,
15 tweets,
5 min read
Read on Twitter
1/
How does the drug name Sinemet (carbidopa/levodopa) provide insights into why it was developed and its mechanism of action?
I love the etymology of medication names.
Hopefully, you do too!
How does the drug name Sinemet (carbidopa/levodopa) provide insights into why it was developed and its mechanism of action?
I love the etymology of medication names.
Hopefully, you do too!
2/
Let's start with a question.
In carbidopa/levodopa, which is the "active" substance directly leading to improvement in symptoms of Parkinson disease?
Let's start with a question.
In carbidopa/levodopa, which is the "active" substance directly leading to improvement in symptoms of Parkinson disease?
3/
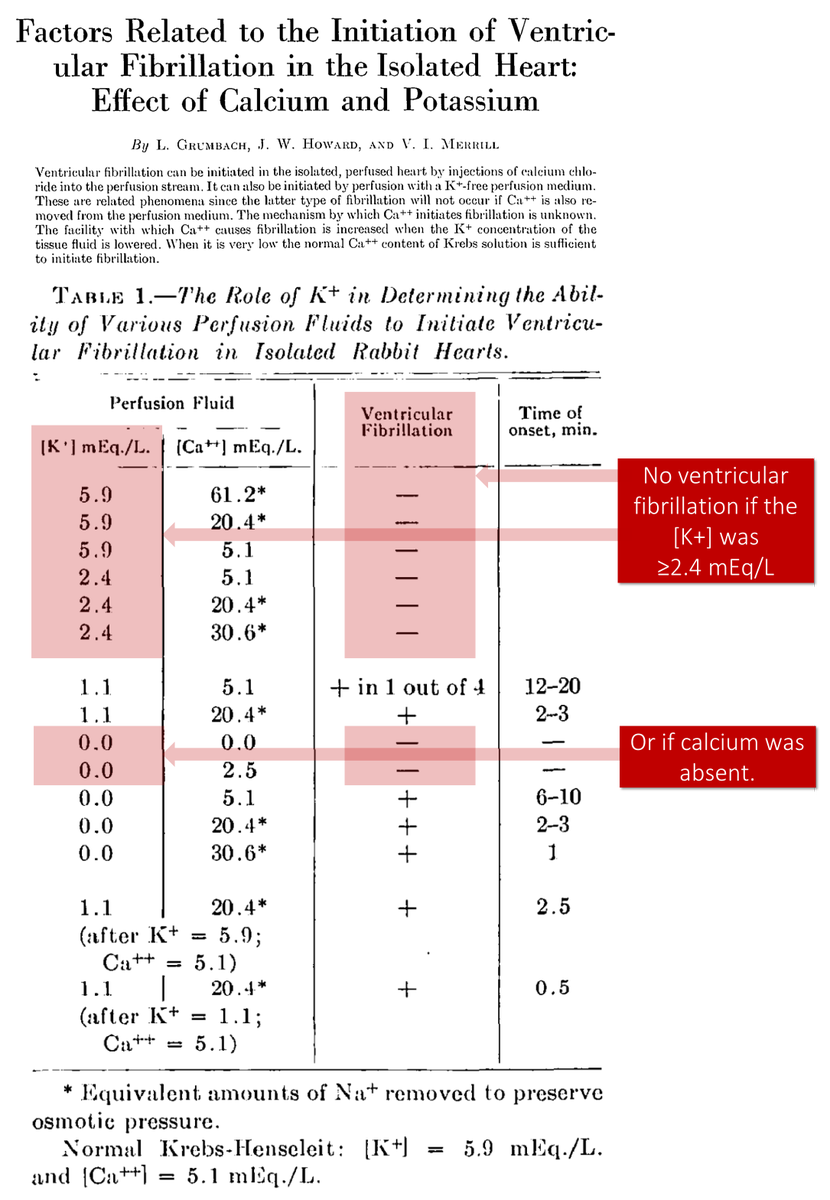
To understand the answer (neither!), we must remind ourselves of one of the lesions in Parkinson disease (PD).
In 1960, the loss of cells in the substantial nigra resulting in decreased levels of dopamine in the brain was first noted.
link.springer.com/article/10.100…
To understand the answer (neither!), we must remind ourselves of one of the lesions in Parkinson disease (PD).
