
,
26 tweets,
8 min read
Read on Twitter
Last week, there was renewed interest in the media about maternal mortality. As a guy who helps lead our #cardiacobstetrics prog @MdAtlPermanente I am deeply invested in making maternal mortality as low as possible - b/c a maternal mortality=a kid growing up without a mom. (1/x)
So I wanted to understand the data driving the conversation. Boy was I surprised by what I found. Let me tell you why, in a thread (2/x)
First the headlines. The crux of the headlines was threefold. 1) maternal mortality is higher in the US than any other developed country 2) there are significant racial disparities in mortality rates & 3) the leading cause of maternal mortality is cardiovascular disease. (3/x)
So is maternal mortality higher? Well if you look that the topline data it would seem so. US rates are reported between 17.2 and 26.4 deaths per 100K live births, compared to 6.6 in the UK or 3.7 in Spain. (source oecd.stat). (4/x)
When you look at the raw numbers though this translates to between 700 to 800 maternal deaths per year ACROSS the US. That the raw number is so low matters because small errors in data acquisition could have big effects on the reported rate. So how do we calculate the rate? (5/x)
In the US, we use a question on death certificates to trigger an analysis. This is then correlated with birth or fetal death certificate to try to verify the results. (source MMRIA committee report) (6/x) 

Unfortunately though, very few states had this question on their death certificate until 2002, and even as late as 2015, it did not appear in some states death certificates. Here's a chart showing the state revision policies by state. (ncbi.nlm.nih.gov/pmc/articles/P…) (7/x)
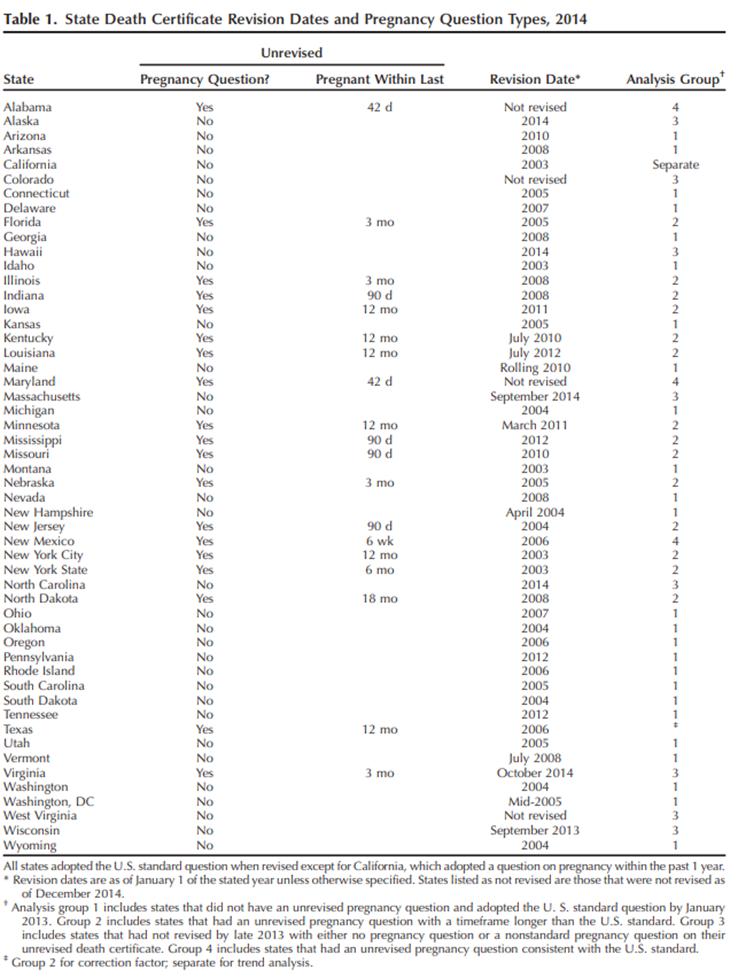
You may say this has the poss of both under- and over- estimating true incidence of maternal mort. And you would be right. (8/x)
But when the # are very small (700 deaths out a total 2.7 million per year on average in the US), the risk of a small error rate having huge effects is high in both directions. An overstimate of 350 death certificates (of 2.7 million) would put us in line with other OECDs. (9/x)
But the error rate can't be that high, can it? Well its difficult to say because granular data is not always available (and the false negative rate is difficult to ascertain). One report (MMRIA cdcfoundation.org/sites/default/…) attempted to study this question. (10/x)
They looked at data from 4 states (Colorado 2008-12, Delaware (2009-14), Geogia (2012-13), and Ohio (2008-12)). They did deep dives into the causes of death. Its really a great report and worth reading cover to cover. What did they find? (11/x)
Of the 650 deaths, 97 had no evidence of pregnancy within the year prior. So 15% of the reported deaths were false positives. But what about the other 553? These were separated into preg-related and preg-associated but not related. (an attempt to understand causality) (12/x)

