,
29 tweets,
8 min read
Read on Twitter
What are the Epidemiologic Signatures in Cancer? A new special report out in NEJM by Gil Welch, Barnett Kramer, and William Black is so good I had to do a #tweetorial. nejm.org/doi/full/10.10…
👇🏾👇🏾👇🏾
👇🏾👇🏾👇🏾
TL;DR -- The MAJOR takeaway doctors and trainees should get from this article is this:
Cancer incidence is an UNRELIABLE measure of cancer burden.
Cancer incidence is an UNRELIABLE measure of cancer burden.
Using data from SEER, which essentially serves as the cancer registry of the United States, authors show trends in cancer mortality, incidence, and metastatic incidence between 1975 and 2015. 

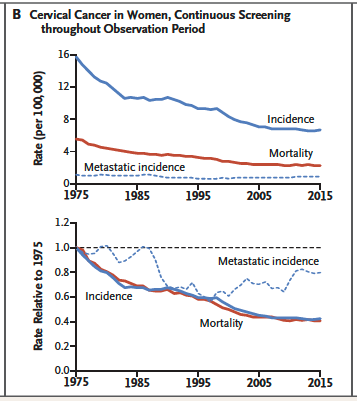
Importantly, authors make use of a pair of graphics. The first depicts the absolute rates (age adjusted) over time, the second depicts the relative rates over time with 1975 as the reference group.
By examining these trends in multiple cancer types, Welch et al show how mortality, incidence, and metastatic incidence curves (i.e. their epidemiologic signature) can provide insight into true cancer occurrence, overdiagnosis, and treatment advances.
The authors grouped 11 different cancers: Hodgkin’s lymphoma, CML, melanoma, lung, stomach, cervical, colorectal, thyroid, prostate, breast and kidney cancers into 3 categories:
1.Desirable signatures
2.Undesirable signatures
3.Signatures with mixed signals
1.Desirable signatures
2.Undesirable signatures
3.Signatures with mixed signals
Let’s dive into these categories….
In the desirable category: Hodgkin lymphoma, CML, and Lung cancer. Advances in medical care and efforts at cancer risk factor reduction are likely responsible for declining mortality.
In Hodgkin’s lymphoma, the steady decline in mortality — contrasted with generally stable
incidence — reflects a steady improvement in treatment. This is compared to the stable incidence in CML and RAPID decline in mortality coinciding with the introduction of imatinib.
incidence — reflects a steady improvement in treatment. This is compared to the stable incidence in CML and RAPID decline in mortality coinciding with the introduction of imatinib.

Imatinib is what a really revolutionary, breakthrough, gamechanging…*insert your favorite medical hyperbole*…drug looks like. Wow.
In Lung cancer, another cancer with a desirable epi signature, trends show the importance of eliminating a POWERFUL risk factor that causes cancer. Smoking!!!

It’s important to appreciate how the relative changes in incidence and mortality are perfectly superimposed in lung cancer. They move together perfectly, likely tracking with the rise and fall of cigarette smoking!
The peaks for men and women are different because prevalence of ever smoking peaked during the 1950s among men and 1970s among women. Cigarette companies began targeting women more aggressively in the 1960s.
Also, in the desirable signature category reflecting variable screening practices are: stomach, cervical, and colorectal cancers.
In stomach cancer, in which there has been no screening, incidence and mortality have fallen in tandem, perhaps because of the decline in Helicobacter Pylori infection, a consistent risk factor for gastric carcinoma.

Cervical cancer incidence/mortality declined due to screening via pap smears leading to early detection and treatment of precancerous lesions. HPV infection is a potent risk factor for cervical cancer, so the Gardasil vaccine will likely further these declines in the future.
The declining incidence and mortality in colon cancer can be explained in part due to screening efforts, however, declines were already in motion before widespread colorectal cancer screening was adopted.

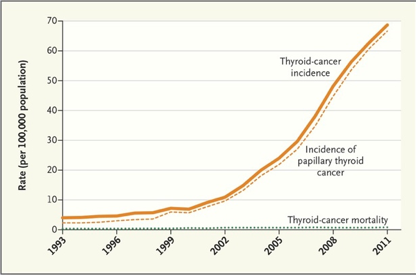
Now let’s look at some UNDESIRABLE signatures: there is something REALLY different: DISCORDANCE. Rising incidence with stable mortality = overdiagnosis.
This signature concerning for overdiagnosis and can be illustrated by thyroid cancer, kidney cancer, and melanoma.

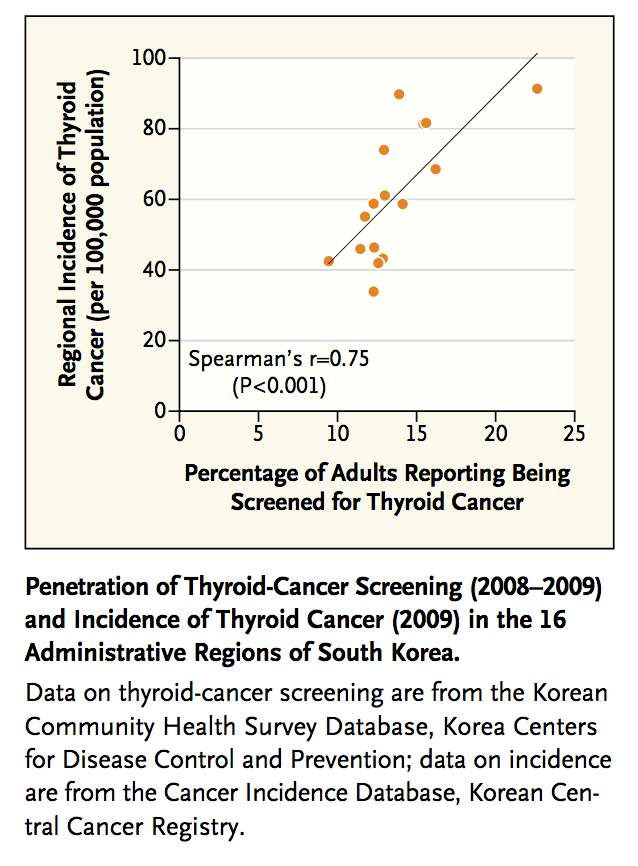
These are highly scrutiny dependent cancers in which the more you look, the more you find, with no improvement in mortality at a population level.
In a study of thyroid cancer incidence in South Korea, exposure to screening lead to an explosion in incidence without a commensurate change in mortality. See: nejm.org/doi/full/10.10…
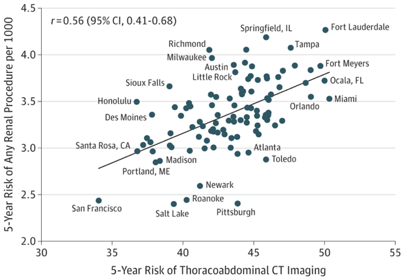
In kidney cancer, CT scans are likely responsible for picking up incidental kidney growths that would have not otherwise harmed the patients. See:
jamanetwork.com/journals/jamai…
jamanetwork.com/journals/jamai…
In melanoma, screening activities are likely largely responsible for a SIX-FOLD increase in incidence over the past 40 years with largely flat mortality. Increases in metastatic incidence may reflect increase in true underlying disease but may also be upstaging.


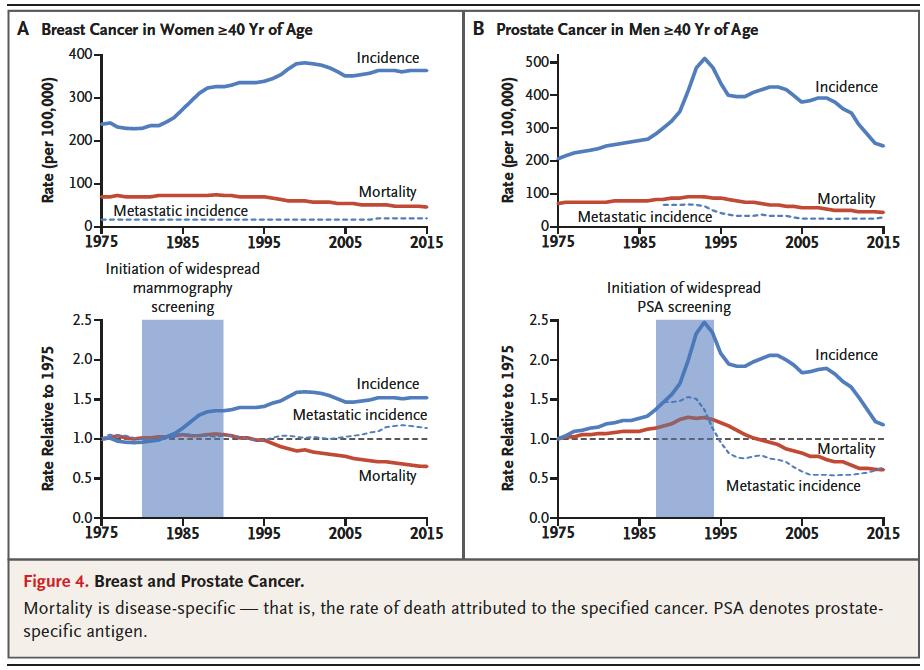
The signatures with mixed signals include breast and prostate cancer in which screening efforts have distorted incidence rates combined with improvements in treatment which have led to declines in mortality.
Moving forward Welch et al make an interesting suggestion for improving acquisition of population-based data on cancer burden by including information that captures system level effects.

For me this paper deftly explains the importance of understanding that changing incidence must be interpreted in context, particularly as it relates to mortality. Diagnosing more “cancer” is not necessarily value added if it does not result in improved morbidity or mortality.
These trends show both our triumph in cancer control through screening, treatment, and prevention (i.e. colon cancer, CML, lung cancer) and where overdiagnosis is a persistent problem (thyroid, kidney, melanoma). The last 2 sentences of the paper capture this well:

I learn so much from anything Gil Welch publishes, hope you learned something too!
Do you think Gil Welch should get on twitter?
Do you think Gil Welch should get on twitter?
Was this #tweetorial helpful?