In 1960, the loss of cells in the substantial nigra resulting in decreased levels of dopamine in the brain was first noted.
link.springer.com/article/10.100…
4/
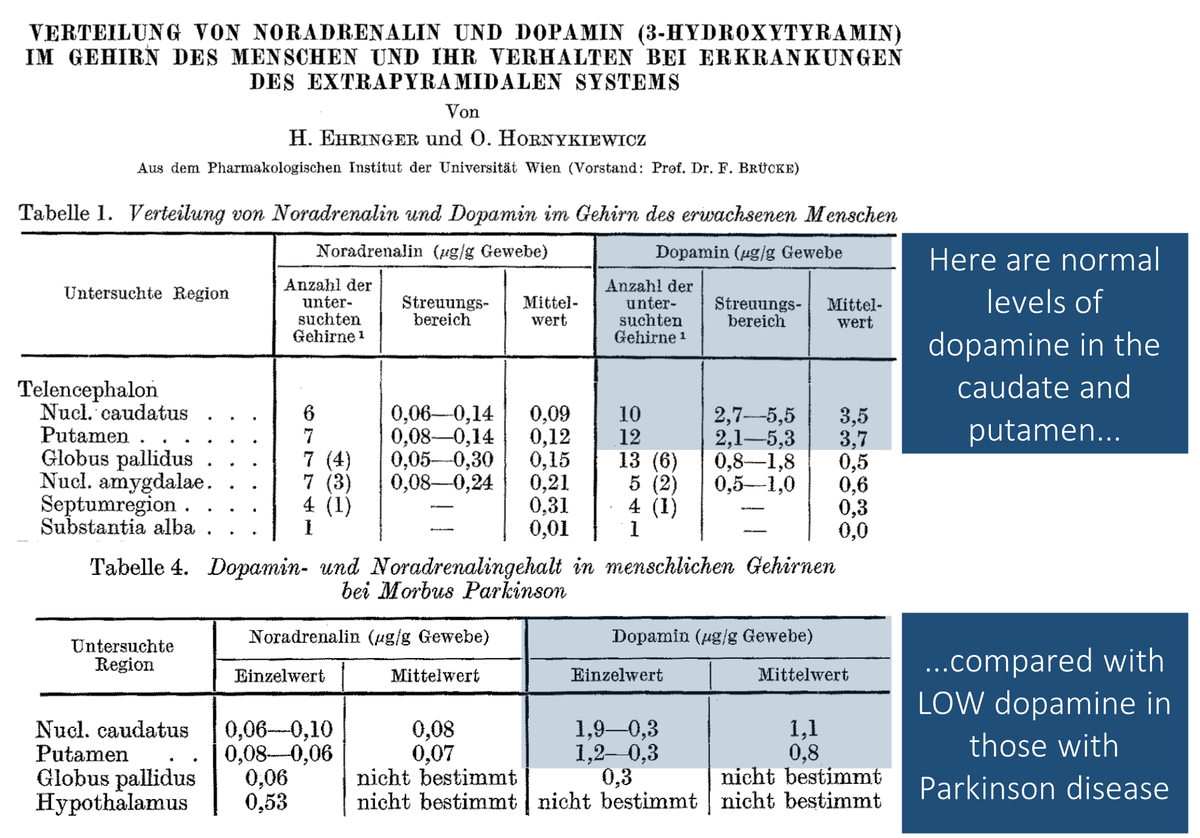
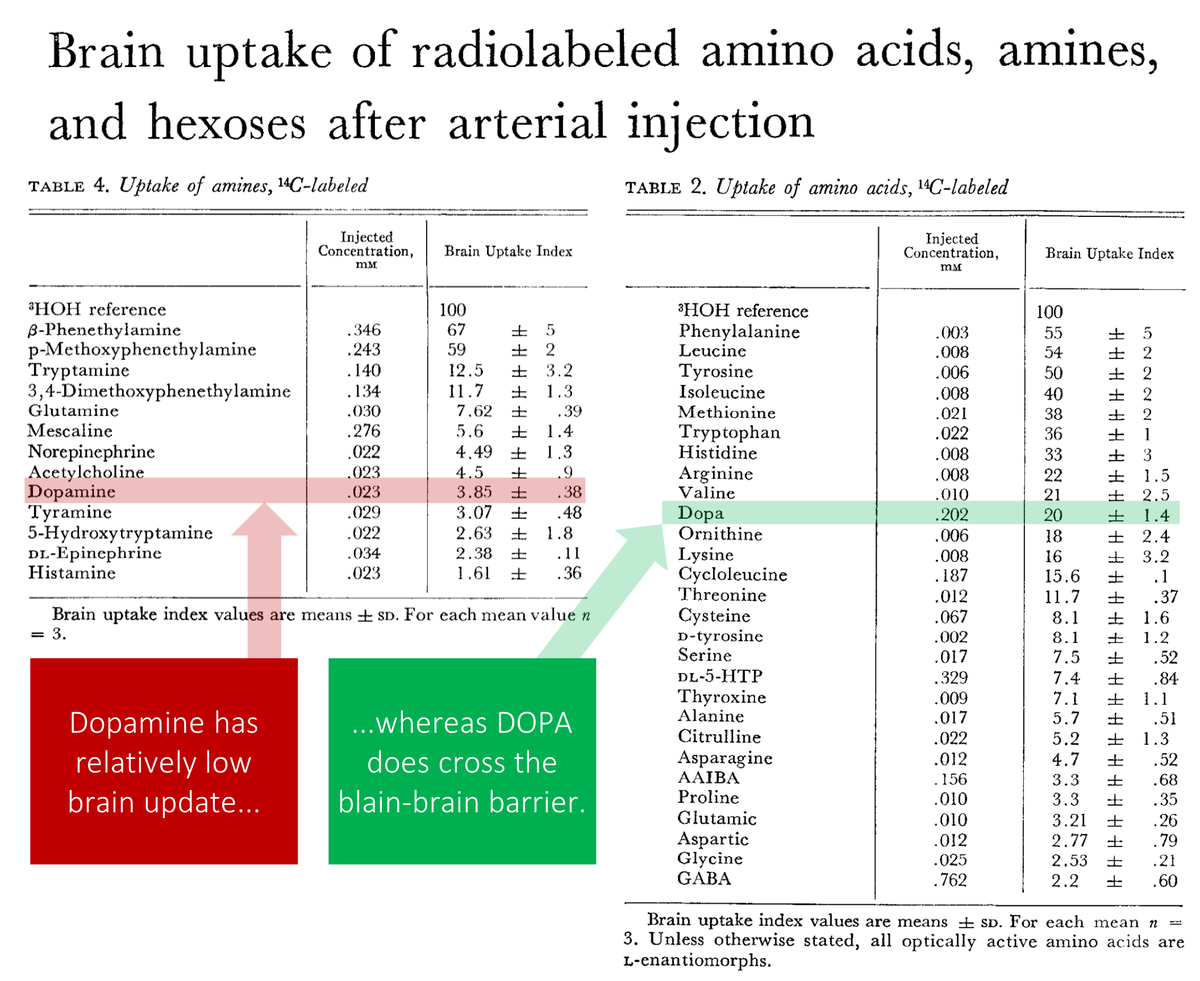
The obvious response to this finding would be to treat patients with dopamine (DA). Unfortunately, DA doesn't cross the blood-brain barrier and isn't a treatment option.
But, its precursor, dihydroxyphenylalanine (DOPA) can get into the brain!
ncbi.nlm.nih.gov/pubmed/5124307
