In this thread, I will compile my medical illustrations in oncology and #RadOnc.
Many are from textbook w @DanTrifMD
amazon.com/Absolute-Clini…
based on @ARRO_org study guide for board exams.
A picture is worth 1000 words.
Here is oncology in a few pics.
Many are from textbook w @DanTrifMD
amazon.com/Absolute-Clini…
based on @ARRO_org study guide for board exams.
A picture is worth 1000 words.
Here is oncology in a few pics.
@DanTrifMD @ARRO_org @SpringerNature Starting with pediatrics:
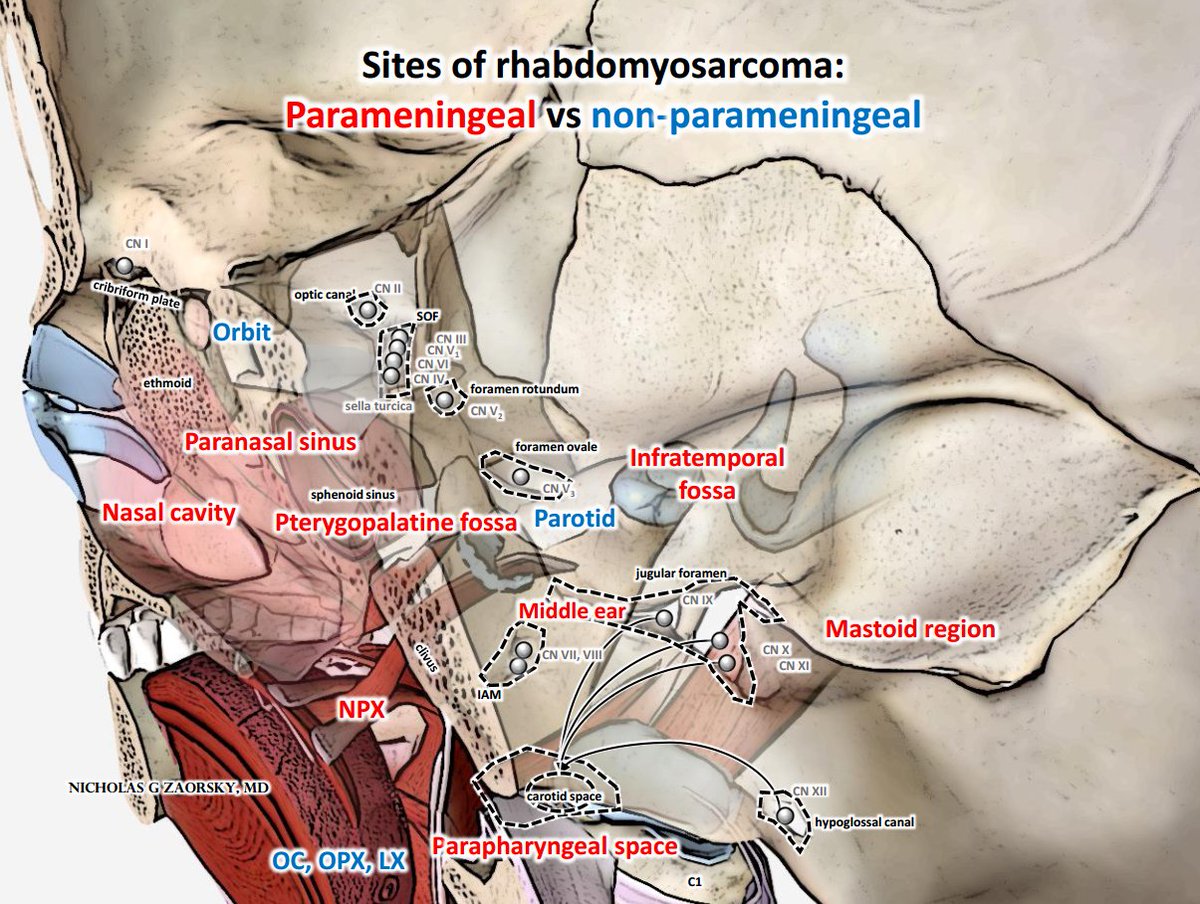
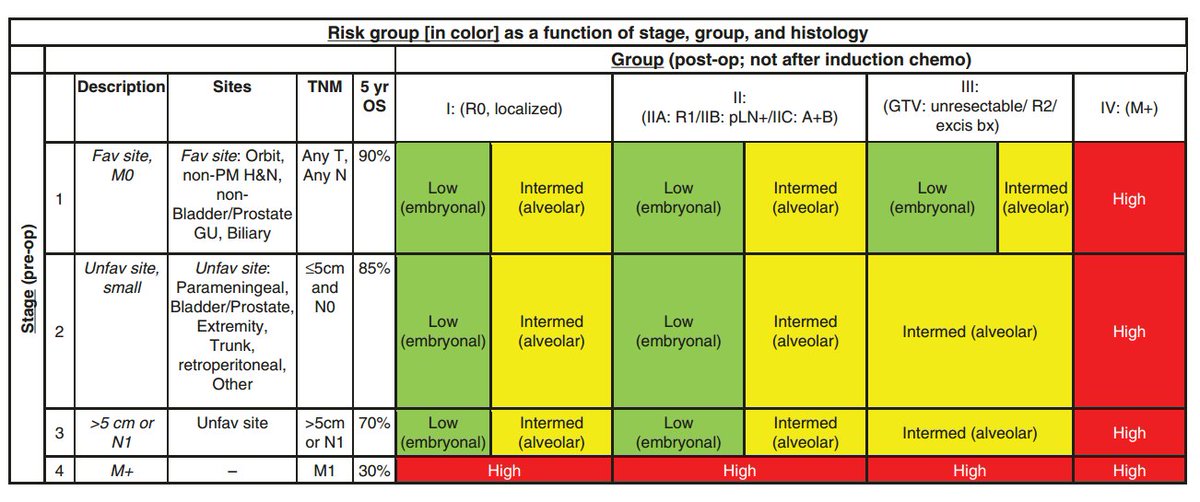
Rhabdomyosarcoma treatment paradigm for cancers of head/neck depends on parameningeal vs non-parameningeal location. PM is an unfavorable site, affects stage. #sarcoma #HNCSM
