,
21 tweets,
11 min read
Read on Twitter
1/20
Inspired by some amazing @JohnsHopkinsDOM & @OslerResidency colleagues (@Dr_DanMD, @david_furfaro, @DxRxEdu to name a few), as well as the master @tony_breu, I’ve decided to take a stab at my first #pulmonology pathophysiology #tweetorial…
Inspired by some amazing @JohnsHopkinsDOM & @OslerResidency colleagues (@Dr_DanMD, @david_furfaro, @DxRxEdu to name a few), as well as the master @tony_breu, I’ve decided to take a stab at my first #pulmonology pathophysiology #tweetorial…
2/
Ever wonder why patients with cystic fibrosis (CF) tend to have more severe disease in the upper lung fields, especially on the right?
I have!
And the answer was not what I was expecting…
Ever wonder why patients with cystic fibrosis (CF) tend to have more severe disease in the upper lung fields, especially on the right?
I have!
And the answer was not what I was expecting…
3/
First, it is important to remember that CF is caused by mutations in the CFTR gene, which ultimately leads to thick, viscous secretions due to the inability to secrete chloride.
First, it is important to remember that CF is caused by mutations in the CFTR gene, which ultimately leads to thick, viscous secretions due to the inability to secrete chloride.

4/
Here is a series of short clips that beautifully depict the role of CFTR in the lungs: (credit to @NatWestMD for sharing this with me)
Here is a series of short clips that beautifully depict the role of CFTR in the lungs: (credit to @NatWestMD for sharing this with me)
5/
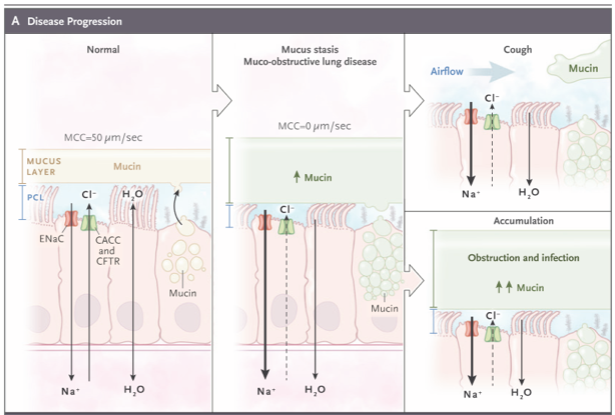
When this thick mucus accumulates, it becomes a nidus for airflow obstruction, infection, and inflammation. The @NEJM review article on Muco-Obstructive Lung Diseases from May 2019 does an amazing job explaining the pathophysiology behind this.
ncbi.nlm.nih.gov/pubmed/31091375
When this thick mucus accumulates, it becomes a nidus for airflow obstruction, infection, and inflammation. The @NEJM review article on Muco-Obstructive Lung Diseases from May 2019 does an amazing job explaining the pathophysiology behind this.
ncbi.nlm.nih.gov/pubmed/31091375
6/
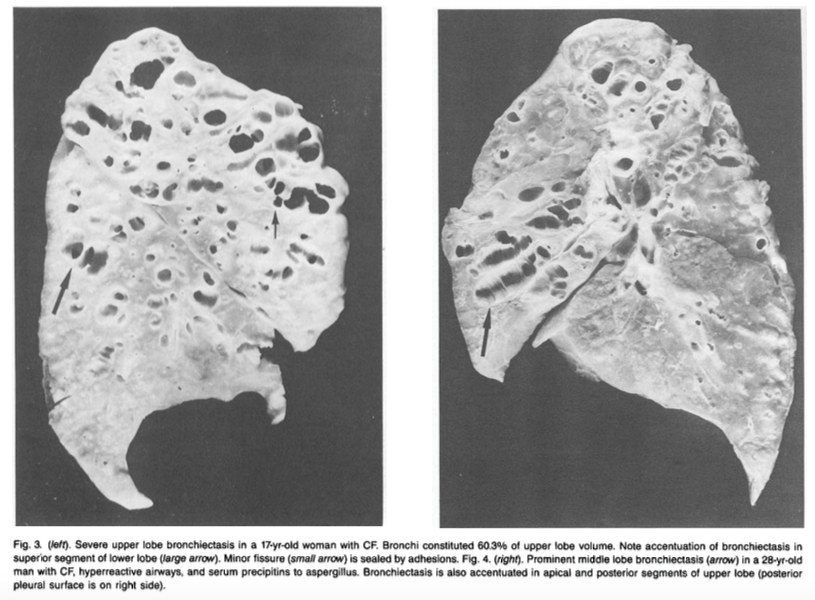
For decades it has been observed that CF tends to cause more severe disease in the upper lobes, particularly on the right. Regional variation in inflammation (upper>lower lobes) on BAL has also been demonstrated.