The obvious response to this finding would be to treat patients with dopamine (DA). Unfortunately, DA doesn't cross the blood-brain barrier and isn't a treatment option.
But, its precursor, dihydroxyphenylalanine (DOPA) can get into the brain!
ncbi.nlm.nih.gov/pubmed/5124307
5/
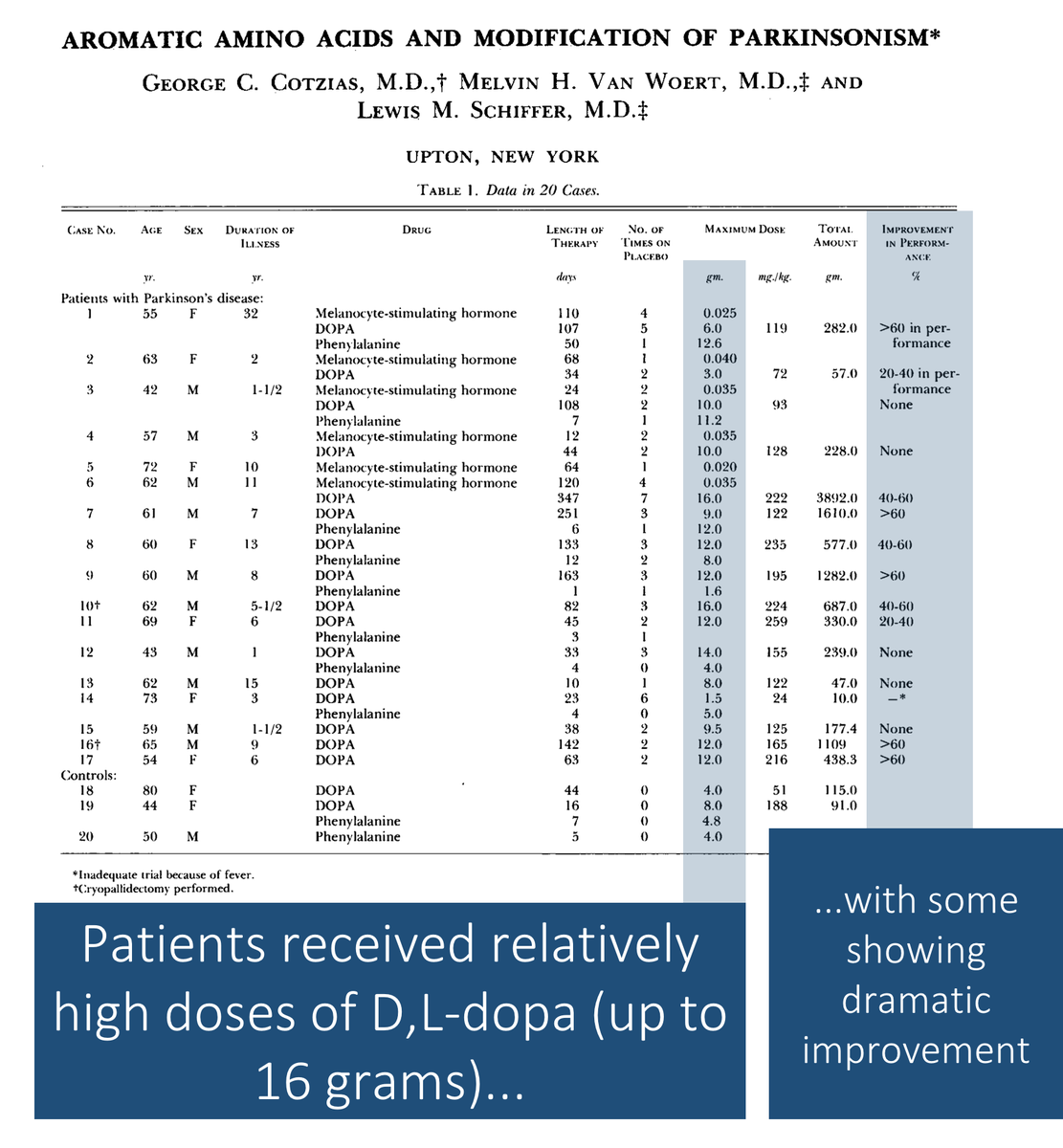
A major breakthrough came in 1967 when Cotzias showed the benefit of D,L-dopa in the treatment of PD. D,L-dopa contains both isomers of dopa.
Unfortunately, 4 of 16 patients experienced neutropenia.
ncbi.nlm.nih.gov/pubmed/5334614
A major breakthrough came in 1967 when Cotzias showed the benefit of D,L-dopa in the treatment of PD. D,L-dopa contains both isomers of dopa.
Unfortunately, 4 of 16 patients experienced neutropenia.
ncbi.nlm.nih.gov/pubmed/5334614
6/
Next, we learned that L-dopa is the active isomer, allowing its administration without D-dopa (the likely culprit for the leukopenia).
This introduced us to levodopa (the "levo" referring to "levorotation", the chirality of this isomer).
ncbi.nlm.nih.gov/pubmed/4178641
Next, we learned that L-dopa is the active isomer, allowing its administration without D-dopa (the likely culprit for the leukopenia).
This introduced us to levodopa (the "levo" referring to "levorotation", the chirality of this isomer).
