the end, but as noted previously, online registration was closed this morning, and despite plenty of empty seats here, veterans have been told the room was full. @theNASEM.
Dr. Savitz is introducing the committee members. There are several very distinguished members present today. Our group in general appreciates the very strong credentials of this group, despite some concerns for certain manageable conflicts of interest among the group.
First up is Dr. Rumm from the VA.

Dr. Rumm acknowledges recent media attention and the concern of @TheQuinismFdn has motivated their request for this study.
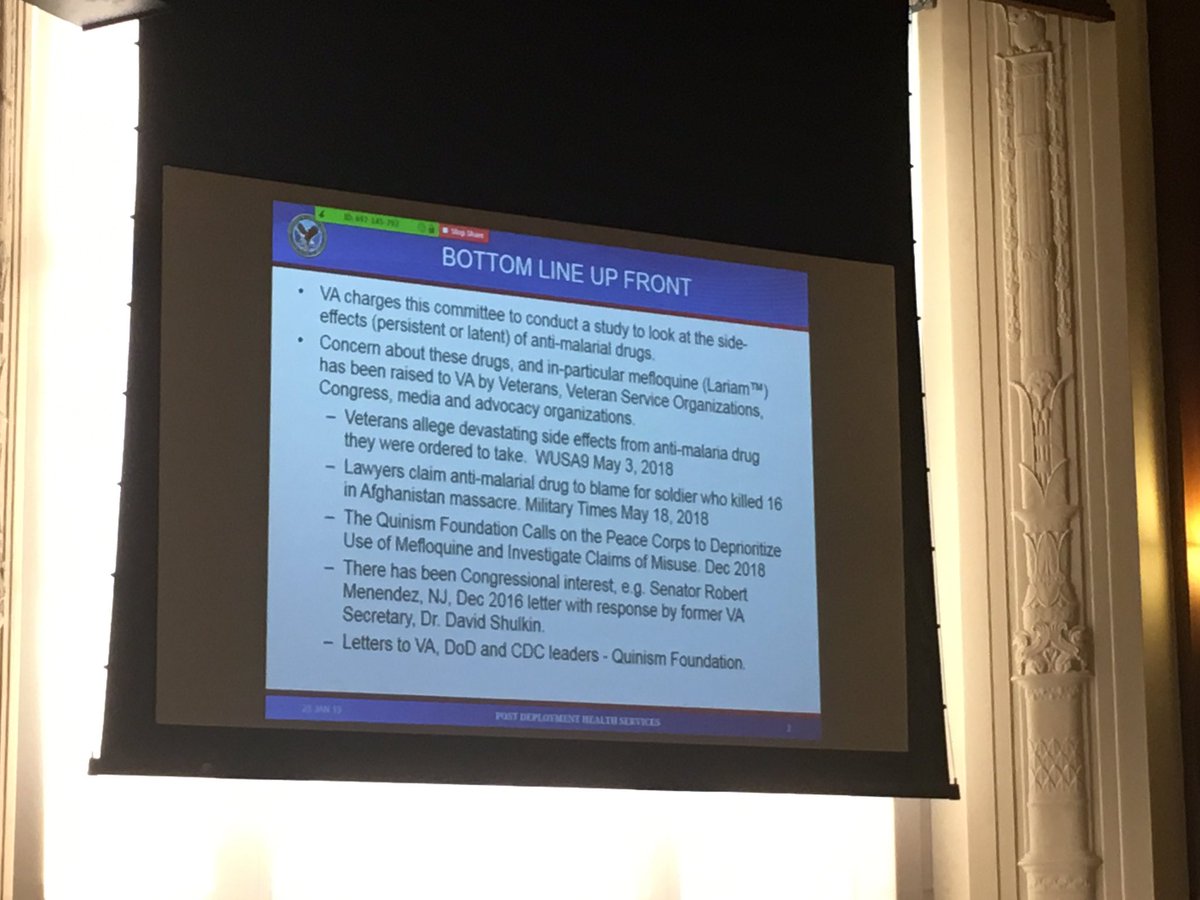
Dr. Rumm mentions the charge to the committee will include a review of tafenoquine.

Dr. Rumm hands over the lecture to Dr. Erickson briefly. His comments are a recapitulation of his recent WUSA9 interview. wusa9.com/mobile/video/n…
Dr. Stergachis asks the VA representatives about the scope of the study, and whether it should include older drugs, and a study of adverse effects at treatment doses, which he implies would be informative.
Dr. Erickson replies that the concern of the VA is primarily not in, for example, halofrantine, but in the drugs that are the subject of recent media attention. Not discussed here are the unique concerns with the quinoline drugs. Will this be the elephant in the room today?
Dr. Savitz asks the VA, essentially, to define “long-term” in regards to adverse effects. Dr. Erickson defers this to the committee’s judgement.
Dr. Stergachis has another question for the VA regarding the specific charge to the committee. Dr. Erickson notes that any recommendations from the committee will likely lead to a requirement for a particular study, hence the desire to not ask for specific recommendations.

Dr. Savitz asks for a definition of the target population. The VA responds they are primarily concerned with use of this drug in the military population, but that the broader literature may be important to assess this.

