,
14 tweets,
3 min read
Read on Twitter
1/
Why do thiazide diuretics cause more hypokalemia than loop diuretics?
Loops DIRECTLY affect potassium (via inhibition of the Na-K-2Cl co-transporter), while thiazides affect the Na-Cl co-transporter (no K!)
And yet, thiazides cause more hypokalemia.
Let's find out why.
Why do thiazide diuretics cause more hypokalemia than loop diuretics?
Loops DIRECTLY affect potassium (via inhibition of the Na-K-2Cl co-transporter), while thiazides affect the Na-Cl co-transporter (no K!)
And yet, thiazides cause more hypokalemia.
Let's find out why.
2/
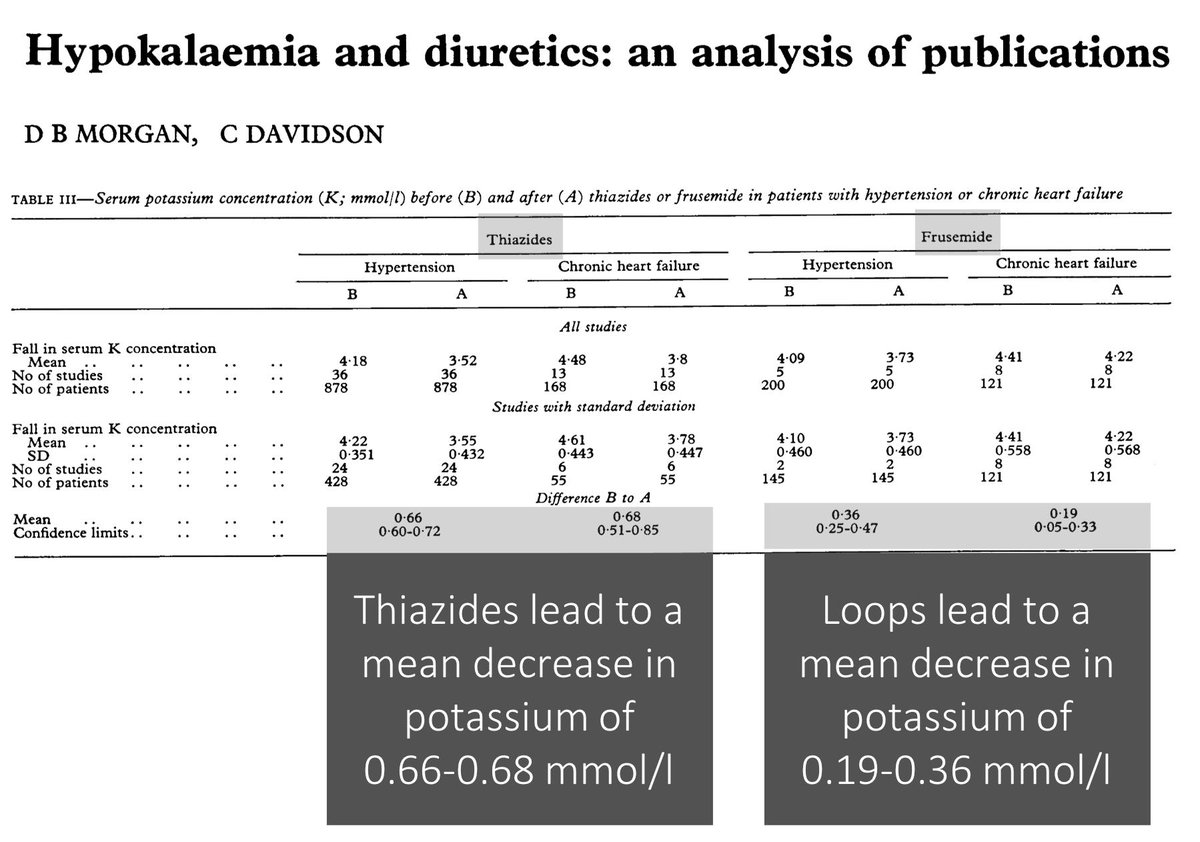
Before moving on, let's first establish that thiazides do, in fact, cause more hypokalemia.
One study reported the following decrease in serum potassium for each diuretic type:
*thiazides = 0.66-0.68 mEq/L
*furosemide = 0.19-0.36 mEq/L
ncbi.nlm.nih.gov/pubmed/7388366
Before moving on, let's first establish that thiazides do, in fact, cause more hypokalemia.
One study reported the following decrease in serum potassium for each diuretic type:
*thiazides = 0.66-0.68 mEq/L
*furosemide = 0.19-0.36 mEq/L
ncbi.nlm.nih.gov/pubmed/7388366
3/
What explains this finding?
