
(1/) I want to bounce around a disease model for #COVID19. This is hypothesis, some parts are hand-wavy, but I'd like to think a lot is also based on evidence. I'll try to clearly distinguish knowns from assumptions as we go...
#COVID2019 #SARSCoV2 #medtwitter #FOAMcc #FOAMed
#COVID2019 #SARSCoV2 #medtwitter #FOAMcc #FOAMed
Would love to hear some #ICU/#CriticalCare/#PCCM tweeps thoughts on this idea.
cc @gattinon @DrMCecconi @ogi_gajic @msiuba @matthieulegrand @JamiePrivratsky @HalliePrescott @TimBuchmanMDPhD @DrSamuelBrown @KhannaAshishCCM @PulmCrit @critconcepts @nelsonSpinto
cc @gattinon @DrMCecconi @ogi_gajic @msiuba @matthieulegrand @JamiePrivratsky @HalliePrescott @TimBuchmanMDPhD @DrSamuelBrown @KhannaAshishCCM @PulmCrit @critconcepts @nelsonSpinto
(2/)First, whatever #COVID19 is, it doesn't sound like #ARDS. Physiology doesn't line up
1-Easy to vent, but hard to oxygenate. Normal lung compliance
2-Deteriorate rapidly
3-Responds to proning, PEEP, & prolonging I:E
4-Tendency to suddenly de-recruit
atsjournals.org/doi/abs/10.116…
1-Easy to vent, but hard to oxygenate. Normal lung compliance
2-Deteriorate rapidly
3-Responds to proning, PEEP, & prolonging I:E
4-Tendency to suddenly de-recruit
atsjournals.org/doi/abs/10.116…
(3/) The imaging doesn't fit either:
5- CTs (at least initially) w/ interstitial and pleural predominance of consolidation.
pubs.rsna.org/doi/10.1148/ra…
(*should clarify we're talking early in disease course, not after 2 weeks on the vent*)
5- CTs (at least initially) w/ interstitial and pleural predominance of consolidation.
pubs.rsna.org/doi/10.1148/ra…
(*should clarify we're talking early in disease course, not after 2 weeks on the vent*)
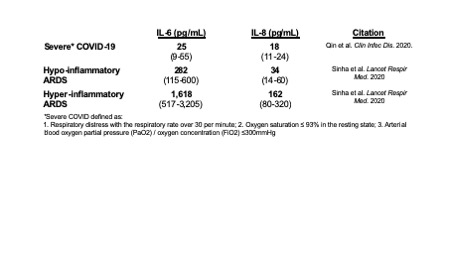
(4/) Nor does the chemistry. Inflammatory markers are decidedly unimpressive. Severe COVID in Wuhan, mean IL-6 reported 10X less than *hypo*inflammatory ARDS
60X < hyperinflammatory ARDS
academic.oup.com/cid/advance-ar…
Remind me why we think anti-inflammatory Rx is a good idea again?
60X < hyperinflammatory ARDS
academic.oup.com/cid/advance-ar…
Remind me why we think anti-inflammatory Rx is a good idea again?
(5/) To summarize so far, #COVID19
-isn't hyper-inflammatory,
-Resp. physiology doesn't fit ARDS at all,
-Imaging doesn't fit ARDS.
...So what is it?
-isn't hyper-inflammatory,
-Resp. physiology doesn't fit ARDS at all,
-Imaging doesn't fit ARDS.
...So what is it?
(6/)I'm first gonna suggest the driving resp insult is thrombotic. Compliant lungs w/ persistent hypoxia sounds like what I've always been taught bad PE looks like.
We've all seen the dimer data. I'm hearing the pts are sticky, constantly clogging dialysis filters, etc..
We've all seen the dimer data. I'm hearing the pts are sticky, constantly clogging dialysis filters, etc..
(7/)I'd been thinking of this more as thrombotic microangiopathy, but going back to the SARS epidemic, PE was common, and there no reason why #COVID19 couldn't include a lot of frank acute PE.
ncbi.nlm.nih.gov/pubmed/14736283
I'm sure others have already suggested these ideas too.
ncbi.nlm.nih.gov/pubmed/14736283
I'm sure others have already suggested these ideas too.
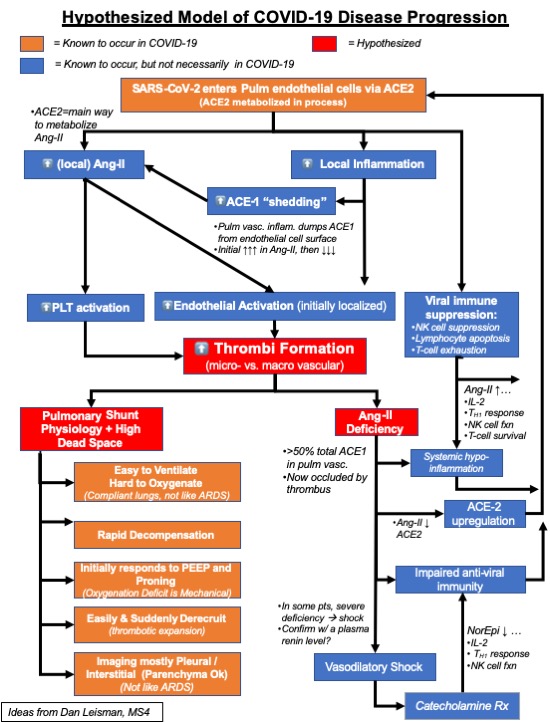
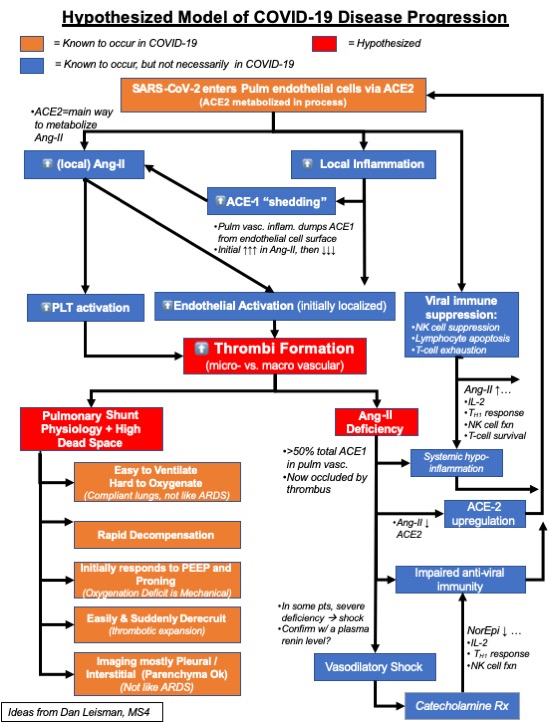
(8/) So molecularly, what might be happening? Back to facts.
#SARSCoV2 enters cells using ACE-2 on pulm endothelium. (Common knowledge at this point).
ncbi.nlm.nih.gov/pubmed/32100877
#SARSCoV2 enters cells using ACE-2 on pulm endothelium. (Common knowledge at this point).
ncbi.nlm.nih.gov/pubmed/32100877
(9/) Viral infxn probably enough to start localized inflammation alone, which is well documented to activate endothelium & clotting.
But viral entry also consumes ACE2. ACE2 = primary means of Angiotensin-II degradation --> increased Ang2.
ncbi.nlm.nih.gov/pubmed/23720263
But viral entry also consumes ACE2. ACE2 = primary means of Angiotensin-II degradation --> increased Ang2.
ncbi.nlm.nih.gov/pubmed/23720263
(10/) So now a Q.
ACE2 metabolizes Ang-II.
ACE1 forms Ang-II by metabolizing Ang-I.
Where is most pulmonary ACE1 found?
ACE2 metabolizes Ang-II.
ACE1 forms Ang-II by metabolizing Ang-I.
Where is most pulmonary ACE1 found?
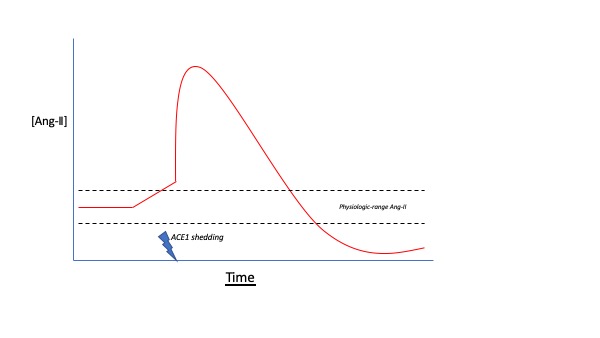
(11)B/c ACE1 is highly expressed on pulm endothelial surface, vasc inflammation can lead to a phenomenon known as ACE1 "shedding".
