,
17 tweets,
10 min read
Read on Twitter
1/
#Dermatology #tweetorial time! Let's spend some time on the autoimmune blistering diseases. There are many, so this will be a broad overview of the approach to a the bullous disease patient.
#dermtwitter #FOAMed #medtwitter #medstudenttwitter #MedEd @healourskin pc:@dermnetnz
#Dermatology #tweetorial time! Let's spend some time on the autoimmune blistering diseases. There are many, so this will be a broad overview of the approach to a the bullous disease patient.
#dermtwitter #FOAMed #medtwitter #medstudenttwitter #MedEd @healourskin pc:@dermnetnz
2/
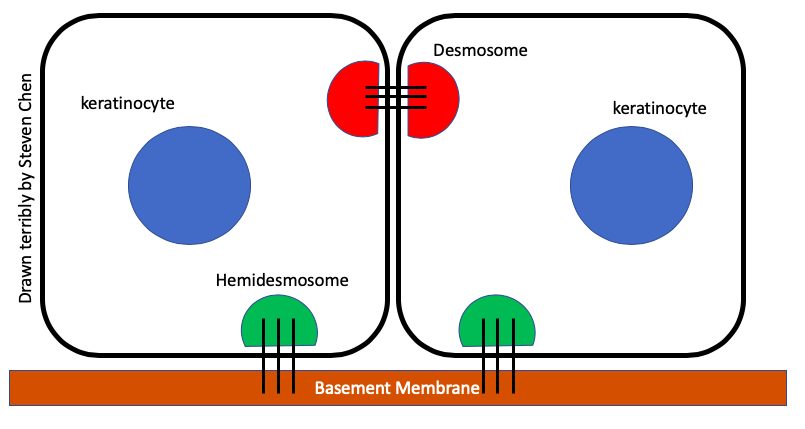
The first ? we usually ask: "What is the level of the split?" That helps to distinguish between the #pemphigus group of diseases where the desmosome is involved in the epidermis, and the #pemphigoid group where the hemi-desmosome is involved at the basement membrane zone.
The first ? we usually ask: "What is the level of the split?" That helps to distinguish between the #pemphigus group of diseases where the desmosome is involved in the epidermis, and the #pemphigoid group where the hemi-desmosome is involved at the basement membrane zone.
3/
This correlates with the exam! Higher up in the epidermis means a thinner walled blister that's more fragile. So these are usually flaccid bullae. Deeper down means tense bullae. Photo 1 is pemphigus - see how droopy the bulla is? Vs photo 2 of pemphigoid, which stands up.
This correlates with the exam! Higher up in the epidermis means a thinner walled blister that's more fragile. So these are usually flaccid bullae. Deeper down means tense bullae. Photo 1 is pemphigus - see how droopy the bulla is? Vs photo 2 of pemphigoid, which stands up.


4/
The caveat is that over time, any bulla will start to droop and look flaccid. Also, any vesicle or bulla that lasts long enough will also fill with pus! We can use other clues to help us make the diagnosis, like checking for a Nikolsky. How do you check for Nikolsky again?
The caveat is that over time, any bulla will start to droop and look flaccid. Also, any vesicle or bulla that lasts long enough will also fill with pus! We can use other clues to help us make the diagnosis, like checking for a Nikolsky. How do you check for Nikolsky again?
5/
A positive Nikolsky means you rubbed next to a blister and made a new one! The related "indirect Nikolsky" is pushing down on a blister & making it spread bigger (aka Asboe-Hansen sign). However, not everything that has a positive NIkolsky is pemphigus! What other dz has it?
A positive Nikolsky means you rubbed next to a blister and made a new one! The related "indirect Nikolsky" is pushing down on a blister & making it spread bigger (aka Asboe-Hansen sign). However, not everything that has a positive NIkolsky is pemphigus! What other dz has it?
6/
Although a different pathophysiologic mechanism, SJS/TEN also has a positive Nikolsky, because the entire epidermis has died and falls off. But this is mediated through cell death, as opposed to the blistering disorders, which are antibody mediated.