What is different about thiazides (when compared with loop diuretics like furosemide) that leads to increased potassium excretion and resulting hypokalemia?
What explains this finding?
What is different about thiazides (when compared with loop diuretics like furosemide) that leads to increased potassium excretion and resulting hypokalemia?
4/
To understand the answer, we must first review how thiazides lead to hypokalemia.
Recall that their site of action is the apical Na-Cl cotransporter (NCC). Inhibition of NCC decreases Na reabsorption in the distal convoluted tubule.
Again: K is not directly affected.
To understand the answer, we must first review how thiazides lead to hypokalemia.
Recall that their site of action is the apical Na-Cl cotransporter (NCC). Inhibition of NCC decreases Na reabsorption in the distal convoluted tubule.
Again: K is not directly affected.
5/
The Na that has NOT been reabsorbed is delivered to the collecting tubules where it is reabsorbed via ENaC. This does two things:
*Increases basolateral Na-K-ATPase activity, shifting K into cells
*Creates a lumen-negative driving force for K secretion into the tubule
The Na that has NOT been reabsorbed is delivered to the collecting tubules where it is reabsorbed via ENaC. This does two things:
*Increases basolateral Na-K-ATPase activity, shifting K into cells
*Creates a lumen-negative driving force for K secretion into the tubule
6/
The resulting volume depletion also activates aldosterone which stimulates apical ENaC channels and basolateral Na-K-ATPase pumps, fueling K secretion.
The resulting volume depletion also activates aldosterone which stimulates apical ENaC channels and basolateral Na-K-ATPase pumps, fueling K secretion.
7/
This explanation generates a hypothesis and question.
Maybe whichever diuretic causes more distal Na delivery also causes more hypokalemia.
So, which diuretic leads to more distal Na delivery?
This explanation generates a hypothesis and question.
Maybe whichever diuretic causes more distal Na delivery also causes more hypokalemia.
So, which diuretic leads to more distal Na delivery?
8/
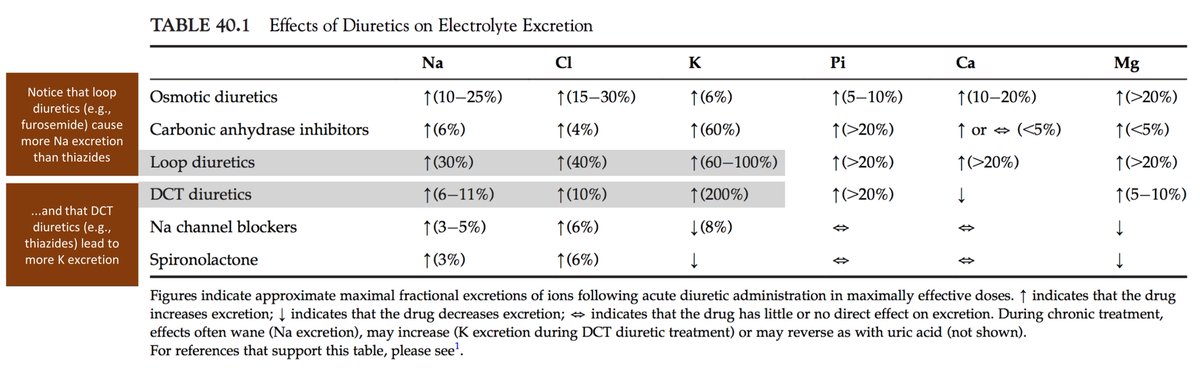
Loop diuretics cause more distal Na delivery. This should come as no surprise given that they are our diuretic of choice when we want to actually diurese...
But, this removes another explanation for why thiazides cause more hypokalemia.
sciencedirect.com/science/articl…
Loop diuretics cause more distal Na delivery. This should come as no surprise given that they are our diuretic of choice when we want to actually diurese...
But, this removes another explanation for why thiazides cause more hypokalemia.
