,
16 tweets,
6 min read
Read on Twitter
[nervously taps the #medtwitter mic] Hi, is this thing on?
Feeling inspired by amazing tweetorials from @david_furfaro @DxRxEdu @AmitGoyalMD @JohnsHopkinsDOM, I thought I might take a stab at my own first ever tweetorial!!!!! #traineetutorial
THREAD:
1/
Feeling inspired by amazing tweetorials from @david_furfaro @DxRxEdu @AmitGoyalMD @JohnsHopkinsDOM, I thought I might take a stab at my own first ever tweetorial!!!!! #traineetutorial
THREAD:
1/
The case: A 54-year old male bus driver with multiple DVTs & PEs on anticoagulation & financial barriers to medication adherence
presented with subacute progressive dyspnea and
lower extremity edema. 2/
presented with subacute progressive dyspnea and
lower extremity edema. 2/
Physical exam was notable for hypoxia requiring 4 L O2, elevated JVP and pitting lower extremity edema. Labs showed troponin <0.04 and pro-BNP of 1428. 3/
This was his ECG. What key abnormalities do you see? [Hint, note leads I, III, V1 and precordial leads!] 4/ 
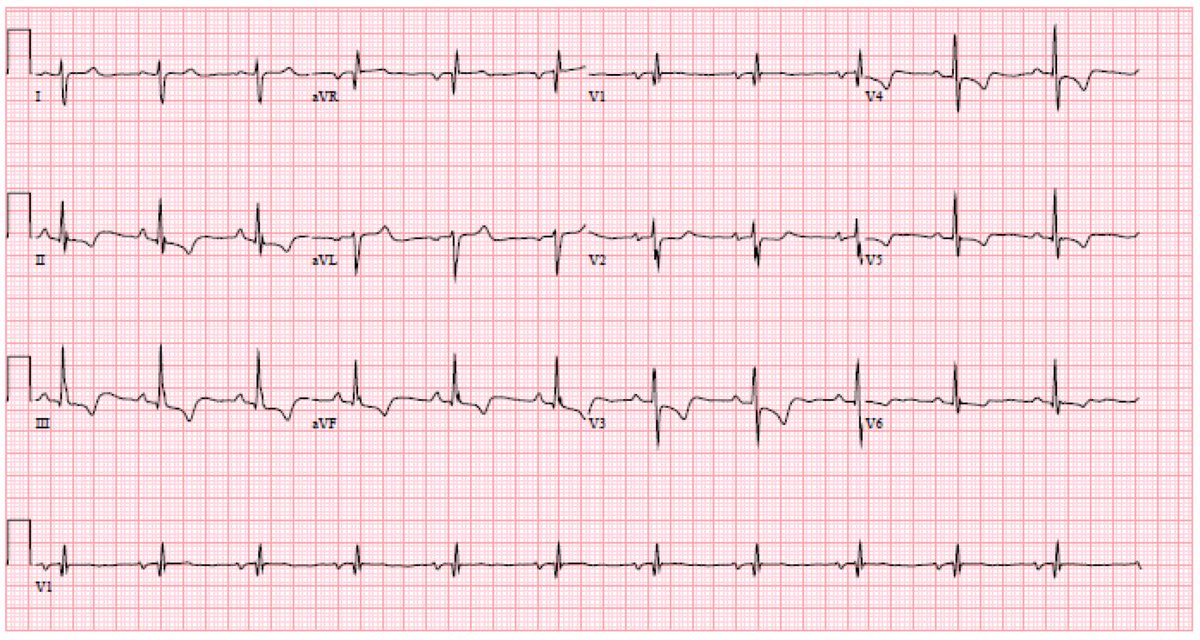
His ECG revealed features suggestive of right heart strain, including right axis
deviation, R>S in V1, S1Q3T3 and precordial T wave
inversions. What diagnosis is the S1Q3T3 ECG pattern frequently associated with (although we rarely ever see it in real life)? Next study? 5/
deviation, R>S in V1, S1Q3T3 and precordial T wave
inversions. What diagnosis is the S1Q3T3 ECG pattern frequently associated with (although we rarely ever see it in real life)? Next study? 5/
A chest CTA was obtained. It was negative for acute PE but showed bilateral peripheral pulmonary artery (PA) filling defects with distal branch attenuation and parenchymal mosaic attenuation concerning for chronic PE. 6/

We then obtained a transthoracic echo. What stands out to you here? 7/

The echo revealed a dilated hypokinetic right ventricle (RV) and elevated RV systolic pressure (103 mmHg) indicative of severe PHTN. The patient subsequently underwent extensive diuresis until he was euvolemic. A right cath was performed and showed the following... 8/

RHC showed normal right heart filling pressure (RA mean 3 mmHg), elevated PA pressure (105/36, mean 53 mmHg), low pulmonary capillary wedge pressure (4
mmHg and elevated pulmonary vascular resistance (10.7 Wood units), thus confirming the diagnosis of precapillary PHTN. 9/
mmHg and elevated pulmonary vascular resistance (10.7 Wood units), thus confirming the diagnosis of precapillary PHTN. 9/
But wait, there's more! Out of concern for chronic thromboembolism, a VQ scan was obtained. Ventilation defects are on left. Perfusion defects are on the right. Note widespread perfusion defects & mismatch with ventilation defects, indicating high probability of chronic PE. 10/


Last, a PA angiogram was obtained & demonstrated enlarged PAs with
peripheral pruning, thus confirming the diagnosis of
chronic thrombembolic pulmonary hypertension (CTEPH) causing group 4 pulmonary hypertension (PHTN). 11/
peripheral pruning, thus confirming the diagnosis of
chronic thrombembolic pulmonary hypertension (CTEPH) causing group 4 pulmonary hypertension (PHTN). 11/


Extensive hypercoagulability testing was unrevealing; the patient's occupation as a bus driver was felt to be his prevailing risk factor. He was discharged on
furosemide, warfarin and oxygen. He was referred to a
CTEPH center for evaluation and management. 12/
furosemide, warfarin and oxygen. He was referred to a
CTEPH center for evaluation and management. 12/
This is a prototypical presentation of advanced CTEPH with severe group 4 PHTN! Early dx is KEY given dire natural history of untreated disease and advent of effective treatment. High index of suspicion & multimodal diagnostics (TTE, VQ >> CT scan, RHC, PA angiography) needed!
A multidisciplinary specialists (pulmonologists, IR, thoracic surgeons) are needed to determine best course of treatment. Treatment options: pulmonary thromboendarterectomy (definitive therapy/CURE), percutaneous balloon pulmonary angioplasty and pulmonary vasodilators! 14/
Final takeaway: CTEPH is often overlooked until patients experience respiratory
and right heart impairment. Early diagnosis and treatment is key as CTEPH/group 4 PHTN may be CURABLE, unlike other causes of PHTN. Fin/
and right heart impairment. Early diagnosis and treatment is key as CTEPH/group 4 PHTN may be CURABLE, unlike other causes of PHTN. Fin/
Thanks to some guidance from my wonderful ACS (chief resident) @AmitGoyalMD, I was able to put it all together into a poster and presented the case at the Maryland ACP conference today. Shout out to @mikemorrison for the #betterposter format (albeit with some modifications)!