Next up is Dr. Wiesen, my former military colleague (as was Dr. Erickson). Dr. Wiesen acknowledges that he was not terribly familiar with this topic prior to recent events.

Dr. Wiesen makes clear his talk is going to emphasize the importance of antimalarial drugs to the military. This is a tired strategy; malaria is dangerous, mefloquine is effective, etc., etc. Veterans are tired of hearing this—we don’t say Agent Orange was an effective defoliant.
Quinism is definitely the elephant in the room, as Dr. Wiesen lists the various antimalarials used by the U.S. military over the years. Not mentioned: the particular concerns with quinoline neurotoxicity, which are the reason the assembled members are present today.

Dr. Wiesen is fortunately now turning his attention to the quinolines in particular. But will he discuss the neurotoxicity of this class of drug?

As expected, Dr. Wiesen completely neglects a discussion of the adverse psychiatric effects of quinacrine (Atabrine). He then briefly discusses chloroquine, and primaquine. But he again neglects a discussion of the known neurotoxicity of this drug.
Dr. Wiesen appears to have deliberately misled the committee in understating the historical use of mefloquine, claiming that it was used only as a first-line drug in limited cases and claiming incorrectly that its use was replaced with Malarone when it became available.
In fact, it took 12 years from Malarone’s widespread availability for it to replace mefloquine as DoD’s drug of choice by policy.
Troublingly, Dr. Wiesen is consistently mispronouncing “quinoline”. By his own admission, he is not the most informed speaker.
Dr. Wiesen is now explaining the game of musical chairs that underlies DoD responsibility for antimalarial policy. In essence, he is absolving Health Affairs of any oversight, and handing this off to the COCOMs and individual physicians.
Dr. Wiesen is discussing documentation of antimalarial drugs. He acknowledges that many soldiers do not have documentation of the drug they believe they took in their medical records.
Dr. Savitz asks a question of Dr. Wiesen regarding inferring exposure to certain antimalarials from location and time. Dr. Wiesen shares his anecdotal experience in being ordered to take mefloquine despite doxycycline being the drug of choice for his deployment by policy.
Committee member Dr. Wolfson asks about dispensing policy, and if servicemembers need to refill their medication in theater. Dr. Wiesen admitted that as resupply in-theater may be difficult, that servicemembers typically deploy with sufficient supplies for their entire tour.
(In so doing, Dr. Wiesen may have conceded that individuals who are not tolerating mefloquine may not be able to receive an alternative antimalarial drug, due to supply issues.)
Next to address the committee is Dr. Cao from the FDA. She will be addressing the committee by teleconference.
The FDA speaker appears to be using a standard stump speech. We will see what information specific to mefloquine the speaker discusses. The FDA’s sorry experience with this drug should be a teaching point, but I suspect this will be lost in today’s presentation.
The FDA speaker is now sharing a description of its adverse event reporting workflow using mefloquine as an example—recall that FDA first identified signals of brainstem toxicity with mefloquine in the early 2000s but waited a decade before requiring the mefloquine boxed warning.
Dr. Herman, a committee member, is asking FDA about the methods used for coding adverse event reports. Keep in mind, commiittee members are drawn from multiple disciplines, and may not have familiarity with standard pharmacovigilance methods.
Dr. Stergachis is asking several questions of FDA, including one regarding tafenoquine. FDA notes they are “very familiar” with tafenoquine safety concerns and are monitoring reports as they come in.

On break, I was quickly interviewed by @WUSA9 news for a segment that may appear tonight. Thank you to @JordanOnRecord for his consistently excellent coverage of this issue.
Next up is Dr. Tan, from @CDCtravel. I have been a consistent critic of Dr. Tan’s work and the neglect of this issue by her and her colleagues. Dr. Tan begins her speech with the typical stump speech that malaria is a deadly disease. Veterans are tired of hearing this.
Dr. Tan is boldly doubling-down on the CDC’s support for mefloquine. This is an interesting strategy.
I will be pausing my live-tweeting to prepare for my talk, which will begin in a few minutes. I am aware of problems veterans have reported with registering for the webinar. I have shared my concerns with @theNASEM in this regard and will mention this at the start of my talk.
A few minutes into her talk, Dr. Tan from @CDCtravel choked up and had difficulty speaking. Perhaps tellingly, this was during her attempts to manufacture doubts as to the dangers of mefloquine.
I will now be speaking in a few moments. Tune in to the live webinar if you are able.
I have finished my talk. For those who could not watch online, hopefully some clips will be shown by @WUSA9 in their coverage tonight and online.
Thanks to the senior officer who spoke to the committee regarding his personal experiences with mefloquine poisoning. Our group did not solicit veteran testimony as we recognize that many are unwilling or find it difficult to speak publicly on these issues.
Now speaking by telephone to the committee is Dr. Dow, the CEO of 60P. Not surprisingly, he is challenging my claims of the neurotoxicity of tafenoquine and stating that adequate safety testing of the drug has been performed. We heard this when mefloquine was first licensed.
Thanks to everyone for joining me for this live-tweeting of the meeting. Look for more comments in future days.
Thanks to @JordanOnRecord for this quick-take story on today’s events. wusa9.com/article/news/n…