Inpatient Service Day 6! Which means my 6th consecutive #MedThread of this #BreadNButterMedicine series.
Today's topic: Utility of Fecal Occult Blood Testing (FOBT) in the inpatient setting.
TL;DR - You probably shouldn't be doing them.
Today's topic: Utility of Fecal Occult Blood Testing (FOBT) in the inpatient setting.
TL;DR - You probably shouldn't be doing them.
2/ (Poll) Do you ROUTINELY order FOBT as an inpatient test?
3/ As always, let's dive a little into the background of what FOBT testing is. This is a test that was developed for and then traditionally used in outpatient colorectal cancer (CRC) screening. If used as screening the USPSTF recommends screening annually. uspreventiveservicestaskforce.org/Page/Document/… 
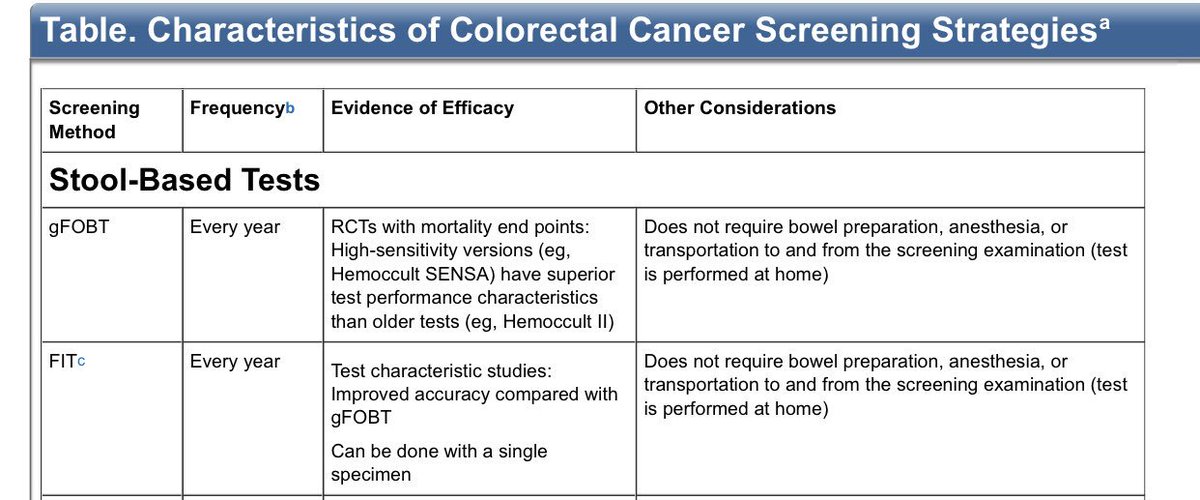
4/ There are two types of testing which most consider FOBT.
☝🏼 gFOBT is Guiac-based testing that tests for the heme component of hemoglobin.
✌🏼 FIT is an immunochemical test for the globin component of hemoglobin
☝🏼 gFOBT is Guiac-based testing that tests for the heme component of hemoglobin.
✌🏼 FIT is an immunochemical test for the globin component of hemoglobin
5/ gFOBT works by detecting pseudoperoxidase in hemoglobin. A positive result occurs if the testing paper containing a stool specimen turns blue after adding the developer. en.wikipedia.org/wiki/Stool_gua…
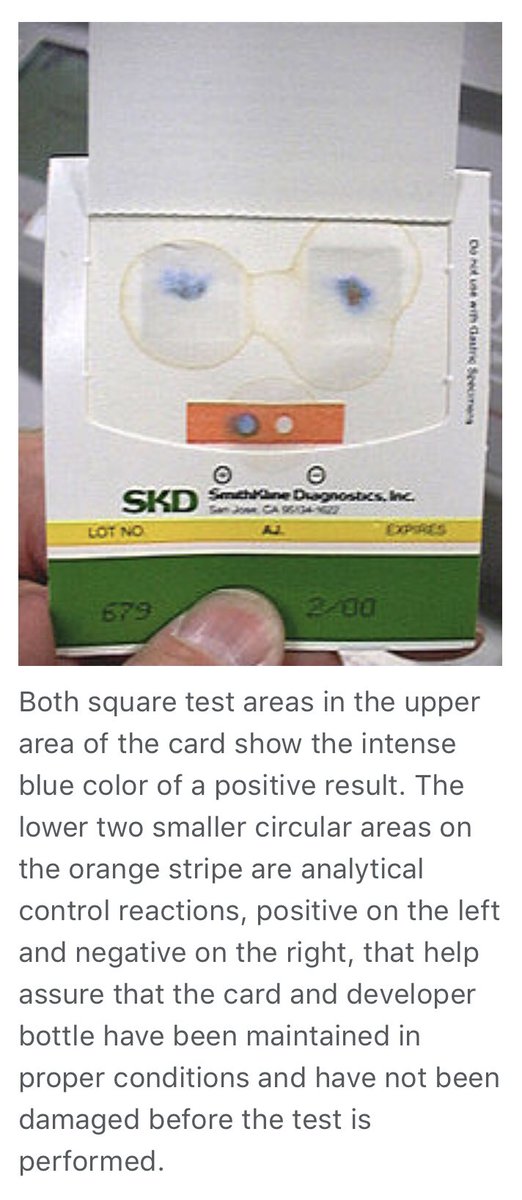
6/ The active component of guaiac paper is alpha-guaiaconic acid and the active component of the developer is hydrogen peroxide. If a fecal sample contains hemoglobin, the peroxidase activity of heme catalyzes a reaction to form a blue colored quinone within a few seconds.