ncbi.nlm.nih.gov/pubmed/3963622
ncbi.nlm.nih.gov/pubmed/9372672
For decades it has been observed that CF tends to cause more severe disease in the upper lobes, particularly on the right. Regional variation in inflammation (upper>lower lobes) on BAL has also been demonstrated.
ncbi.nlm.nih.gov/pubmed/3963622
ncbi.nlm.nih.gov/pubmed/9372672



8/
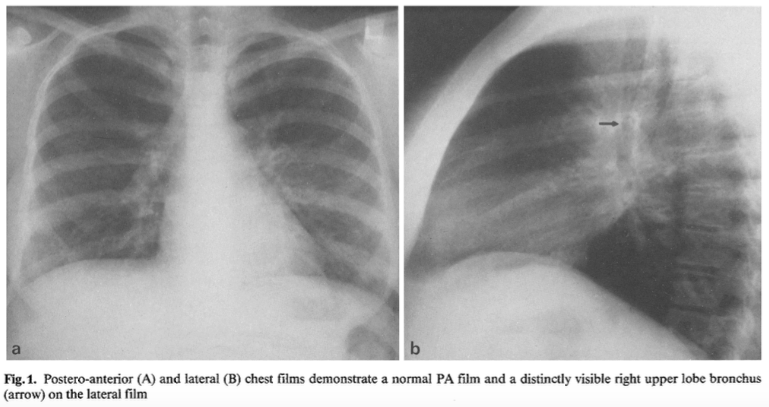
Interestingly, it was shown in 1985 (before newborn screening for CF was widespread) that a distinctly outlined orifice/thickening of the right upper lobe bronchus on lateral chest film in adolescents is a sensitive marker for CF.
ncbi.nlm.nih.gov/pubmed/3963622
Interestingly, it was shown in 1985 (before newborn screening for CF was widespread) that a distinctly outlined orifice/thickening of the right upper lobe bronchus on lateral chest film in adolescents is a sensitive marker for CF.
ncbi.nlm.nih.gov/pubmed/3963622
9/
So back to our original question. Why might the upper lobes be affected more than the lower lobes in patients with CF, especially on the right?
So back to our original question. Why might the upper lobes be affected more than the lower lobes in patients with CF, especially on the right?
10/
One commonly proposed mechanism includes reduced ventilatory excursion of the upper lobes when compared with the lower lobes (which have a closer proximity to the diaphragm), leading to inefficient clearance of secretions from upper lung regions via cough.
One commonly proposed mechanism includes reduced ventilatory excursion of the upper lobes when compared with the lower lobes (which have a closer proximity to the diaphragm), leading to inefficient clearance of secretions from upper lung regions via cough.
11/
While this explanation is attractive (and may very well contribute to worse disease in the upper lobes), it wouldn’t explain the right-sided predominance described above.
While this explanation is attractive (and may very well contribute to worse disease in the upper lobes), it wouldn’t explain the right-sided predominance described above.
12/
Another possible mechanism is that the higher partial pressure of oxygen in the upper lobes provides a selective advantage for aerobic bacterial growth such as pseudomonas (the major implicated respiratory pathogen as CF patients age).
Another possible mechanism is that the higher partial pressure of oxygen in the upper lobes provides a selective advantage for aerobic bacterial growth such as pseudomonas (the major implicated respiratory pathogen as CF patients age).
13/
Not only would this not explain the right-sided predominance, but studies have shown that airway inflammation is present in infants with CF who are as young as 4 weeks! (before colonization with CF-related pathogens)
ncbi.nlm.nih.gov/pubmed/7697234
Not only would this not explain the right-sided predominance, but studies have shown that airway inflammation is present in infants with CF who are as young as 4 weeks! (before colonization with CF-related pathogens)
ncbi.nlm.nih.gov/pubmed/7697234
14/
…not to mention that pseudomonas in patients without CF usually involves the lower lobes. Which brings us to the third answer…
ncbi.nlm.nih.gov/pubmed/4306124
…not to mention that pseudomonas in patients without CF usually involves the lower lobes. Which brings us to the third answer…
ncbi.nlm.nih.gov/pubmed/4306124
15/
The prevalence of gastroesophageal (GE) reflux is higher in CF patients than the general population (as high as ~80%!), and reflux has been associated with more severe lung disease.
ncbi.nlm.nih.gov/pubmed/24964289
The prevalence of gastroesophageal (GE) reflux is higher in CF patients than the general population (as high as ~80%!), and reflux has been associated with more severe lung disease.
ncbi.nlm.nih.gov/pubmed/24964289
16/
The mechansim for reflux in CF is thought to be due to ⬇️ lower esophageal spincter (LES) pressure & ⬆️ transient LES relaxations, which can lead to intermittent aspiration of acidic stomach contents, especially when supine.
ncbi.nlm.nih.gov/pubmed/22777342
The mechansim for reflux in CF is thought to be due to ⬇️ lower esophageal spincter (LES) pressure & ⬆️ transient LES relaxations, which can lead to intermittent aspiration of acidic stomach contents, especially when supine.
ncbi.nlm.nih.gov/pubmed/22777342
17/
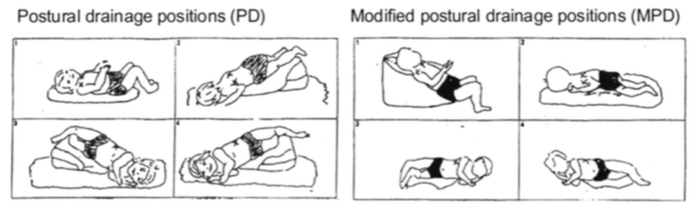
A 2003 study showed that when a modified postural draining position was adopted (versus the standard Trendelenberg position) in CF patients, reflux decreased, as did respiratory complications, further supporting the ⬇️ LES pressure theory.
ncbi.nlm.nih.gov/pubmed/12567389
A 2003 study showed that when a modified postural draining position was adopted (versus the standard Trendelenberg position) in CF patients, reflux decreased, as did respiratory complications, further supporting the ⬇️ LES pressure theory.
ncbi.nlm.nih.gov/pubmed/12567389
18/
Supine aspiration of acidic stomach contents compounds the vicious cycle of inflammation, infection, and progression of lung disease, particularly in the right upper lobe due to anatomical positioning.
Supine aspiration of acidic stomach contents compounds the vicious cycle of inflammation, infection, and progression of lung disease, particularly in the right upper lobe due to anatomical positioning.


19/
Before summarizing, lets revisit the original question once more:
Why does CF tend to cause more severe disese in the upper lobes, especially on the right?
Before summarizing, lets revisit the original question once more:
Why does CF tend to cause more severe disese in the upper lobes, especially on the right?
20/
SUMMARY
✅ CF patients have ⬇️ LES pressure, leading to ⬆️ GE reflux
✅ Reflux leads to aspiration of acidic stomach contents, which triggers a cascade of inflammation & worsening lung disease
✅ Supine aspiration affects upper > lower lobes, R > L
SUMMARY
✅ CF patients have ⬇️ LES pressure, leading to ⬆️ GE reflux
✅ Reflux leads to aspiration of acidic stomach contents, which triggers a cascade of inflammation & worsening lung disease
✅ Supine aspiration affects upper > lower lobes, R > L
21/
Obviously, this is just a theory, but interested to hear others thoughts! @NatWestMD @CMerloMD @sanjayvdesai @hopkinscf @ChadHoc @david_furfaro @DxRxEdu @CPSolvers
Obviously, this is just a theory, but interested to hear others thoughts! @NatWestMD @CMerloMD @sanjayvdesai @hopkinscf @ChadHoc @david_furfaro @DxRxEdu @CPSolvers