Although a different pathophysiologic mechanism, SJS/TEN also has a positive Nikolsky, because the entire epidermis has died and falls off. But this is mediated through cell death, as opposed to the blistering disorders, which are antibody mediated.

7/
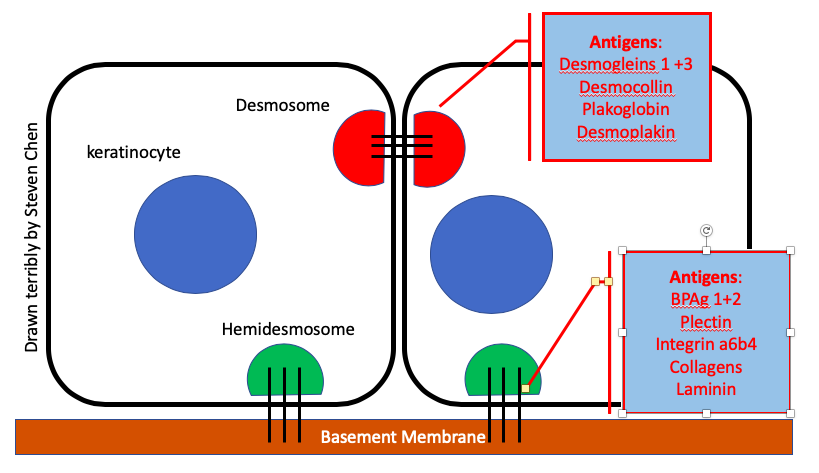
For the most part, every blistering disorder has an Ag that is targeted by some Ab. The common ones:
Bullous Pemphigoid (BP): BPAg1 & BPAg2
Pemphigus Vulgaris (PV): Desmoglein (Dsg) 3 +/- 1
Pemphigus Foliaceous: Dsg 1 only
If you're going into #derm, you'll need to know more!
For the most part, every blistering disorder has an Ag that is targeted by some Ab. The common ones:
Bullous Pemphigoid (BP): BPAg1 & BPAg2
Pemphigus Vulgaris (PV): Desmoglein (Dsg) 3 +/- 1
Pemphigus Foliaceous: Dsg 1 only
If you're going into #derm, you'll need to know more!
8/
Ask about & examine the oropharynx & other mucosal sites. Although we classically think of PV with this, a recent @JAMADerm paper showed >17% of BP pts also have it, & was associated with more aggressive dz phenotype! A thorough ROS is important!
jamanetwork.com/journals/jamad…
Ask about & examine the oropharynx & other mucosal sites. Although we classically think of PV with this, a recent @JAMADerm paper showed >17% of BP pts also have it, & was associated with more aggressive dz phenotype! A thorough ROS is important!
jamanetwork.com/journals/jamad…
9/
If pts have mucosal dz, it is important to be extra careful w/ counseling. Certain foods can be really difficult to eat, pts lose weight, & often require more aggressive therapy. If mucosal dz is all they have, partnering with other specialists is crucial (eg: ENT, ophtho).
If pts have mucosal dz, it is important to be extra careful w/ counseling. Certain foods can be really difficult to eat, pts lose weight, & often require more aggressive therapy. If mucosal dz is all they have, partnering with other specialists is crucial (eg: ENT, ophtho).
10/
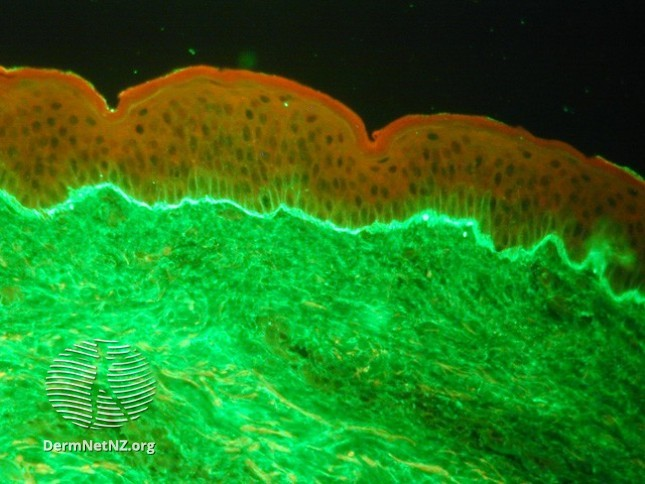
Work up includes a biopsy for H+E & Direct immunofluroescence (DIF). That's where we bx the patient's skin, & incubate it with an fluorescent tagged antibody targeting Immunoglobulins, such that any part of their skin that has antibodies or complement attached will light up!