sciencedirect.com/science/articl…
9/
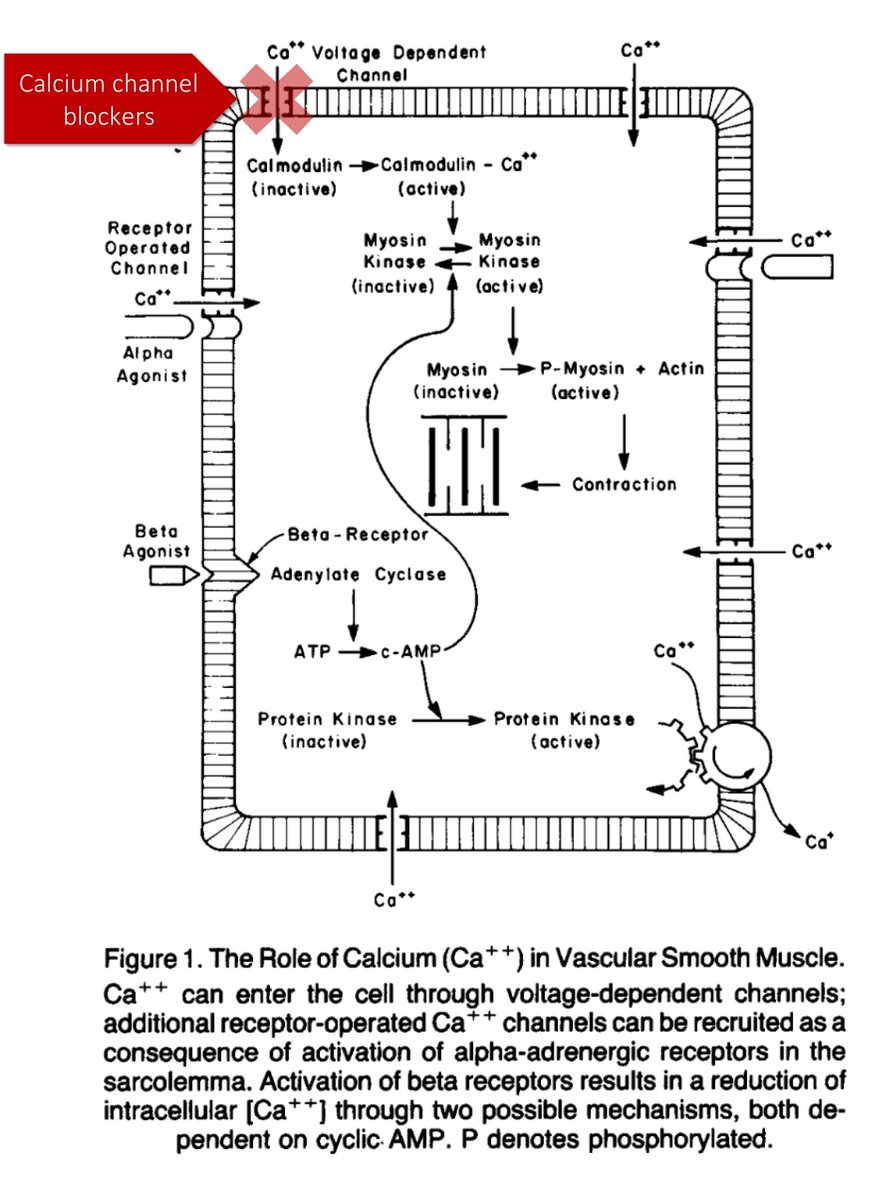
While both loop diuretics and thiazides lead to decreased Na reabsorption, they have opposite effects on another cation...
...CALCIUM
And its the handling of Ca that likely contributes to the difference in rates of hypokalemia.
While both loop diuretics and thiazides lead to decreased Na reabsorption, they have opposite effects on another cation...
...CALCIUM
And its the handling of Ca that likely contributes to the difference in rates of hypokalemia.
10/
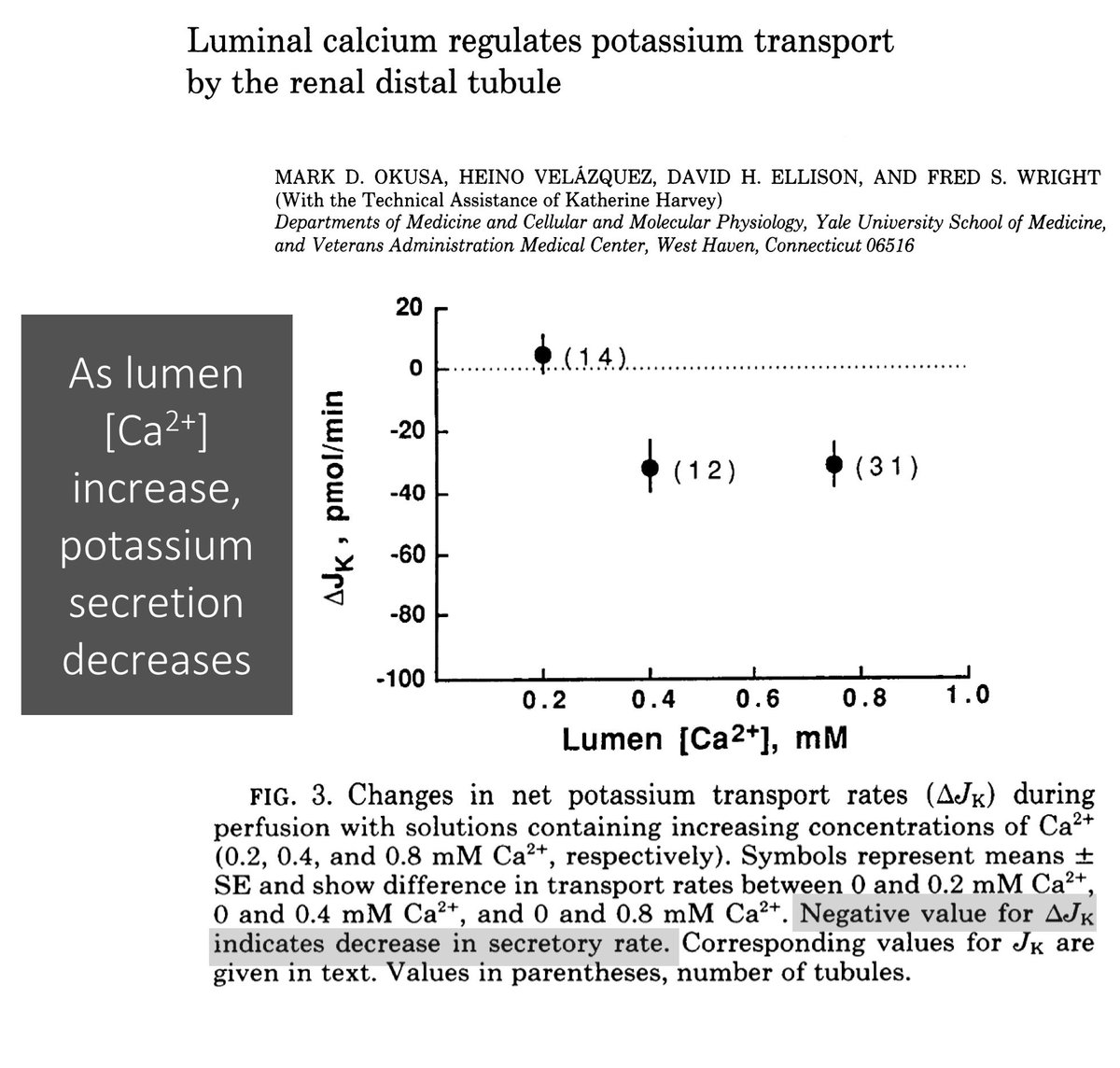
In 1980, the effect on calcium on K secretion was demonstrated. Okusa et al showed that as luminal [Ca] increases, K secretion decreases.
The higher [Ca] is delivered distally and reduces the lumen-negative driving force for potassium excretion!
ncbi.nlm.nih.gov/pubmed/2309896
In 1980, the effect on calcium on K secretion was demonstrated. Okusa et al showed that as luminal [Ca] increases, K secretion decreases.
The higher [Ca] is delivered distally and reduces the lumen-negative driving force for potassium excretion!
ncbi.nlm.nih.gov/pubmed/2309896
11/
So, whichever class of diuretic leads to LESS distal calcium delivery should cause MORE potassium secretion and more hypokalemia.
As you may recall, loops cause more calcium excretion, which is one reason they are used to treat hypercalcemia.
So, whichever class of diuretic leads to LESS distal calcium delivery should cause MORE potassium secretion and more hypokalemia.