This means ACE1 is rapidly dumped into interstitium, leading initially to sharply ⬆️local Ang-II, then to ⬇️⬇️Ang-II
atsjournals.org/doi/abs/10.116…
This means ACE1 is rapidly dumped into interstitium, leading initially to sharply ⬆️local Ang-II, then to ⬇️⬇️Ang-II
atsjournals.org/doi/abs/10.116…
(12/) So initially, a confluence of viral infxn, localized endothelial activation, and ACE2 consumption *could* start an Ang-II driven feedforward loop leading to marked endothelial activation and coagulation.

(11/) Another Q:
Where is most of the total body ACE1 found?
Where is most of the total body ACE1 found?
(12/) The highest density of total body ACE-1 is found on pulmonary endothelium.
As ACE-1 gets widely shed and/or pulmonary vasculature clots off, Ang-II deficiency (rather than excess) likely develops.*
[**THIS STATEMENT = HYPOTHESIS ONLY**]
As ACE-1 gets widely shed and/or pulmonary vasculature clots off, Ang-II deficiency (rather than excess) likely develops.*
[**THIS STATEMENT = HYPOTHESIS ONLY**]
(13/) I'm hearing from ICU fellows that COVID + shock has been extremely responsive to Giapreza. Still, anecdote does not evidence make.
The biology is easy enough to interrogate though. Check a plasma renin level. Massive elevation suggests ACE1 (& thus AngII) deficit.
The biology is easy enough to interrogate though. Check a plasma renin level. Massive elevation suggests ACE1 (& thus AngII) deficit.
(14/)Anyway, there are a number of reasons why an ang-II deficiency might be a really bad thing in the setting of #SARSCoV2.
For one, Ang-II downregulates ACE2. ACE1 inhibition and ARBs upregulate ACE2.
ncbi.nlm.nih.gov/pmc/articles/P…
For one, Ang-II downregulates ACE2. ACE1 inhibition and ARBs upregulate ACE2.
ncbi.nlm.nih.gov/pmc/articles/P…
A lot's been made of this idea already. It sounds nice, although i'm not all that convinced it's a big story.
thelancet.com/journals/lanre…
thelancet.com/journals/lanre…
(15/) But what I think has been totally overlooked are Ang-II's profoundly immune-modulatory effects, especially re: viral immunity.
Ang-II:
-⬆️T-cell activation & ⬆️IL-2, initiating TH1 differentiation, which is important for antiviral response
jasn.asnjournals.org/content/28/5/1…
Ang-II:
-⬆️T-cell activation & ⬆️IL-2, initiating TH1 differentiation, which is important for antiviral response
jasn.asnjournals.org/content/28/5/1…
(16/) Ang-II also promotes Natural Killer (NK) cell proliferation and function.
jasn.asnjournals.org/content/18/4/1…
NK cells are critical in viral immunity, and NK depletion was correlated with disease severity in the SARS epidemic.
ncbi.nlm.nih.gov/pubmed/15080302
jasn.asnjournals.org/content/18/4/1…
NK cells are critical in viral immunity, and NK depletion was correlated with disease severity in the SARS epidemic.
ncbi.nlm.nih.gov/pubmed/15080302
(17/) And for the patients who do progress to shock, norepinephrine opposes virtually all of these putatively beneficial immune effects of ang-II.
atsjournals.org/doi/full/10.11…
atsjournals.org/doi/full/10.11…
(18/)So to summarize, I think:
-#COVID19 doesn't smell like ARDS: physiologically or immunologically.
-COVID physio looks more like thrombosis & viral-immunosuppression then hyper🔥& ARDS
-?Angiotensin system imbalances at immune/vascular interface could mediate a lot of this?
-#COVID19 doesn't smell like ARDS: physiologically or immunologically.
-COVID physio looks more like thrombosis & viral-immunosuppression then hyper🔥& ARDS
-?Angiotensin system imbalances at immune/vascular interface could mediate a lot of this?
(19/) One last thing @Leo_ReapDO pointed out that lymphocytes and gut Epithelia express ACE2. In fact, nearly all cells express ACE2.
So maybe this respiratory virus is a lot more systemic than we think. And maybe endothelial activation & thrombosis isn't just limited to lungs
So maybe this respiratory virus is a lot more systemic than we think. And maybe endothelial activation & thrombosis isn't just limited to lungs