ncbi.nlm.nih.gov/pubmed/4178641
7/
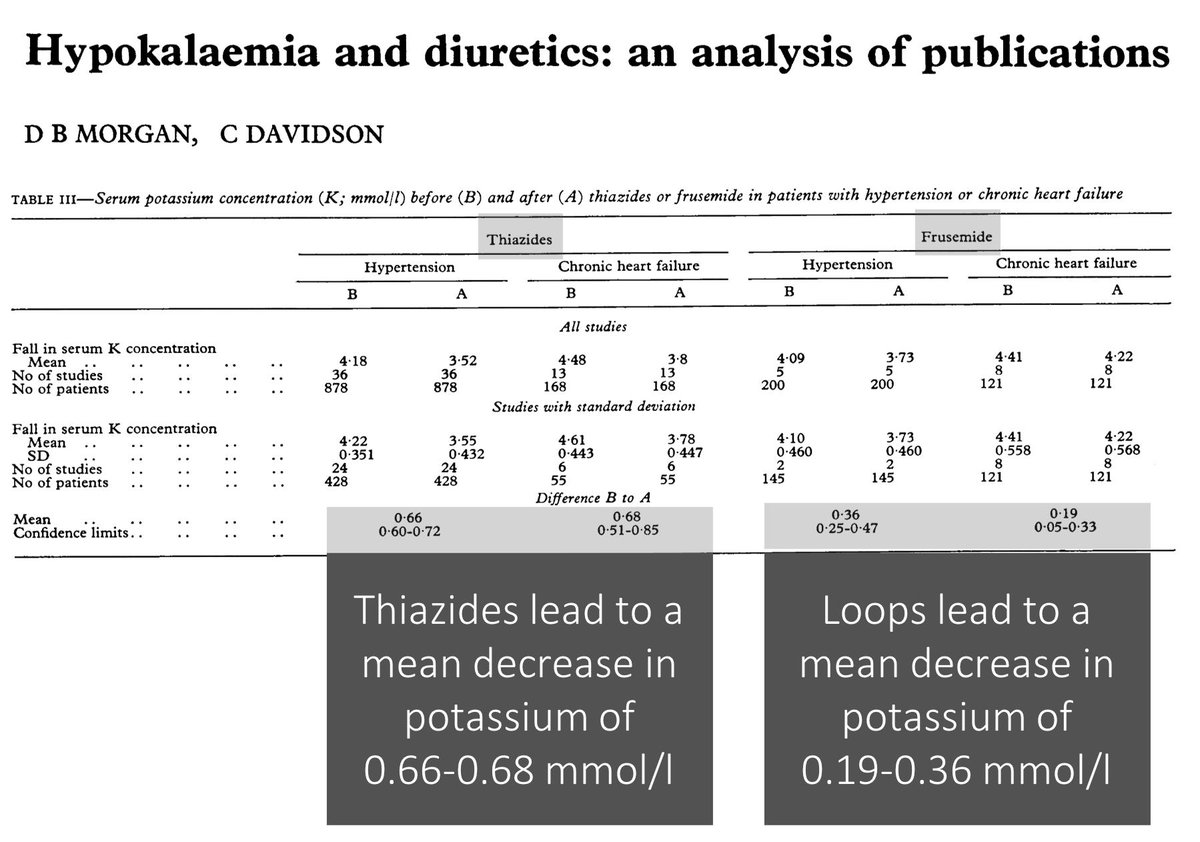
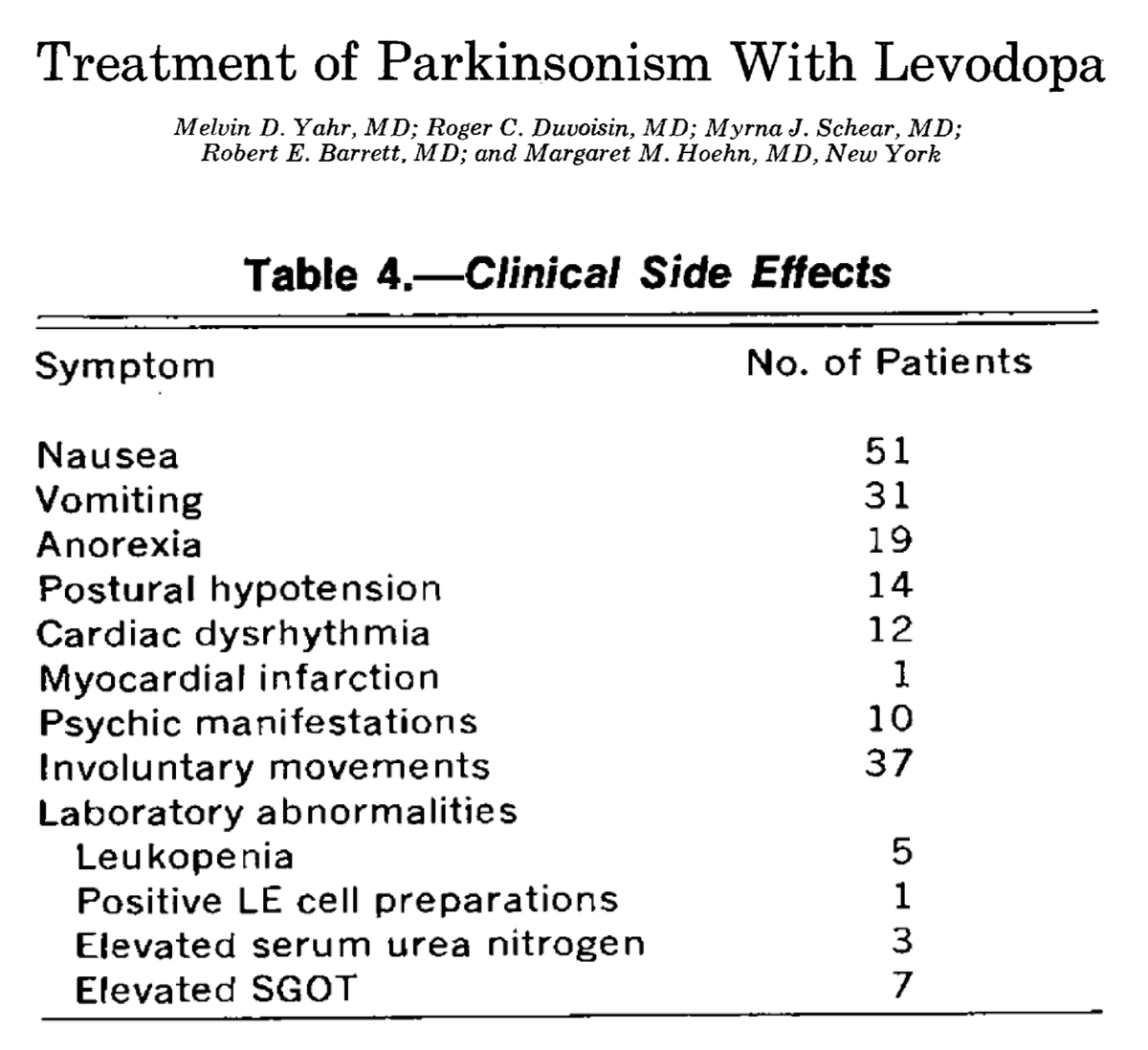
Though progress was being made, the ability to escalate doses to maximize therapeutic benefit was limited by GI side effects.
For example, one study of L-dopa reported:
91% nausea
55% vomiting
34% anorexia
ncbi.nlm.nih.gov/pubmed/5820999
Though progress was being made, the ability to escalate doses to maximize therapeutic benefit was limited by GI side effects.
For example, one study of L-dopa reported:
91% nausea
55% vomiting
34% anorexia
ncbi.nlm.nih.gov/pubmed/5820999
8/
L-dopa is largely inert. Its effects in PD derive from the fact that it:
1. crosses the blood-brain barrier
2. is converted to dopamine (DA) in the brain
BUT, L-dopa is also converted to DA peripherally. This leads to GI side effects.
And, where does DA act to cause nausea?
