This is a bizarre answer and I'm curious what epi folks make of this.
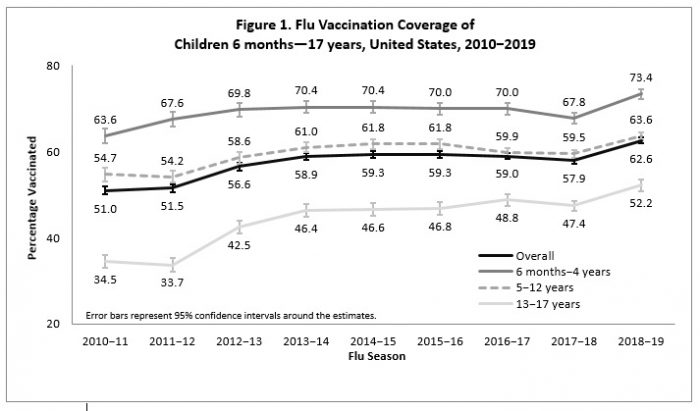
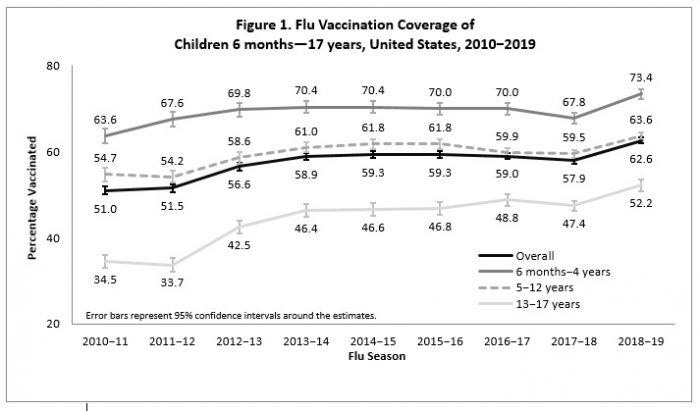
There is NO data I have seen to suggest a CFR approaching anywhere close to the 0.1% CFR for seasonal flu.
What we've seen so far is that COVID-19 fatality rate is highly variable but much higher than flu.
There is NO data I have seen to suggest a CFR approaching anywhere close to the 0.1% CFR for seasonal flu.
What we've seen so far is that COVID-19 fatality rate is highly variable but much higher than flu.
Lowest-end estimates I've seen are 0.6% in South Korea and 0.7% non-Hubei areas of China. These are prob the best proxies we have because testing has been widespread in both places, so they're the most complete picture we've got of the CFR denominator. scmp.com/week-asia/heal…
So if those are our best provisional estimates of low-end mortality - that's still 6-7x as deadly as seasonal flu. That's extremely dangerous!
But there's more. Really important to remember, as @maiamajumder notes, that CFR is not a fixed characteristic.
But there's more. Really important to remember, as @maiamajumder notes, that CFR is not a fixed characteristic.
And WHO's China mission report makes this extremely clear: CFR varied hugely between Wuhan and everywhere else.
CFR in Wuhan was 5.8% - a frankly scary figure. About 8x higher than the low-end estimates and 58x (!!) higher than seasonal flu.
CFR in Wuhan was 5.8% - a frankly scary figure. About 8x higher than the low-end estimates and 58x (!!) higher than seasonal flu.

Also really important - CFR varied highly over time. In Wuhan in the earliest phase, it was much higher still - over 20% (likely reflecting the early bias toward finding the most severe cases). As testing widened and China's lockdown slowed transmission, CFR improved.

