2/I was trained by conservative cardiologists in the post-COURAGE era. I don't offer PCI to stable patients with the idea that I am going to make them live longer or reduce hard endpoints. We offer PCI to stable patients for one predominant reason - symptoms despite meds.
3/However, it is VERY common for patients to be surprised that walking around with a blocked artery is safe. Even after a clear conversation about what the benefits of elective PCI are, post-PCI patients will often say, "Now I can walk around without worrying...".
4/What they're worried about is having the "big one". I've already tried to disabuse many of this notion, but this idea that open arteries are inherently safer than blocked ones is deeply human. I'm always surprised ppl think the root cause predominantly driven by $ incentives.
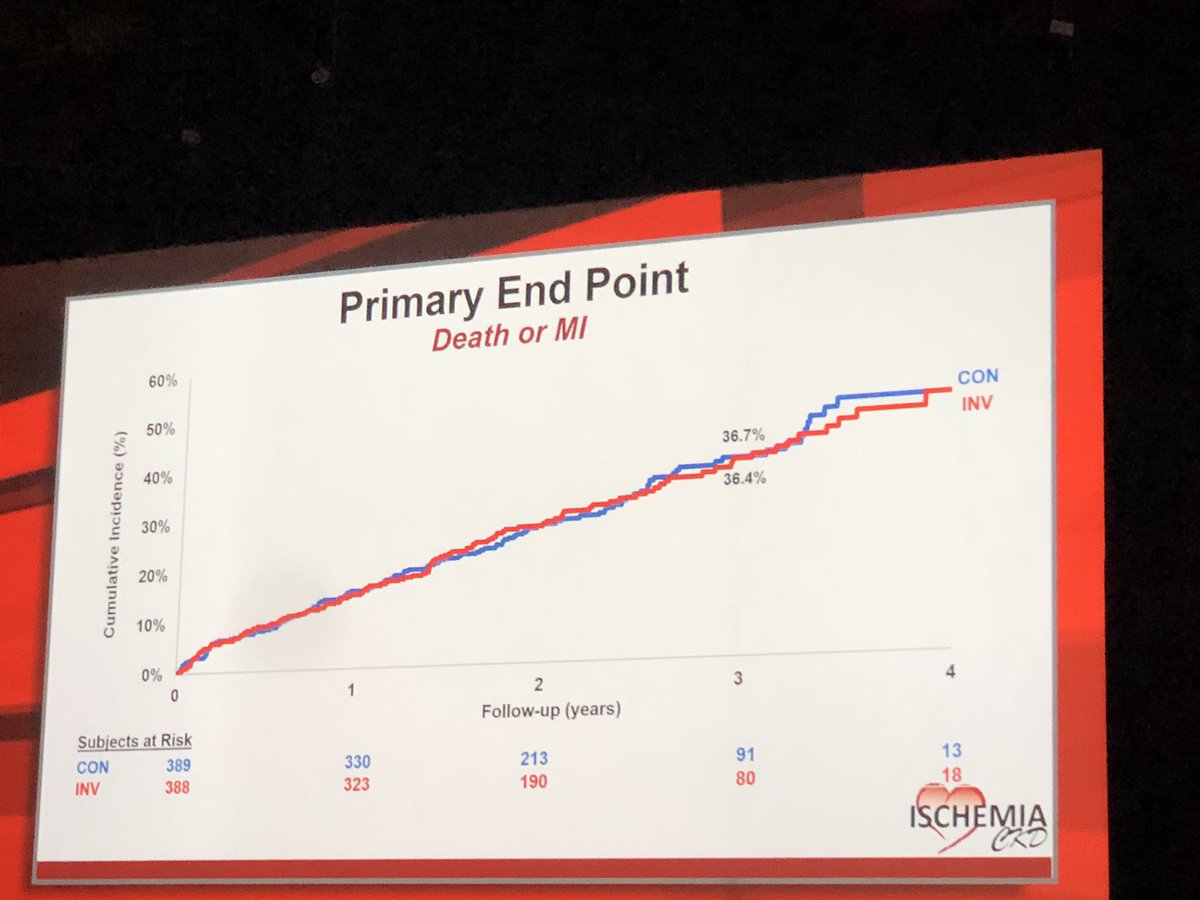
5/So a negative #ISCHEMIA trial for hard endpoints is consistent what I already believe and try to espouse to patients. It'll provide more robust evidence to support to my current practice. It'll hopefully help with pt conversations and providing reassurance.
6/One area where we more commonly think about the prognostic importance of ischemia is 3VD . It would be a big change to not send patients to CABG with extensive MVD. But this will be a subgroup analysis with short f/u - not sure that the trial should change that practice here
7/If treating ISCHEMIA in stable patients DOES reduce hard endpoints, then I'll be looking closely to see if this was driven mostly by the 3VD/CABG type of patients (which would not be surprising or practice changing)
8/But if they find consistent results across the spectrum of disease severity for both PCI/CABG treated patients, then I'll have to change my conversation and let patients know, "yes you're right, walking around with that blockage that is causing ischemia isn't good for you."
9/Most of the practice change of a negative trial seems like it will come upstream of an interventional cardiologist like me (no generally cards practice). Reflexive caths for positive stress tests, esp in minimally or asymptomatic pts, might go away. We should all welcome that.
10/So if you're an evidence-based patient-centered interventional cardiologist, I personally think you can rest comfortably whatever the results of the trial show. I'm trying to go in with an open mind and no agenda.
It's the spin cycle that I'm more worried about.... end.
It's the spin cycle that I'm more worried about.... end.