L-dopa is largely inert. Its effects in PD derive from the fact that it:
1. crosses the blood-brain barrier
2. is converted to dopamine (DA) in the brain
BUT, L-dopa is also converted to DA peripherally. This leads to GI side effects.
And, where does DA act to cause nausea?
9/
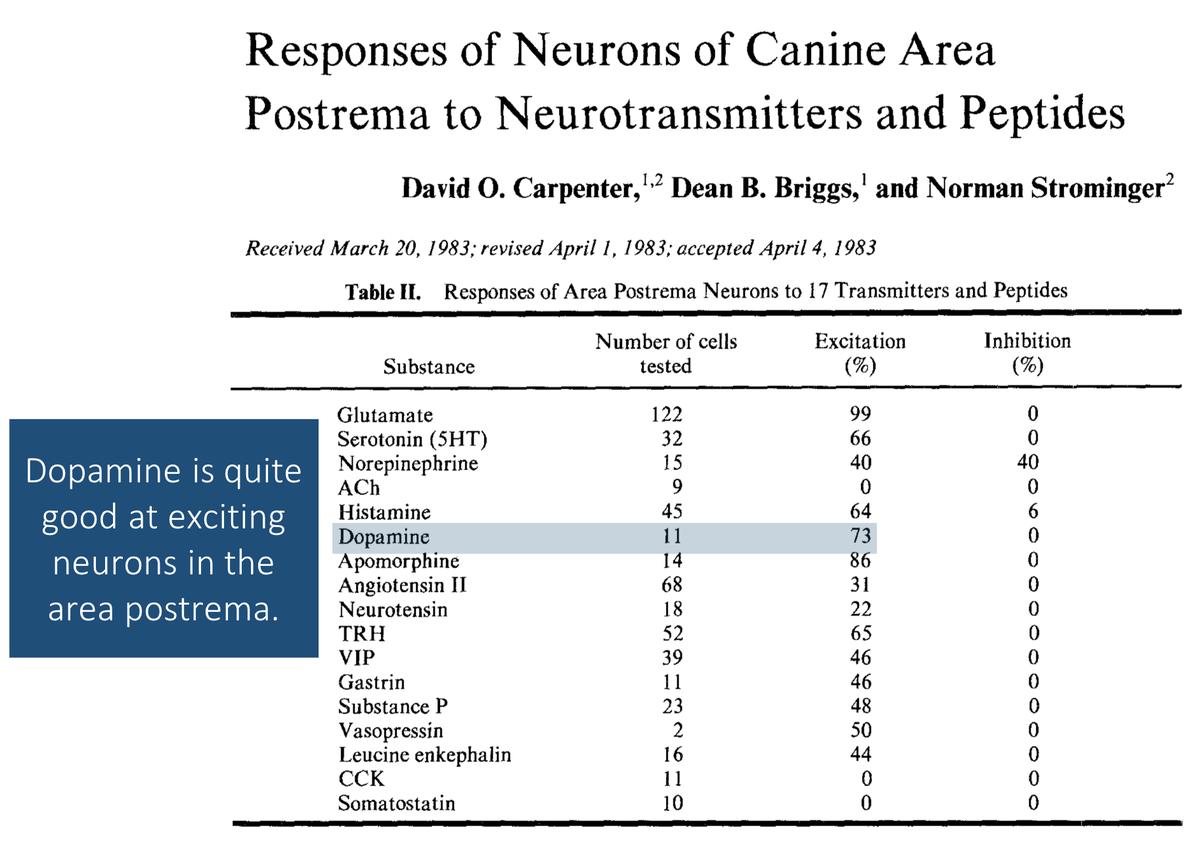
After taking L-dopa, some is converted to DA peripherally. This activates receptors in the area postrema in the medulla causing nausea.
But, if the postrema is in the brain and DA can't cross the blood-brain barrier, how can PERIPHERAL conversation of L-dopa cause nausea?
After taking L-dopa, some is converted to DA peripherally. This activates receptors in the area postrema in the medulla causing nausea.
But, if the postrema is in the brain and DA can't cross the blood-brain barrier, how can PERIPHERAL conversation of L-dopa cause nausea?
10/
Here's the cool explanation:
The area postrema sits OUTSIDE the blood-brain barrier and therefore can be reached by peripheral DA.
In fact, one role of this structure is to sense bloodstream toxins and cause us to vomit!
ncbi.nlm.nih.gov/pubmed/6140078
Here's the cool explanation:
The area postrema sits OUTSIDE the blood-brain barrier and therefore can be reached by peripheral DA.
In fact, one role of this structure is to sense bloodstream toxins and cause us to vomit!
ncbi.nlm.nih.gov/pubmed/6140078
11/
How would you address the problem of peripheral conversion of L-dopa to dopamine?
Fortunately, there is a drug that inhibits DOPA decarboxylase, the enzyme that converts L-dopa to dopamine...
...CARBIDOPA!
How would you address the problem of peripheral conversion of L-dopa to dopamine?
Fortunately, there is a drug that inhibits DOPA decarboxylase, the enzyme that converts L-dopa to dopamine...
...CARBIDOPA!