Rhabdomyosarcoma treatment paradigm for cancers of head/neck depends on parameningeal vs non-parameningeal location. PM is an unfavorable site, affects stage. #sarcoma #HNCSM
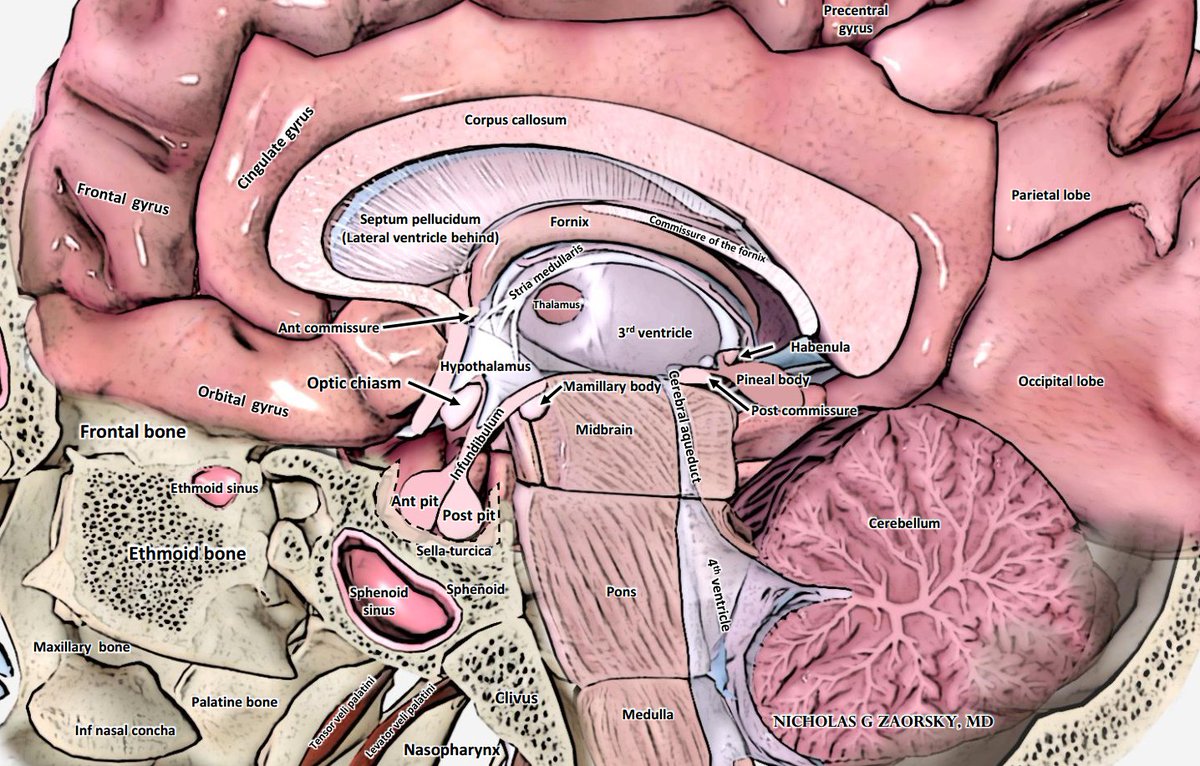
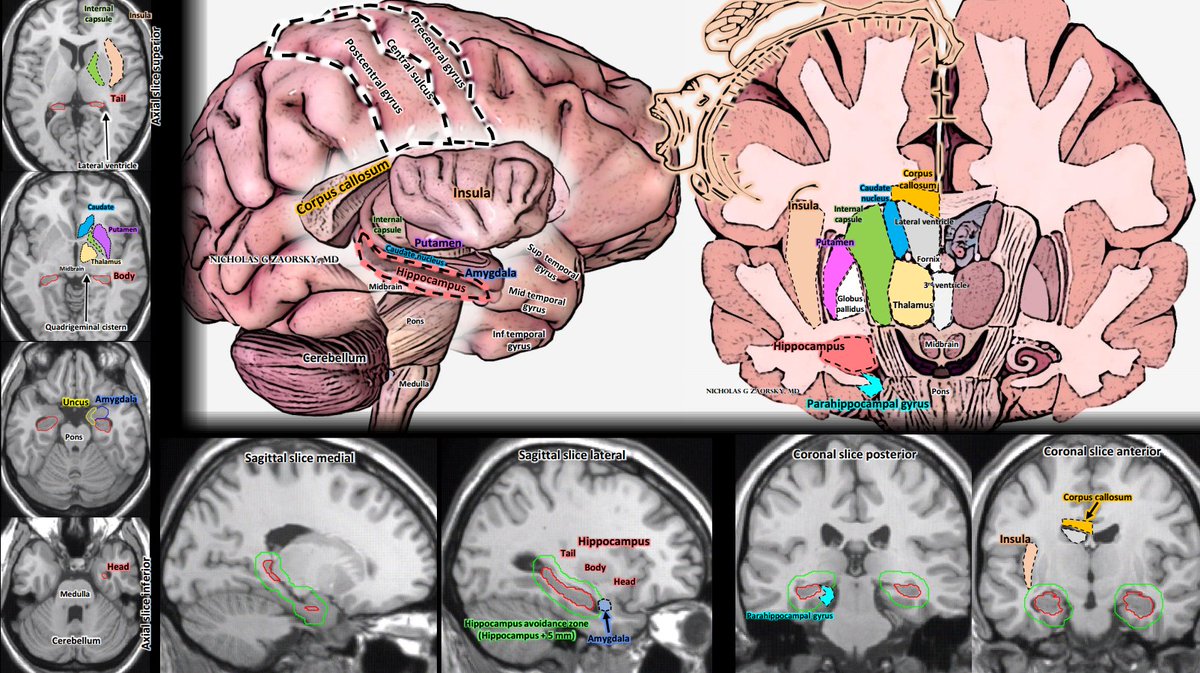
@DanTrifMD @ARRO_org @SpringerNature CNS/brain anatomy from sagittal view.
