
1/ In honor of #COPD Awareness Month, let’s solve the prevailing problem of rare #palliativecare (PC) in COPD, especially early.
See our qual exploration of clinicians in @PalliativeMed_j
liebertpub.com/doi/abs/10.108…
Care to take a stroll?
#pallipulm @pallipulm
@atscommunity
See our qual exploration of clinicians in @PalliativeMed_j
liebertpub.com/doi/abs/10.108…
Care to take a stroll?
#pallipulm @pallipulm
@atscommunity
2/ First, a PSA:
Waiting for PC until end-stage #copd is too late & misses a golden opportunity to meet COPD patient & family needs earlier in the trajectory.
See our @AnnalsATS pub atsjournals.org/doi/abs/10.151….
@AnnalsATS will have a podcast on that soon, so stay tuned!
Waiting for PC until end-stage #copd is too late & misses a golden opportunity to meet COPD patient & family needs earlier in the trajectory.
See our @AnnalsATS pub atsjournals.org/doi/abs/10.151….
@AnnalsATS will have a podcast on that soon, so stay tuned!

3/ Contrast “late” (the status quo if at all) to “early” PC, which brings comprehensive palliative & supportive care to patients & families before end-stage disease.
Others have explored PC in COPD.
The key here is “early”.
Lots to learn from #qualitative research!
Others have explored PC in COPD.
The key here is “early”.
Lots to learn from #qualitative research!
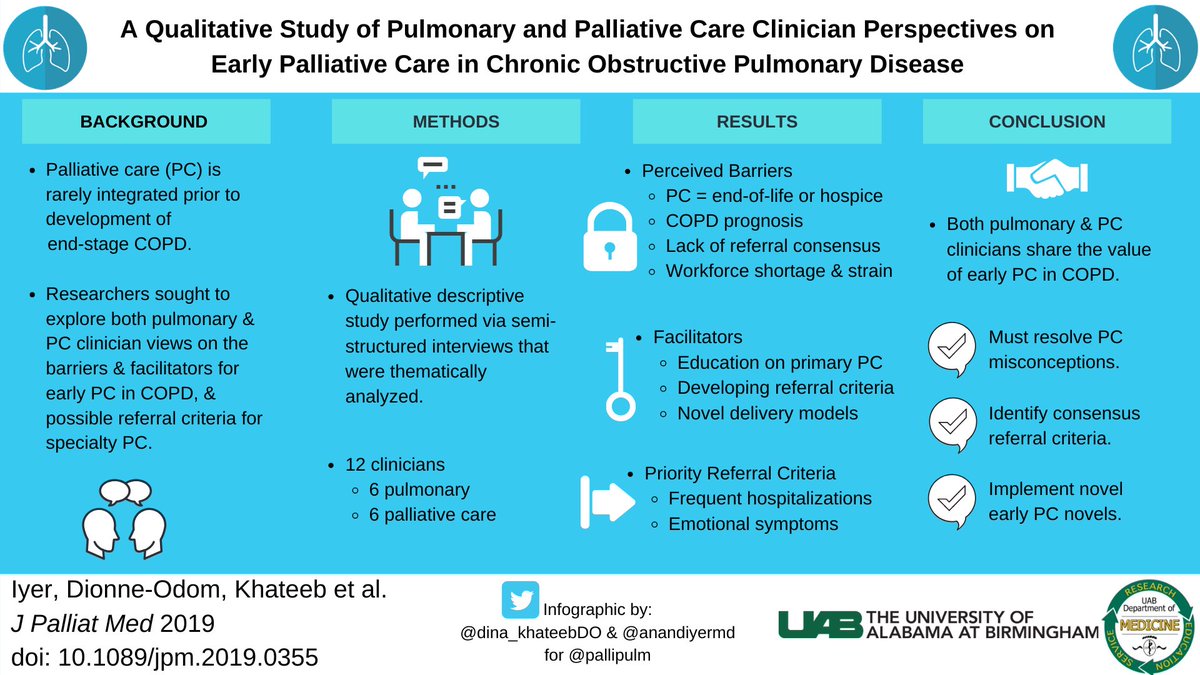
4/ This qualitative descriptive study explored pulm & PC clinician perspectives on early PC in #COPD.
We identified themes on barriers to early integration/referral within broad educational, clinical, & operational categories & explored potential early referral criteria.
We identified themes on barriers to early integration/referral within broad educational, clinical, & operational categories & explored potential early referral criteria.
5/ Major educational barriers:
1) PC is only hospice or end-of-life care. (It’s not.)
2) Insufficient training in primary PC.
An insightful pulmonologist got to the core for the specialty as did a palliative clinician (see below).
1) PC is only hospice or end-of-life care. (It’s not.)
2) Insufficient training in primary PC.
An insightful pulmonologist got to the core for the specialty as did a palliative clinician (see below).


6/ Major clinical barriers:
1) No consensus referral criteria
2) Prognosticating in COPD is difficult (what about values-based discussions instead?)
3) Resistance to palliative dyspnea meds (opioids) for fear of resp suppression in COPD (see quotes from both). This is huge!
1) No consensus referral criteria
2) Prognosticating in COPD is difficult (what about values-based discussions instead?)
3) Resistance to palliative dyspnea meds (opioids) for fear of resp suppression in COPD (see quotes from both). This is huge!


7/ Major operational barriers:
1) Not enough time in clinic for primary PC (this is a prob for everyone);
2) Inadequate reimbursement for primary PC (looking at you systems
@CMSGov)
3) Insufficient palliative workforce to handle COPD (@CTACorg @CAPCpalliative #pcheta)
1) Not enough time in clinic for primary PC (this is a prob for everyone);
2) Inadequate reimbursement for primary PC (looking at you systems
@CMSGov)
3) Insufficient palliative workforce to handle COPD (@CTACorg @CAPCpalliative #pcheta)
8/ Major facilitators included:
1) More primary PC training in pulmonary (working on this through @atscommunity and @pallipulm)
2) Consensus referral criteria
3) Innovative delivery models, i.e. telehealth, nurse-led, embedded, etc.
1) More primary PC training in pulmonary (working on this through @atscommunity and @pallipulm)
2) Consensus referral criteria
3) Innovative delivery models, i.e. telehealth, nurse-led, embedded, etc.
9/ Finally, hospitalizations and emotional symptoms were priority PC referral criteria shared by both discipline.
Others were raised (oxygen, dyspnea, weight loss, pain, surprise question, etc).
These guide future work to move referral earlier. Symptom- or FEV1-based or both?
Others were raised (oxygen, dyspnea, weight loss, pain, surprise question, etc).
These guide future work to move referral earlier. Symptom- or FEV1-based or both?
10/ This work begins to shift the needle earlier, but more work is needed.
Thanks to @PalliativeMed_j & co-authors: @MBakitas @N_DionneOdomPhD @dina_khateebDO @realmdransfield
Comments?
@JoshFessel @KaminskiMed @ctsinclair @acderinger @kpedmonds @arifkamalmd @DianeEMeier
Thanks to @PalliativeMed_j & co-authors: @MBakitas @N_DionneOdomPhD @dina_khateebDO @realmdransfield
Comments?
@JoshFessel @KaminskiMed @ctsinclair @acderinger @kpedmonds @arifkamalmd @DianeEMeier