12/
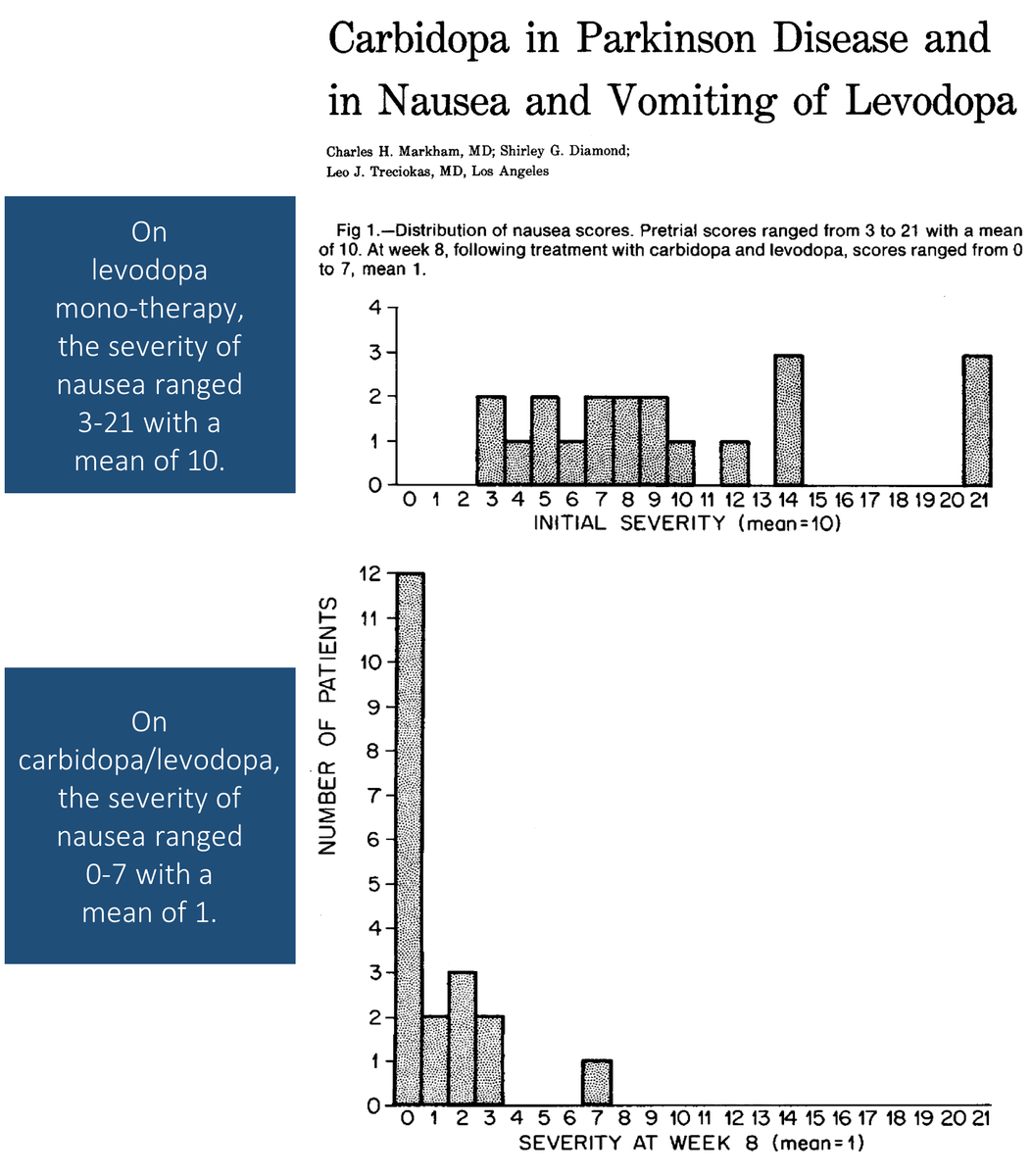
Trials suggest that if you administer carbidopa with L-dopa, the rates of nausea decrease dramatically.
And, because carbidopa can't cross the blood-brain barrier, it doesn't decrease brain DA levels.
ncbi.nlm.nih.gov/pubmed/4834974
Trials suggest that if you administer carbidopa with L-dopa, the rates of nausea decrease dramatically.
And, because carbidopa can't cross the blood-brain barrier, it doesn't decrease brain DA levels.
ncbi.nlm.nih.gov/pubmed/4834974
13/
The namers of this new combination medication made reference to the added benefit of carbidopa added to L-dopa (levodopa).
SINE (without)
+
EMET (vomiting)
=
SINEMET
The namers of this new combination medication made reference to the added benefit of carbidopa added to L-dopa (levodopa).
SINE (without)
+
EMET (vomiting)
=
SINEMET
14/
Before summarizing, here is the original question one more time.
In carbidopa/levodopa, which is the "active" substance directly leading to improvement in symptoms of Parkinson disease?
Before summarizing, here is the original question one more time.
In carbidopa/levodopa, which is the "active" substance directly leading to improvement in symptoms of Parkinson disease?
15/SUMMARY
✔️Parkinson disease partly results from decreased brain dopamine (DA)
✔️L-dopa (levodopa) is inert but is converted to DA, treating symptoms
✔️Carbidopa decreases peripheral conversion of L-dopa to DA
✔️This mitigates nausea seen with L-dopa monotherapy
✔️Parkinson disease partly results from decreased brain dopamine (DA)
✔️L-dopa (levodopa) is inert but is converted to DA, treating symptoms
✔️Carbidopa decreases peripheral conversion of L-dopa to DA
✔️This mitigates nausea seen with L-dopa monotherapy