Work up includes a biopsy for H+E & Direct immunofluroescence (DIF). That's where we bx the patient's skin, & incubate it with an fluorescent tagged antibody targeting Immunoglobulins, such that any part of their skin that has antibodies or complement attached will light up!
11/
This is in contrast to an indirect immunofluroescence, which is rarely done (usually when the DIF is equivocal). In this case, we take patient serum and incubate it with a substrate rich with target antigens. Then we do the same tagging like in the DIF to see what lights up!
This is in contrast to an indirect immunofluroescence, which is rarely done (usually when the DIF is equivocal). In this case, we take patient serum and incubate it with a substrate rich with target antigens. Then we do the same tagging like in the DIF to see what lights up!

12/
Now, we can also check for antibodies that target Dsg 1/3, as well as those that target BPAg1/2, directly from the blood. This is another piece of the puzzle in deciding how to treat your patient. There are some data to link titers to disease course.
jamanetwork.com/journals/jamad…
Now, we can also check for antibodies that target Dsg 1/3, as well as those that target BPAg1/2, directly from the blood. This is another piece of the puzzle in deciding how to treat your patient. There are some data to link titers to disease course.
jamanetwork.com/journals/jamad…
13/
The tx of these diseases is complicated and often requires subspecialty care; #Dermatologists should be involved. The tx can range from anti-inflammatory (eg: tetracycline abx + niacinamide), or infusions (eg: rituximab)! R/b/a need to be discussed frankly with the patient.
The tx of these diseases is complicated and often requires subspecialty care; #Dermatologists should be involved. The tx can range from anti-inflammatory (eg: tetracycline abx + niacinamide), or infusions (eg: rituximab)! R/b/a need to be discussed frankly with the patient.
14/
Since so many of our treatments are immunosuppressive, it's important to screen patients for certain diseases, like hepatitis and TB, so that we don't inadvertently cause reactivation. Patients also need to know about their suppressed immunity so counseling is a big part!
Since so many of our treatments are immunosuppressive, it's important to screen patients for certain diseases, like hepatitis and TB, so that we don't inadvertently cause reactivation. Patients also need to know about their suppressed immunity so counseling is a big part!
15/
It's important to remember that not all cases are idiopathic. Some are drug-induced, & some can be paraneoplastic. Before embarking on a treatment plan, be sure to ask about new medications, dose changes, & make sure cancer screening is considered.
jaad.org/article/S0190-…
It's important to remember that not all cases are idiopathic. Some are drug-induced, & some can be paraneoplastic. Before embarking on a treatment plan, be sure to ask about new medications, dose changes, & make sure cancer screening is considered.
jaad.org/article/S0190-…
16/To Recap:
- Autoimmune blistering dzs occur when antibodies attack the "glue" that holds the skin together.
- The exam is critical for diagnosis. Biopsies and blood work help confirm.
- Be sure to consider possible triggers before treatment.
- Involve a #dermatologist to help!
- Autoimmune blistering dzs occur when antibodies attack the "glue" that holds the skin together.
- The exam is critical for diagnosis. Biopsies and blood work help confirm.
- Be sure to consider possible triggers before treatment.
- Involve a #dermatologist to help!
17/17
Thanks for joining me! Remember there is a ton more to say about these diseases. If you're interested (and a #medstudent), you should think about joining us in #derm! These patients can be very sick, and being able to provide the care they need is unbelievably rewarding!
Thanks for joining me! Remember there is a ton more to say about these diseases. If you're interested (and a #medstudent), you should think about joining us in #derm! These patients can be very sick, and being able to provide the care they need is unbelievably rewarding!