Of the 553 pregnancy-associated deaths, only 175 were determined to be pregnancy-related. If only pregnancy related deaths were included in the OECD metric, the rate would be 5.8/100K, similar to other OECD countries (13/x)

Of course, this is an unfair comparison, b/c there is great variation in how maternal death is measured and calculated across the world. But it shows the risks of comparing a low incidence condition with varying methods and challenging data collection to influence policy. (14/x)
You may say that the MMWR report from this year adjudicates for preg-related death (excluding all the others). And you are right. But even that dataset, 12.8% (420/3410) excluded b/c timing couldn't be determined, suggesting a FP rate in that dataset as well. (15/x)

Ok so we are unsure about the measurement. What about the racial disparities? Are there disparities by race (as noted on the death certificate) among those deaths determined to be pregnancy-related? The answer is, unfortuantely, yes. (16/x)
Its difficult to find clean data on this question for a variety of reasons (that people much smarter than me can explain), but to me this is pretty telling. Among women with a preg-associated death, a much higher % of black women had preg-related deaths (17/x)

What about the causes of death? Is CV disease the leading cause of death? Again look at the table from the MMWR. The way to get to that conclusion is to combine CVA, Cardiomyopathy, and "other CV conditions". (18/x)

Other CV conditions btw includes a variety of conditions (congenital, ischemic, valvular disease, hypertensive heart disease (that is not a CVA I guess) & congestive heart failure (not related to cardiomyopathy?) (19/x)

While this makes sense from an epi grouping perspective, when enacting policy, these grouping are potentially dangerous because the approach to each of these rare conditions in pregnancy is different - so grouping results in overemphasis and exuberant policy interventions (20/x)
Here is an example. This well meaning administrator instituted automatic treatment for HTN above a threshold and automatic chest xrays for pregnant women with SOB to reduce the death rate to "1/2 the national average". jamanetwork.com/journals/jama/… (21/x)
Sounds great right? Except the national average is 17.2/100K. to reduce to half is 8.6. Since these guys had 210K births, if they started average their interventions reduced maternal death by 18. how many healthy preg women with SOB got unnecc chest xrays to achieve that? (22/x)
As @venkmurthy has explained in his thread on LQTS and the iwatch, there is great risk to widespread screening of a low prevalence condition, especially when the test characteristics (chest xray for volume overload) are mediocre at best (23/x)
So what to do? Well, I think the MMRIA and MMWR mentioned above give us hints. I like this table in particular (from MMRIA). It tells us maternal mortality is actually three distinct conditions, with the need to create three types of intervention sets. (24/x)

Will continue my thoughts for intervention on another thread when I get a moment. thanks for reading so far (25/25)
Would love to hear thoughts of other folks who do cardiac ob? @MinnowWalsh @purviparwani @ddefariayeh @DrMarthaGulati







