1. Let's begin! Just to recap: a 25 y/o female cyclist with no known past medical history presents to the emergency department after sustaining a collision with a bus. Upon arrival to the emergency department she is un-arousable with a GCS of 7. #BBTBI
2. What is your immediate next step in her management? Is there any speciality you’d like to involve early? #BBTBI
3. The priorities of assessment and resuscitation should follow Airway, Breathing and Circulation. Attention to these aspects will reduce further brain injury. It’s important to involve neurosurgery and anaesthetics early for intubation and mechanical ventilation. #BBTBI
4. The role of intubation and mechanical ventilation in patients with head trauma is to maintain adequate oxygenation and respiration, as well as prevention of aspiration. For this reason, endotracheal intubation is often performed. #BBTBI
5. The anaesthetist arrives and intubates the patient. During the intubation the anaesthetist also administers a muscle relaxant, short acting sedation, analgesia and begins mechanical ventilation. #BBTBI
6. In head injury it’s vital that the patient is adequately oxygenated and ventilated to avoid any further brain injury. If there is inadequate oxygenation this can be detrimental to brain tissue. #BBTBI
7. The brain has a high oxygen consumption and without oxygen, energy dependent processes in the brain cease leading to irreversible cellular injury. #BBTBI
8. Ventilation is another important aspect to consider in a brain injury patient. Reduced ventilation can result in the build-up of carbon dioxide (hypercapnia). Cerebral blood flow is actually largely dependent on carbon dioxide. 🩸🌬️ #BBTBI
9. Do you know what carbon dioxide does to the cerebral blood vessels? #BBTBI
10. So, what carbon dioxide does is that it causes vasodilation of the cerebral vessels. Vasodilation of the blood vessels means that the cerebral blood flow increases. This causes the cerebral blood volume to increase and consequently the intra-cranial pressure. #BBTBI
11. Therefore, carbon dioxide must be closely monitored and maintained in the normal range of 4-4.5 kpa. If there is difficulty maintaining this range, the patient is mechanically ventilated. #BBTBI
12. You now move onto C (circulation). You notice the patients BP is 86/54. As we’ve just learned, MAP must be higher than ICP in order to perfuse the brain. Does anyone have any idea how we should increase BP? 👆 #BBTBI
13. This is achieved by aggressive fluid resuscitation. Hypotension should be treated aggressively as it is the biggest cause of secondary ischaemic injury. In some cases, pressor support and inotropes may also be required if low pressure persists after fluid resuscitation.#BBTBI
14. The patient is now administered I.V fluids. Now that ABC has been assessed and she is stabilised it is important to evaluate the extent of neurological impairment. #BBTBI
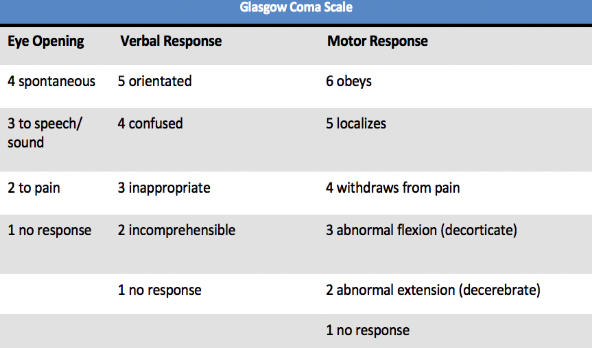
15. You go onto access the patients GCS again. She doesn’t open her eyes; she withdraws her arms to pain and she mutters incomprehensible sounds in response to your questions. Based on your assessment what is her GCS? #BBTBI
16. The patient has a GCS of 7. She doesn’t open his eyes = 1, mutters incomprehensible sounds = 2 and she withdraws from pain = 4. This can be written as E1V2M4. #BBTBI 
17. On further examination you notice her right pupil to be 7mm and non-reacting and her left pupil to be 3mm and reacting. What do you think is the cause? 🔦👀 #BBTBI