As you may recall, loops cause more calcium excretion, which is one reason they are used to treat hypercalcemia.
12/
And, thiazides cause LESS calcium excretion.
Result: thiazides cause more K secretion than loop diuretics and more hypokalemia!
Note: there are likely other mechanisms (e.g., activation of maxi-K channels) that contribute to the different rates of hypokalemia.
And, thiazides cause LESS calcium excretion.
Result: thiazides cause more K secretion than loop diuretics and more hypokalemia!
Note: there are likely other mechanisms (e.g., activation of maxi-K channels) that contribute to the different rates of hypokalemia.
13/
Before closing, let's ask the original question once more:
What is different about thiazides (when compared with loop diuretics like furosemide) that leads to increased potassium excretion and resulting hypokalemia?
Before closing, let's ask the original question once more:
What is different about thiazides (when compared with loop diuretics like furosemide) that leads to increased potassium excretion and resulting hypokalemia?
14/SUMMARY
✔️Although loop diuretics cause more distal Na delivery, and
✔️Distal Na delivery is a key driver of K secretion,
✔️Thiazides cause more K secretion (and hypokalemia), given that they
✔️Decrease distal Ca delivery
✔️Although loop diuretics cause more distal Na delivery, and
✔️Distal Na delivery is a key driver of K secretion,
✔️Thiazides cause more K secretion (and hypokalemia), given that they
✔️Decrease distal Ca delivery