There are a lot of factors that go into explaining these variances, and we don't understand them fully yet. But one of them is definitely the availability of quality medical care vs the volume of severe and critical cases.
So an important priority must be managing that ratio.
So an important priority must be managing that ratio.
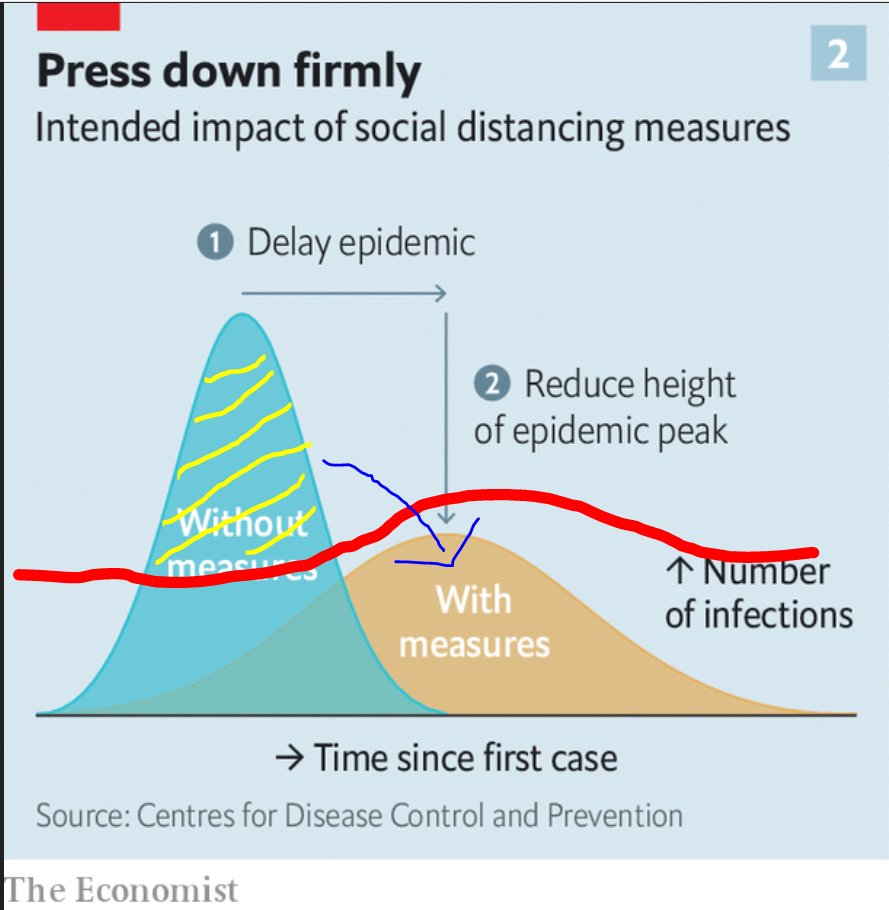
This chart shows conceptually how social distancing can delay and depress the arrival of an epidemic peak. Smart public health measure can depress the curve further.
So if intensive treatment capacity is a horizontal line, you want to keep peak case volume at or below that line.
So if intensive treatment capacity is a horizontal line, you want to keep peak case volume at or below that line.

Measures to depress the curve help limit the strain on hospital capacity, thus improving care quality and reducing CFR.
And by delaying the peak, public health measures can also buy time to surge treatment capacity so that care quality can keep up with the epidemic peak.
And by delaying the peak, public health measures can also buy time to surge treatment capacity so that care quality can keep up with the epidemic peak.

So Wuhan's declining CFR likely due partly to early explosive case volume exceeding clinical capacity (yellow stripes). Suppressing the curve (lockdown, contact tracing, etc) and surging treatment (1000-bed clinic), brought clinical capacity into line with case volume (arrow).
Now, the above charts are a little misleading, because they show both scenarios with the same starting point. That won't happen, because you won't have the perfect foresight to trigger social distancing, etc, immediately. Takes time to detect cases, assess risk, plan, execute.
So in reality you trigger social distancing and public health measure once you're already partway up that original epidemic curve. And the further you are up that curve, the more aggressive and extensive the measure must be to bend it. Here's Wuhan's actual curve.

So you can see how it quickly flattens when lockdown & other measures imposed - stabilizing then reducing the curve. And with a (totally notional) line representing hospital capacity, you can see how opening the 1000-bed clinic could bring capacity into line with case volume.

So as the US now faces our own outbreak(s), the important questions are 1) how far have our major cities progressed up their curves; 2) what is our ratio of clinical surge capacity to potential case volume, and 3) what can we do to bring these into manageable alignment?
And that's a really long explanation for why I take issue with the official's statement on likely CFR. Because unless we have clearer answers to those three questions, we have no idea whether mortality in US cities will be closer to S. Korea (hopefully) or Wuhan.
And that's again why testing delays are so so damaging - makes it hard to tell where we are along the epi curve, and therefore what risk is posed to our health systems, and how aggressively we must calibrate mitigation measures.
That's it. WASH YOUR HANDS!
That's it. WASH YOUR HANDS!
(This threaded weird for some reasons - click on the last tweet above and the rest of the thread should show up)
(Also - would gratefully invite professional epi folks to correct if I've mischaracterized anything here)
See also - these curves from the 1918 pandemic
Pinning this to the end of the thread. I think @aetiology is right about the sourcing on this, and we discuss why I think that's still very problematic as risk messaging.
Fauci NEJM piece makes pretty clear that a <1% CFR is a speculative assumption, not something grounded in current data. "If one assumes"..."CFR *may* be..."
That's quite different from Giroir characterization: "The best estimates of the overall mortality rate."
That's quite different from Giroir characterization: "The best estimates of the overall mortality rate."

Addendum - related thread on how these dynamics look in the developing world:
Addendum-dendum - had meant to also point out, as @PeterHotez does here, that CFR can also vary greatly by age. COVID-19 CFR dramatically higher among the elderly.