1/ All teachers will have learners who aren’t meeting expectations.
Providing feedback in these situations can be tough, but is VITALLY important.
Hang with us, the #MedEdTwagTeam, and we will walk you through it on today’s #TweetorialTuesday!
Providing feedback in these situations can be tough, but is VITALLY important.
Hang with us, the #MedEdTwagTeam, and we will walk you through it on today’s #TweetorialTuesday!

2/ Today, we will discuss the “struggling learner”, a terrible phrase that shouldn’t be used.
From now on, we will be discussing the learner who isn’t meeting expectations (LWIME). This doesn’t label, and describes their current behaviors, not their potential.
From now on, we will be discussing the learner who isn’t meeting expectations (LWIME). This doesn’t label, and describes their current behaviors, not their potential.

3/ Can we define LWIME? Per @JenniferSpicer4 & @gradydoctor, you need a measuring stick to say whether a learner is, or is not, meeting expectations.
Great tools are the #ACGME Core Competencies or #CanMEDS Framework. You can further break this down by specialty #milestones.
Great tools are the #ACGME Core Competencies or #CanMEDS Framework. You can further break this down by specialty #milestones.

4/ Why is this important?
In order to identify BEHAVIOR for improvement, it is very important to be specific. These institutional measuring sticks help you focus your assessment AND your coaching.
In order to identify BEHAVIOR for improvement, it is very important to be specific. These institutional measuring sticks help you focus your assessment AND your coaching.
5/ After you have defined the domain in which a learner isn’t meeting expectations, you need to clarify:
🔑 Cause (work vs. non-work issues)
🔑 Frequency (limited vs. recurrent/frequent)
This data will help you tailor your feedback.
🔑 Cause (work vs. non-work issues)
🔑 Frequency (limited vs. recurrent/frequent)
This data will help you tailor your feedback.

6/ This is why the “ART of Feedback” is so helpful. It allows you to gather collateral information and perspective (regarding cause and frequency, etc.) from your learners to help shape your feedback.
https://twitter.com/GStetsonMD/status/1366811589630857216

7/ So, the tools needed to discuss an area that needs improvement are:
⭐️Behavior
⭐️Cause
⭐️Frequency
What if you can’t pinpoint the answer to any of these?
Talk the case over with a trusted, confidential colleague. You will likely end up describing the behaviors.
⭐️Behavior
⭐️Cause
⭐️Frequency
What if you can’t pinpoint the answer to any of these?
Talk the case over with a trusted, confidential colleague. You will likely end up describing the behaviors.

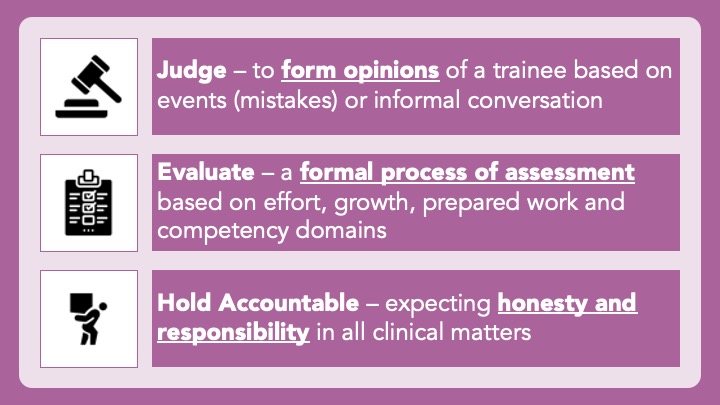
8/ If the area in which a learner isn’t meeting expectations is not listed in the competencies or milestones, then it is time to check yourself.
Are my expectations out of whack?
Is it just a personal attribute that annoys me?
Am I being biased (racist, sexist, ageist, etc.)?
Are my expectations out of whack?
Is it just a personal attribute that annoys me?
Am I being biased (racist, sexist, ageist, etc.)?
9/ Again, find a trusted colleague to discuss if you are having a hard time here.
10/ Even if the expectation is on the list, #bias can still play a role. #Professionalism is a particularly sticky one as the “rules” of professionalism have historically been defined by white-cis-hetero male physicians (speaking as one).
CC: @PedsOtoDoc
pubmed.ncbi.nlm.nih.gov/32134778/
CC: @PedsOtoDoc
pubmed.ncbi.nlm.nih.gov/32134778/

11/ Equipped with your three data points it is now time to deliver the feedback. When it is your turn to “tell”, make sure to do the following:
🔑Name the behavior
🔑Explain (using specific examples) the impact of the behavior
🔑Ask for the learner’s reflections
🔑Name the behavior
🔑Explain (using specific examples) the impact of the behavior
🔑Ask for the learner’s reflections

12/ Delivering feedback as close to the event (good or bad) is important, but for the LWIME, it is VITAL.
The sooner you 2 are on the same page about the work that needs to be done, the sooner you 2 can get to work!
Remember, NO SURPRISE FEEDBACK at the end of the rotation!
The sooner you 2 are on the same page about the work that needs to be done, the sooner you 2 can get to work!
Remember, NO SURPRISE FEEDBACK at the end of the rotation!
13/ After feedback has been delivered, team up to devise SMART goals. Use short intervals so that you can check in soon about progress. Sit down to discuss results:
🥳If goals achieved, celebrate (+/- make new goals)
🤔If goals not achieved, reevaluate goals and strategies
🥳If goals achieved, celebrate (+/- make new goals)
🤔If goals not achieved, reevaluate goals and strategies

14/ Many colleagues and trainees are reticent to deliver tough feedback.
We should relish these opportunities as teachers.
A tough feedback convo can galvanize a relationship when trust is present & is just the beginning of a mutual journey towards improvement.
We should relish these opportunities as teachers.
A tough feedback convo can galvanize a relationship when trust is present & is just the beginning of a mutual journey towards improvement.
15/ Thanks again for joining us today! Any questions, comments, #Feedback, just reply to this tweet.
Follow @JenniferSpicer4 so you can learn about Soliciting Feedback during next #TweetorialTuesday.
Have a great week!
Follow @JenniferSpicer4 so you can learn about Soliciting Feedback during next #TweetorialTuesday.
Have a great week!
• • •
Missing some Tweet in this thread? You can try to
force a refresh