,
13 tweets,
3 min read
Read on Twitter
The next big thing that’s described in breast cancer is “receptor status”. Using IHC, tumors are stained for the estrogen receptor (ER), the progesterone receptor (PR), and Her2.
These receptors are used because they inform treatment decisions.
These receptors are used because they inform treatment decisions.
The estrogen receptor is a protein found in mammary epithelial cells. During puberty, estrogen levels increase which causes increased estrogen- estrogen receptor interaction in these cells.
When estrogen and ER bind, they go to the nucleus and bind to DNA on specific locations that will make RNA then new proteins that tell the cell to grow and divide. 

At puberty, estrogen causes the mammary glands to develop. This process continues to occur over the rise and fall of a woman’s menstrual cycle and is TIGHTLY regulated.
In cancer, the process becomes aberrant.
In cancer, the process becomes aberrant.
In breast cancer that is dependent on estrogen for growth, ER levels increase in breast cancer. We call these tumors estrogen receptor positive or ER+.
One of the proteins that ER-estrogen helps make is the progesterone receptor (PR). As a result, tumors are usually also PR+.
One of the proteins that ER-estrogen helps make is the progesterone receptor (PR). As a result, tumors are usually also PR+.
Amazingly intelligent scientists recognized that estrogen drives breast cancer growth in ER+ breast cancers (about 70% of all breast cancer) and developed drugs that block estrogen signaling.
There are 3 main classes of ER-targeted therapy (aka endocrine therapy aka anti-estrogens):
1. Selective estrogen receptor modulators (SERMS) including Tamoxifen that bind ER to prevent estrogen from binding.
1. Selective estrogen receptor modulators (SERMS) including Tamoxifen that bind ER to prevent estrogen from binding.

2. Aromatase inhibitors (AI) that prevent estrogen from being made. (Aromatase is the enzyme - or protein - that converts testosterone into estrogen.)
3. Selective estrogen receptor degraders (SERDs) that degrade the estrogen receptor.
3. Selective estrogen receptor degraders (SERDs) that degrade the estrogen receptor.
Her2 is epidermal growth factor receptor 2. It is a protein found on the cell surface that interacts with other members of the Her family proteins. Together, they form a “dimer” and send a message to the cell to grow and divide.
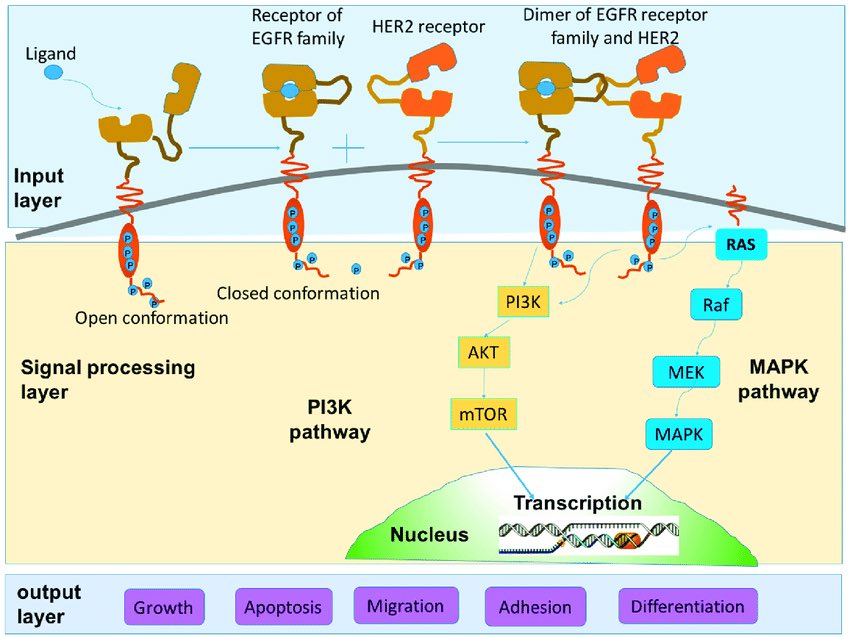
In Her2-positive (Her2+) breast cancer, Her2 is amplified.
This means there are extra copies of the DNA that the Her2 protein is made from, which leads to an excess of Her2 protein production (and more growth).
This means there are extra copies of the DNA that the Her2 protein is made from, which leads to an excess of Her2 protein production (and more growth).

There are drugs that block Her2 signaling:
1. Antibodies including Herceptin & Perjeta that block interactions and can cause the immune system to respond
2. Small molecule inhibitors including Tykerb that prevent signaling molecules from interacting with members of the Her family
1. Antibodies including Herceptin & Perjeta that block interactions and can cause the immune system to respond
2. Small molecule inhibitors including Tykerb that prevent signaling molecules from interacting with members of the Her family
3. Antibody-drug conjugates like Kadcyla that bind to Her2 on the outside of the cell which allows the drug (chemotherapy) to enter the cell.

The three main receptor statuses are:
1. ER+
2. Her2+
3. Triple negative
1 and 2 have targeted therapies as I just described. As of now, the option for triple negative patients is non-specific chemotherapy. (Which some patients with ER+ and Her2+ cancer also receive.)
1. ER+
2. Her2+
3. Triple negative
1 and 2 have targeted therapies as I just described. As of now, the option for triple negative patients is non-specific chemotherapy. (Which some patients with ER+ and Her2+ cancer also receive.)