18. This is a fixed dilated pupil. Most likely due to Uncal (trans-tentorial) herniation! 👁️ #BBTBI
19. Does anyone know what uncal herniation is and what is the cause? 🧠#BBTBI
20. Uncal herniation occurs when rising ICP causes herniation of the medial temporal lobe from the middle into the posterior fossa, across the tentorial opening. The uncus herniates over the tentorial notch compressing the CN III located just medial to the uncus. #BBTBI
21. Who knows why pupillary dilatation is often the first sign in uncal herniation? #BBTBI
22. As the parasympathetic fibres are on the outside of the third nerve, the first sign of uncal herniation is usually pupillary dilation. #BBTBI
23. Does anyone know of any other herniation syndromes? ( 🔎hint, we mentioned one yesterday!) #BBTBI

25. Are there any imaging tests you’d like to do at this point? #BBTBI
26. Head CT scan! The current primary investigation of choice for the detection of acute clinically important brain injuries is CT imaging of the head. 🧠💀#BBTBI

28. The head CT reveals an acute right subdural hematoma with mass effect and midline shift. #BBTBI
29. Can anyone tell us what blood vessel is involved in subdural hematoma? #BBTBI
30. Bridging veins! 🌉 #BBTBI
31. So.. who wants to operate? #BBTBI
32. The decision is made to perform a right decompressive craniectomy to permit brain swelling and reduce the ICP. The patient is taken to theatre and the clot evacuated. #BBTBI
33. Check out our video later to see how remove the clot and what surgery is involved! youtube.com/watch?v=iGpLBP… #BBTBI
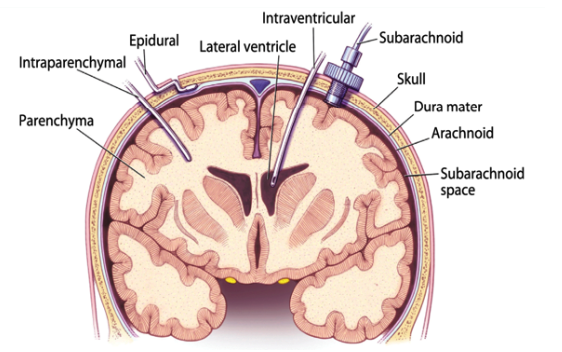
34. During the procedure an ICP bolt is placed. This allows for the monitoring of ICP and is the gold standard. ICP bolts can be placed in either the subdural or epidural space. 🔩💀 #BBTBI
35. There are other methods to monitor ICP in different intracranial locations. These include an extraventricular drain (EVD) or intraparenchymal catheter. These are illustrated below ! #BBTBI
36. Does anyone know of any pharmacological methods we can use to control ICP? 💊 #BBTBI
37. Mannitol! Mannitol is widely used in head injury management. It is an osmotic diuretic which sets up an osmotic gradient and draws water out of neurons, reducing ICP. Mannitol is best given in boluses. Does anyone know why? #BBTBI
38. After prolonged administration (continuous infusion) mannitol molecules move across into the cerebral interstitial space and may exacerbate cerebral oedema and raise ICP😲#BBTBI
39. The patient is taken to ITU and has maximal medical management. This consists of: 1⃣ The patients head remains in a neutral position with the head of the bed elevated to 30 degrees. The reason for this is to promote jugular venous outflow and reduce ICP. #BBTBI
40. 2⃣ The patient is sedated and prescribed analgesia. The purpose of this is to decrease the cerebral metabolic rate of oxygen consumption, and thus reduce ICP. #BBTBI
41. 3⃣ It’s also important to maintain cerebral oxygenation. Oxygen saturation must be maintained higher than 90% and carbon dioxide controlled between 25-30mmHg to avoid hypercapnia. 🌬️ #BBTBI
42. 4⃣ Systolic blood pressure must be above 90mmHg to maintain an adequate cerebral perfusion pressure and thus cerebral blood flow. #BBTBI
43. 5⃣ During periods of elevated ICP, mannitol may be used in boluses to decrease cerebral oedema. ⏬🧠 #BBTBI
44. Finally: Following 15 days in ITU the patient is extubated. She has a further CT scan of the head in order to plan a cranioplasty. She is stepped down to the neurorehabilitation ward for ongoing physiotherapy and rehabilitation #BBTBI
45. And that's all for this round folks! We hope you enjoyed this CBD on TBI Clinical Management. We'd love your feedback to see how we can improve in the future (certificates for completion!) Tune in again next time! #BBTBI #neurosurgery