7/ FIT uses antibodies detecting the globin component of hemoglobin instead of heme like the gFOBT. Globin is broken down and decreased during intestinal transit by digestive enzymes and gastric acid and therefore FIT testing is more specific for lower GI bleeding.
8/ Unfortunately gFOBT can produce false results.
False Positives for CRC can be caused by medications that cause clinically insignificant GI blood loss (ASA, NSAIDs, EtOH), iron supplements, red meat & veggies like broccoli/cauliflower (due to peroxidase or catalase activity).
False Positives for CRC can be caused by medications that cause clinically insignificant GI blood loss (ASA, NSAIDs, EtOH), iron supplements, red meat & veggies like broccoli/cauliflower (due to peroxidase or catalase activity).
9/ False Negatives can be caused by Vitamin C 🍊🍊🍊🍊
10/ Here's a more comprehensive table that presents the causes of inaccurate FOBT. (I don't remember where I got this table for citation, sorry)

11/ The risks of false positives and false negatives are why it is recommended to avoid previously mentioned foods for up to 3 days prior to testing. Also, abstinence of meds like NSAIDs are recommended as well.
12/ So why would one want to use FOBT in the inpatient setting? There may be a variety of reasons one might rationalize:
💩 Concerns for GI Bleed
💩 Work-up for anemia
💩 Iron deficiency
💩 Non-bloody diarrhea
💩 Colorectal cancer screening
💩 pre-anticoagulation initiation
Etc.
💩 Concerns for GI Bleed
💩 Work-up for anemia
💩 Iron deficiency
💩 Non-bloody diarrhea
💩 Colorectal cancer screening
💩 pre-anticoagulation initiation
Etc.
13/ What are the pitfalls of using FOBT in a setting that it was not intended?
1️⃣ Can't control for the food restrictions that can cause false positives and negatives
2️⃣ Hospitalized patients are already high risk for occult GI bleeding due to comorbidity
1️⃣ Can't control for the food restrictions that can cause false positives and negatives
2️⃣ Hospitalized patients are already high risk for occult GI bleeding due to comorbidity
14/
3️⃣ Hospitalized patients are often on multiple drugs which may confound results
4️⃣ Bleeding from the GI tract may be intermittent and a negative result cannot exclude presence of occult bleeding
onlinelibrary.wiley.com/doi/pdf/10.111…
3️⃣ Hospitalized patients are often on multiple drugs which may confound results
4️⃣ Bleeding from the GI tract may be intermittent and a negative result cannot exclude presence of occult bleeding
onlinelibrary.wiley.com/doi/pdf/10.111…
15/ Lastly the most important question: Does testing actually impact management decisions anyways?
This 2014 study found that the majority of patients suspected of GIB underwent endoscopy regardless of FOBT results. ncbi.nlm.nih.gov/pubmed/2531435…
This 2014 study found that the majority of patients suspected of GIB underwent endoscopy regardless of FOBT results. ncbi.nlm.nih.gov/pubmed/2531435…
16/ What should we do instead?
A 2017 TWDFNR article offers:
1️⃣ Take a careful history and exam
2️⃣ Consider a visual inspection of stool (observed melena has likelihood ratio of 25, patient report melena has LR+ of 5-6)
3️⃣ UGIB may have elevated BUN:Cr ratio (>30 has LR+ of 7.5)
A 2017 TWDFNR article offers:
1️⃣ Take a careful history and exam
2️⃣ Consider a visual inspection of stool (observed melena has likelihood ratio of 25, patient report melena has LR+ of 5-6)
3️⃣ UGIB may have elevated BUN:Cr ratio (>30 has LR+ of 7.5)
FIN/ Summary:
💥FOBT is a CRC screening tool and not a really a diagnostic test for GI bleeding
💥FOBT is plagued by poor sensitives, poor specificity, false positives and false negatives for this purpose
💥FOBT doesn't seem to actually impact Medical Decision Making
(POLL)
💥FOBT is a CRC screening tool and not a really a diagnostic test for GI bleeding
💥FOBT is plagued by poor sensitives, poor specificity, false positives and false negatives for this purpose
💥FOBT doesn't seem to actually impact Medical Decision Making
(POLL)
For those coming to this late, you can start from day 1 of my #MedThreads: