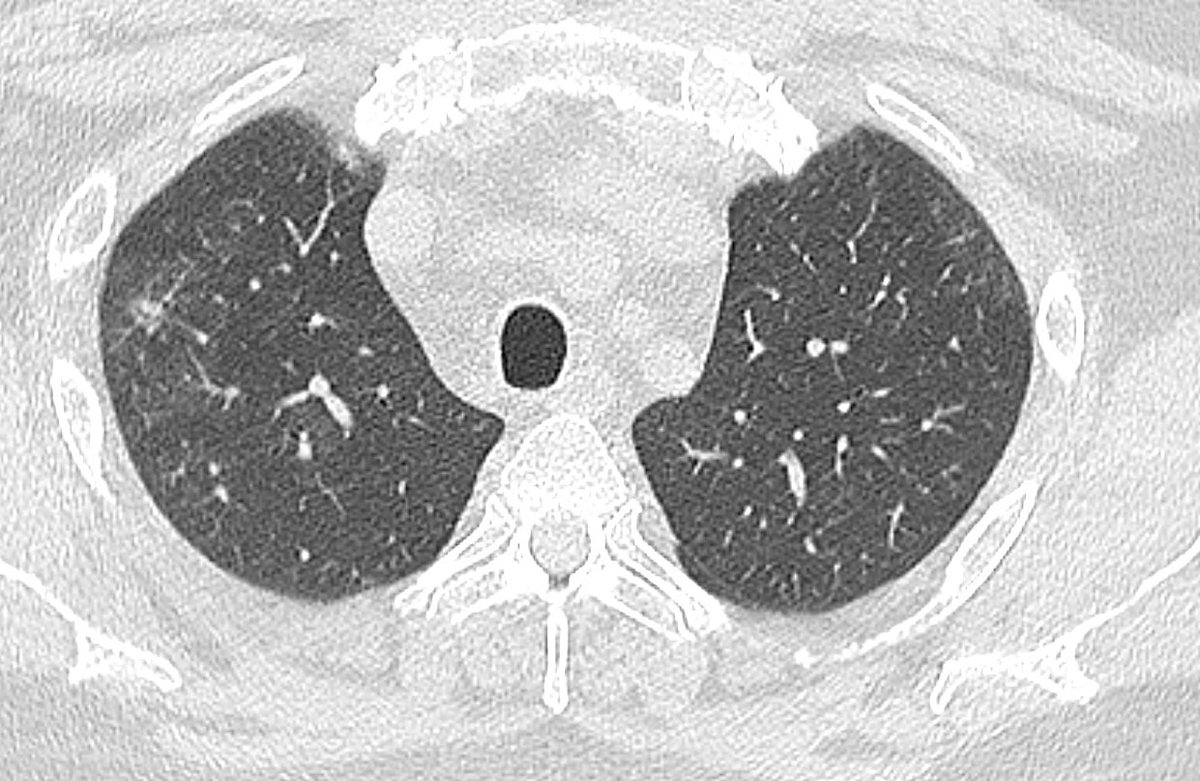
The patient is a 45 yo male. Acute kidney injury and ? Pneumonia. The first image was at presentation. There is peribronchial consolidation with a nice perilobular appearance peripherally. Looks like organising pna. Cause could be infection, vaping, drug reaction, CTD...
Here is a similar level, 7 days later. Consolidation has progressed. OP is really just a type of lung injury. If the lung injury gets worse, we could get into ARDS/AIP territory. But, no septal lines and no effusion. So just bad OP. ANA is elevated. 

Serology: ANA greater than 1:1280 nucleolar pattern. Extended panel otherwise entirely negative.
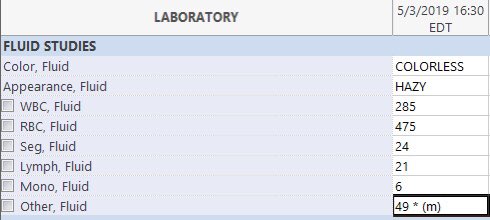
Here’s the BAL:
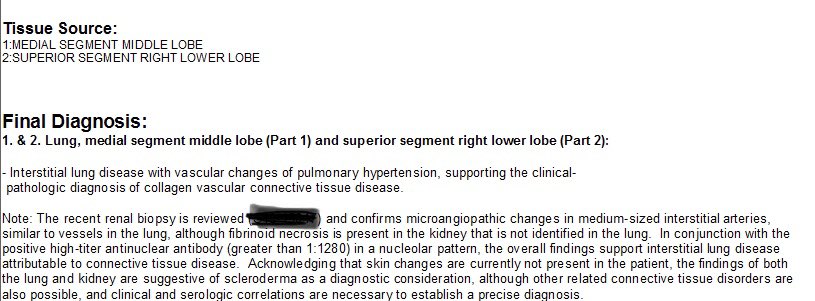
The patient was started on mycophenylate and prednisone. A trans bronchial biopsy was not revealing. VATS biopsy was performed. Here is report of microscopic findings:

So, in CTD-related ILD this peribronchial, more or less symmetric, lower zone organising pneumonia is a really typical appearance. There is a differential as above, but when I see this picture I will always recommend screening for CTD. Yes, even in men.
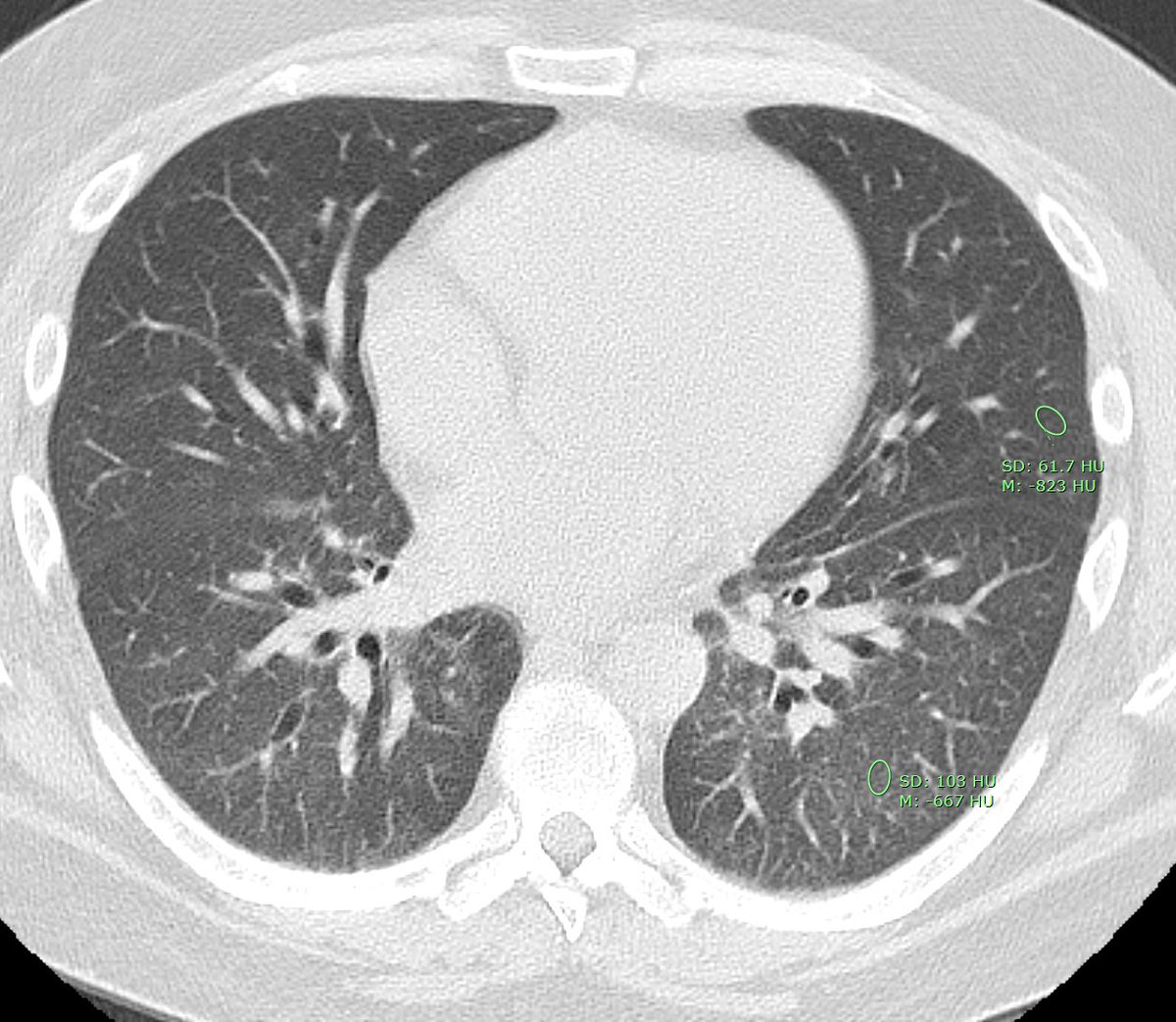
Here is the CT after 2 months of treatment. The OP has really improved. There is still some peribronchial ground glass in the lower lobes. I have measured lung density. Normal lung should be -750 to -850. So -667 is to high. Could be cells, or fine fibrosis.
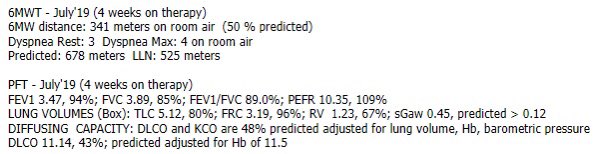
Here are PFT’s 8 weeks after starting therapy. Says 4 weeks but that is an error.
CT at 6 months. Now there is quite mild central traction bronchiectasis, and still some faint ggo.

Some degree of fibrosis is common after this degree of organising pneumonia, but it can be subtle. The pattern on CT is NSIP, and histology would also be expected to show NSIP. Here are images from the upper zone, first at time of presentation:

And at 6 months. Mild fibrosis with subpleural sparing, and probably a tiny focus of traction bronchiolectasis on the (radiological) right amid that more focal opacity.
So, clinically the patient did not meet diagnostic criteria for one of the described connective tissue diseases. So, together with the elevated ANA, imaging, renal biopsy (remember patient presented with renal failure), a diagnosis of IPAF with suspicion for scleroderma was made
WHAT the heck is IPAF?! You might say. Interstitial pneumonia with autoimmune features. Because chest. It’s not really a clinical diagnosis but a research designation, with criteria, a sort of place holder until docs smarter than me figure it out. thoracic.org/statements/res…
So, personally I find this area of chest radiology fascinating. I hope I’ve shared some of that enthusiasm, and that this approach has made this complex area a bit easier to understand. Comments or added wisdom from rads pulmonologists and pathologists welcome! /end