PROBLEM
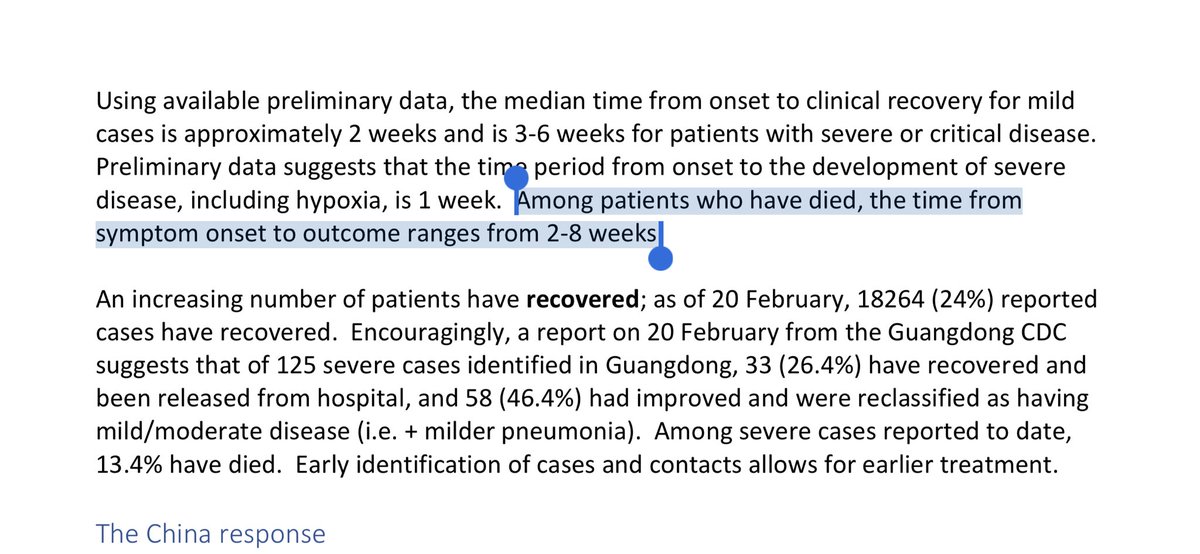
For 80% the disease is mild, but for 20% it's severe.
SOLUTION
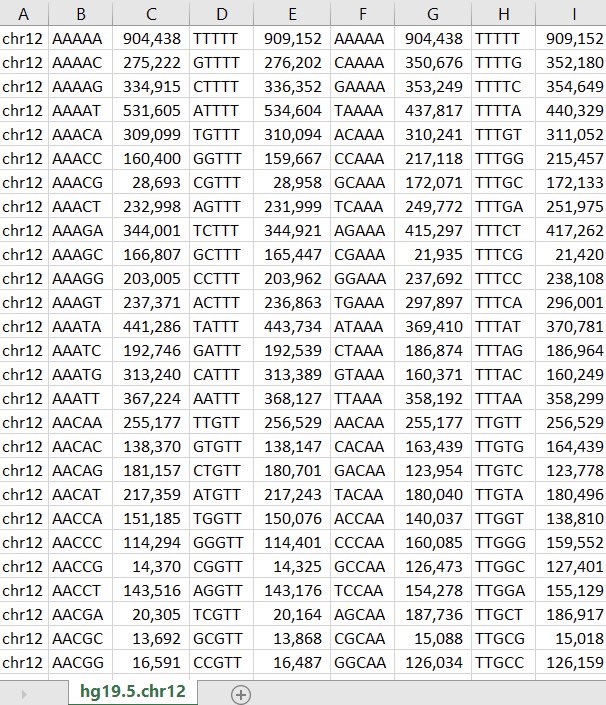
Sequence all infected. Record clinical outcome: mild or severe? Do association study to predict outcome from genomics, phenotype.
You *might* be able to predict probability of coming down with a severe case.
For 80% the disease is mild, but for 20% it's severe.
SOLUTION
Sequence all infected. Record clinical outcome: mild or severe? Do association study to predict outcome from genomics, phenotype.
You *might* be able to predict probability of coming down with a severe case.

This is a high-stakes GWAS. You'd need large samples & strong signal to be confident in it.
But if it did work, you might be able to let the subgroup with the lowest predicted risk out of quarantine after genotyping them.
This can unblock the production of vaccines, antivirals.
But if it did work, you might be able to let the subgroup with the lowest predicted risk out of quarantine after genotyping them.
This can unblock the production of vaccines, antivirals.
As more context, the thing I've been most concerned about is the virus infecting frontline healthcare workers (MDs, nurses) and the people working on diagnostics, vaccines, therapeutics who have to handle dangerous samples.
Knowing who's at higher risk may help a lot here.
Knowing who's at higher risk may help a lot here.
REFERENCES
There's a literature on genetic determinants of infectious disease susceptibility. Some cites:
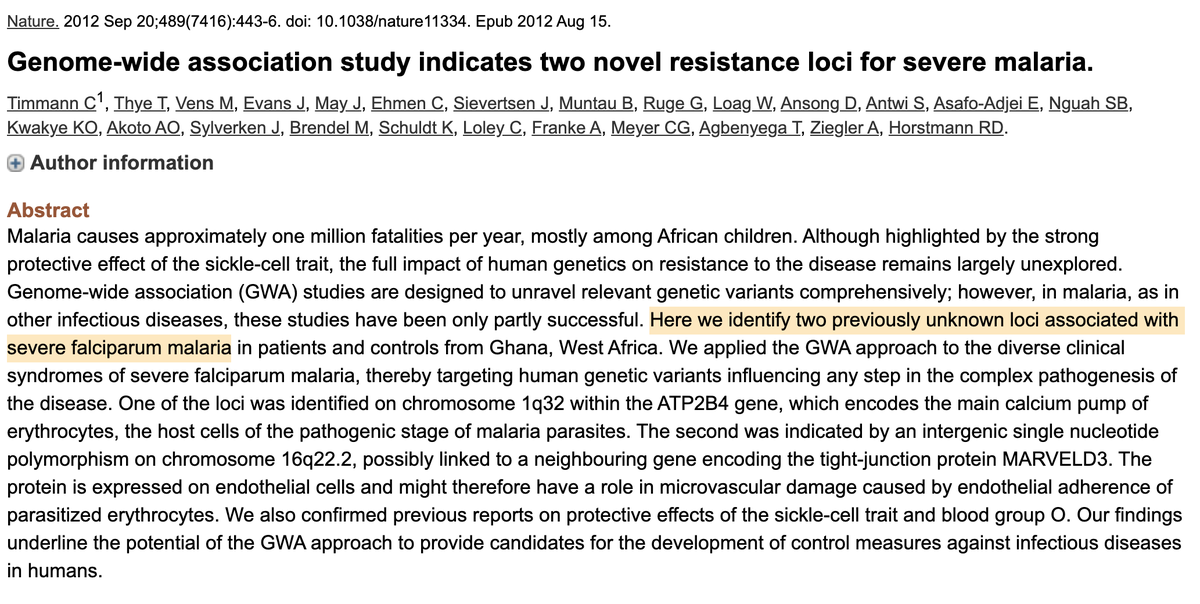
1) Malaria: ncbi.nlm.nih.gov/pubmed/2289518……
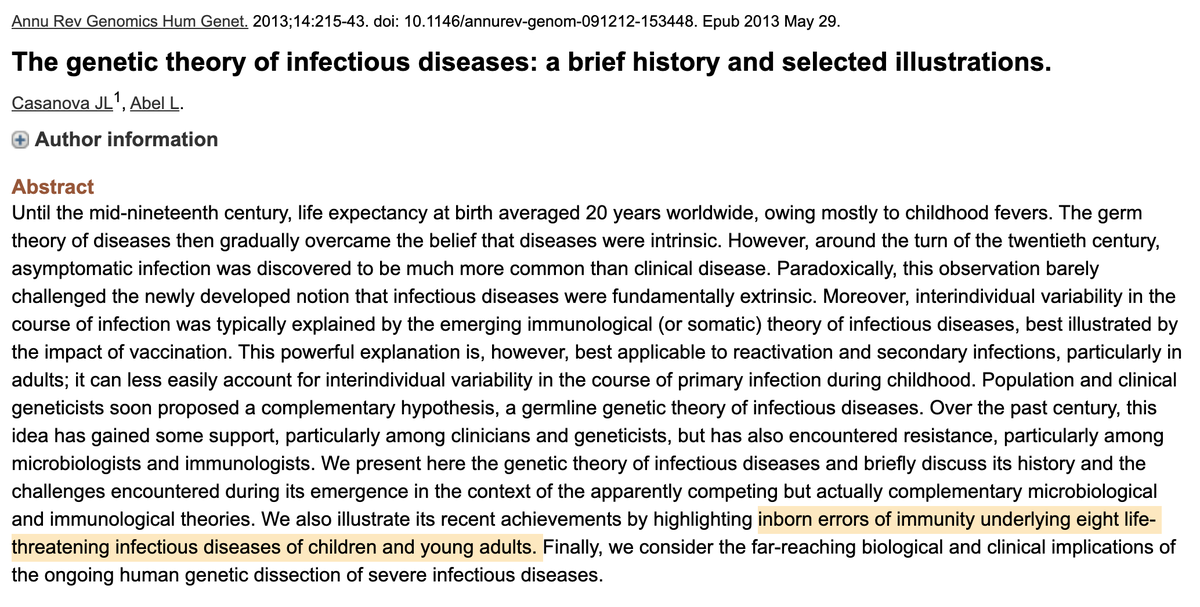
2) Theory:
ncbi.nlm.nih.gov/pubmed/2372490……
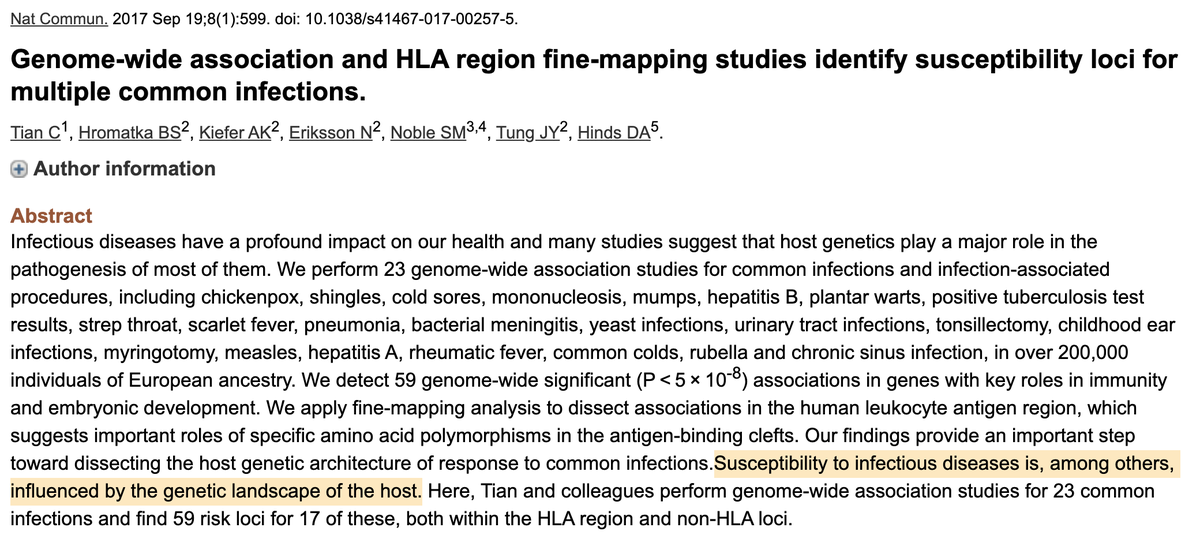
3) 20+ diseases: ncbi.nlm.nih.gov/pubmed/2892844……
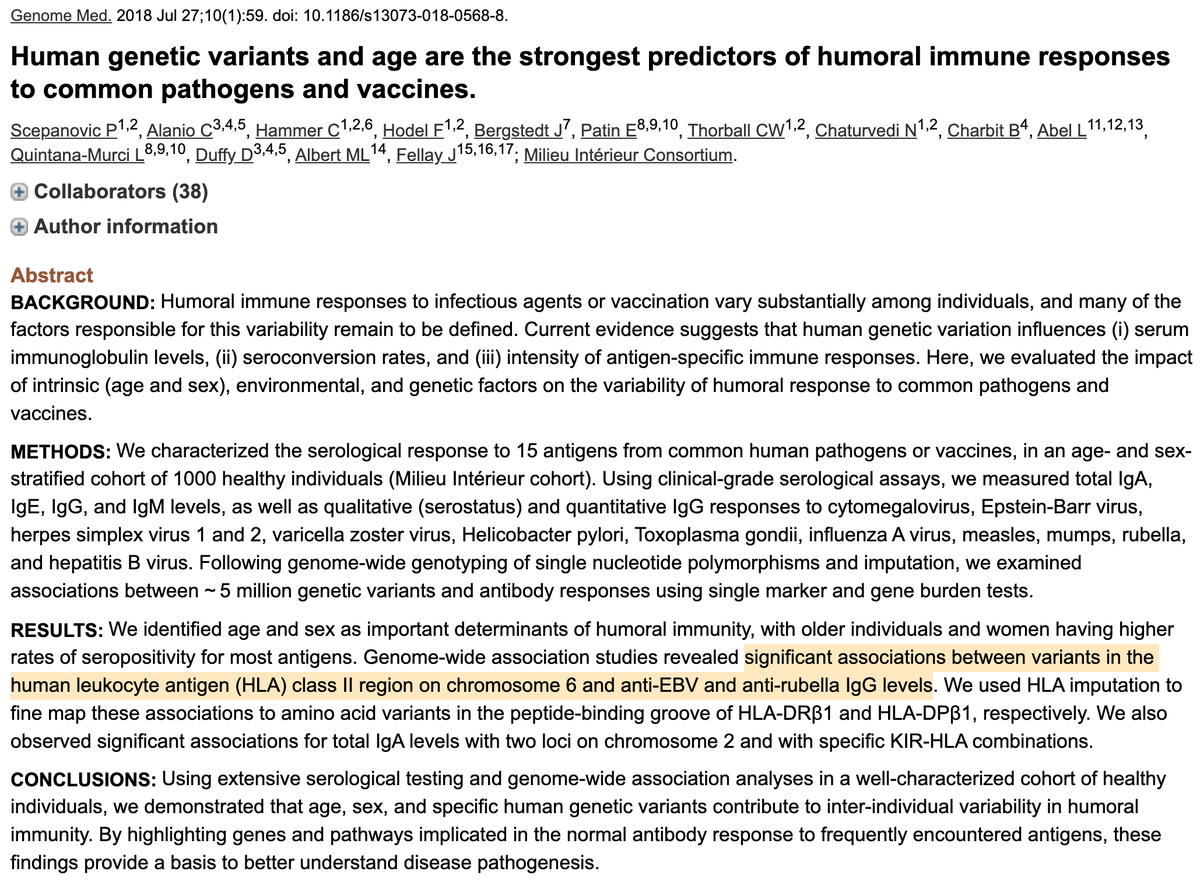
4) 10+ diseases:
ncbi.nlm.nih.gov/pubmed/30053915
There's a literature on genetic determinants of infectious disease susceptibility. Some cites:
1) Malaria: ncbi.nlm.nih.gov/pubmed/2289518……
2) Theory:
ncbi.nlm.nih.gov/pubmed/2372490……
3) 20+ diseases: ncbi.nlm.nih.gov/pubmed/2892844……
4) 10+ diseases:
ncbi.nlm.nih.gov/pubmed/30053915
One point worth repeating: trait prediction from genetics isn't a layup.
Sometimes you get great signal from just a single variant, or a small number (eg OCA2/eyes). Other times you need many (eg PGS).
So this would have to give strong signal. But the ROI is high if it works.
Sometimes you get great signal from just a single variant, or a small number (eg OCA2/eyes). Other times you need many (eg PGS).
So this would have to give strong signal. But the ROI is high if it works.
1) Most fundamental idea: can we predict severity? That's highly actionable.
2) Specific inputs are flexible. As noted in OP, can be phenotype + genetics.
3) Age/gender: cheap to ascertain, high value. Assess other predictors via ascertainment cost vs predictive benefit.
2) Specific inputs are flexible. As noted in OP, can be phenotype + genetics.
3) Age/gender: cheap to ascertain, high value. Assess other predictors via ascertainment cost vs predictive benefit.