#BTSM
Chapter from @cgr0105, Sameer Nath, from University of Colorado
#BTSM
Chapter from @cgr0105, Sameer Nath, from University of Colorado
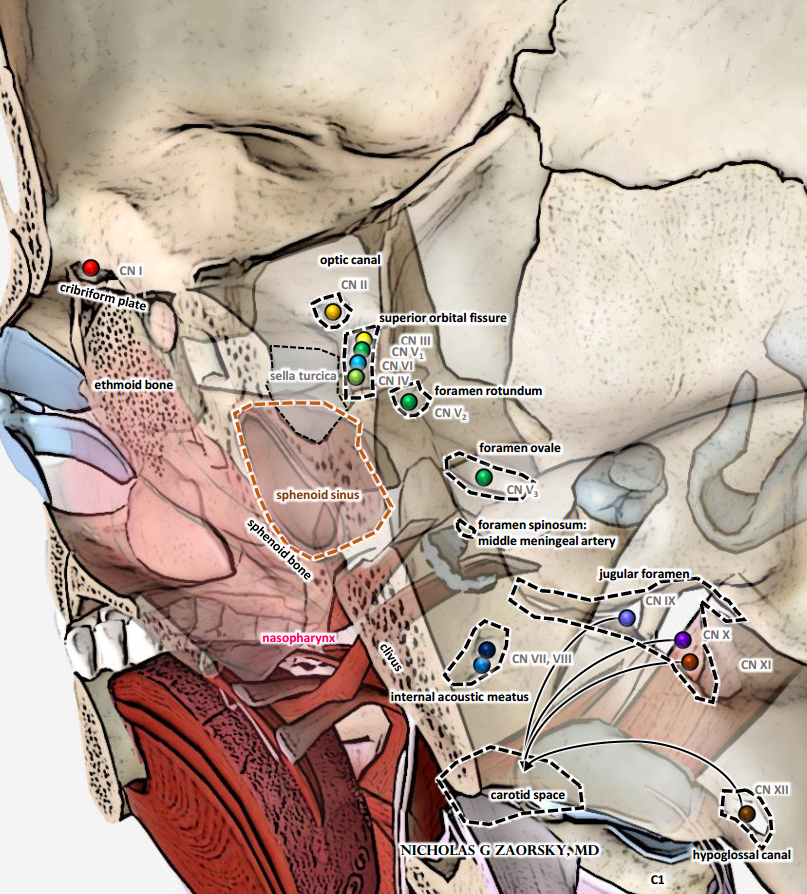
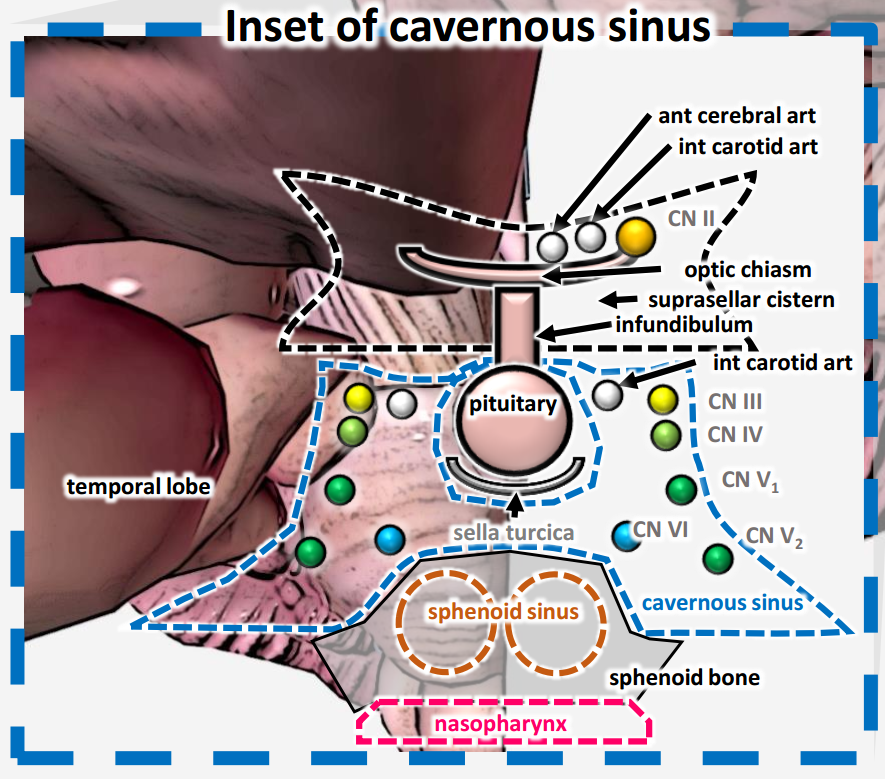
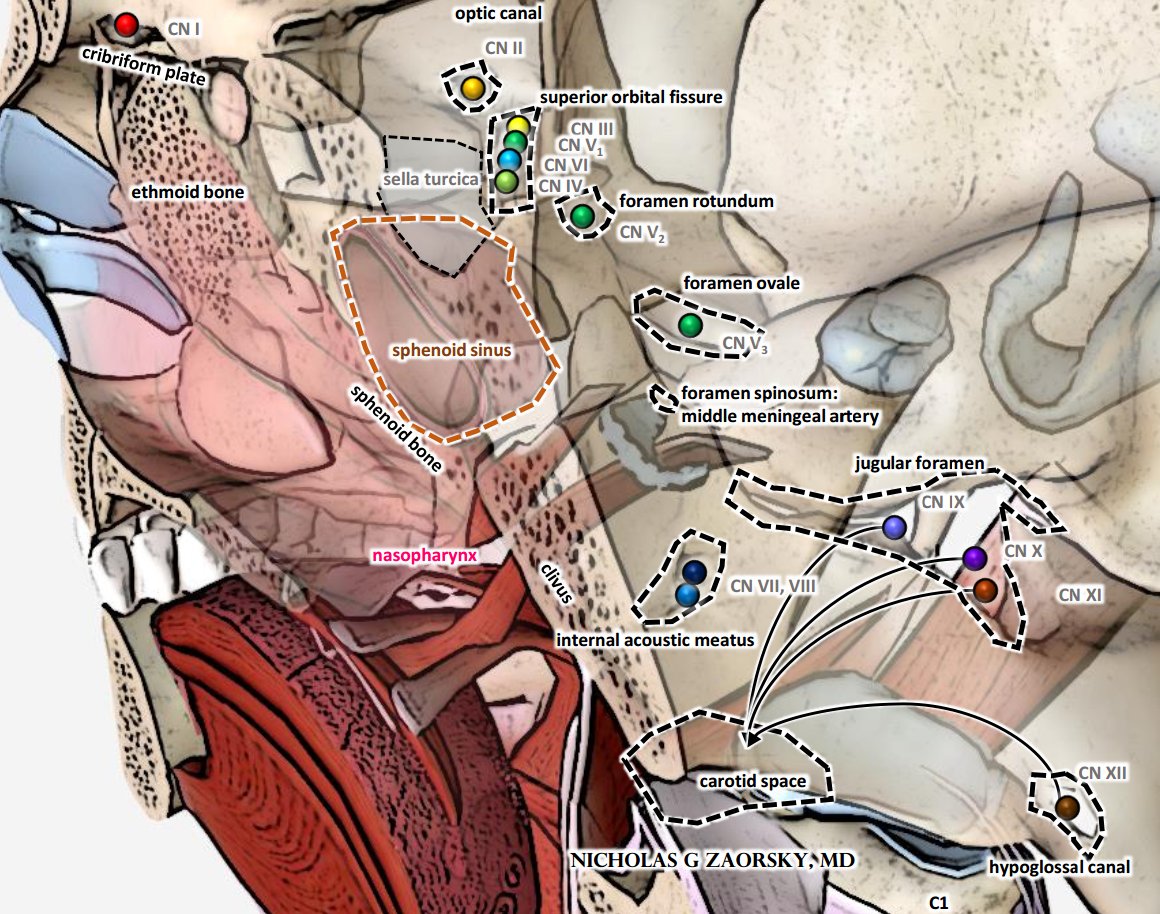
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 Where do cranial nerves exit skull base?
Cavernous sinus has III, IV, V1, V2, VI.
VI is relatively medial, can be affected first from pituitary tumors, or cancers of sphenoid sinus, advanced nasopharynx ca.
#HNCSM
Cavernous sinus has III, IV, V1, V2, VI.
VI is relatively medial, can be affected first from pituitary tumors, or cancers of sphenoid sinus, advanced nasopharynx ca.
#HNCSM
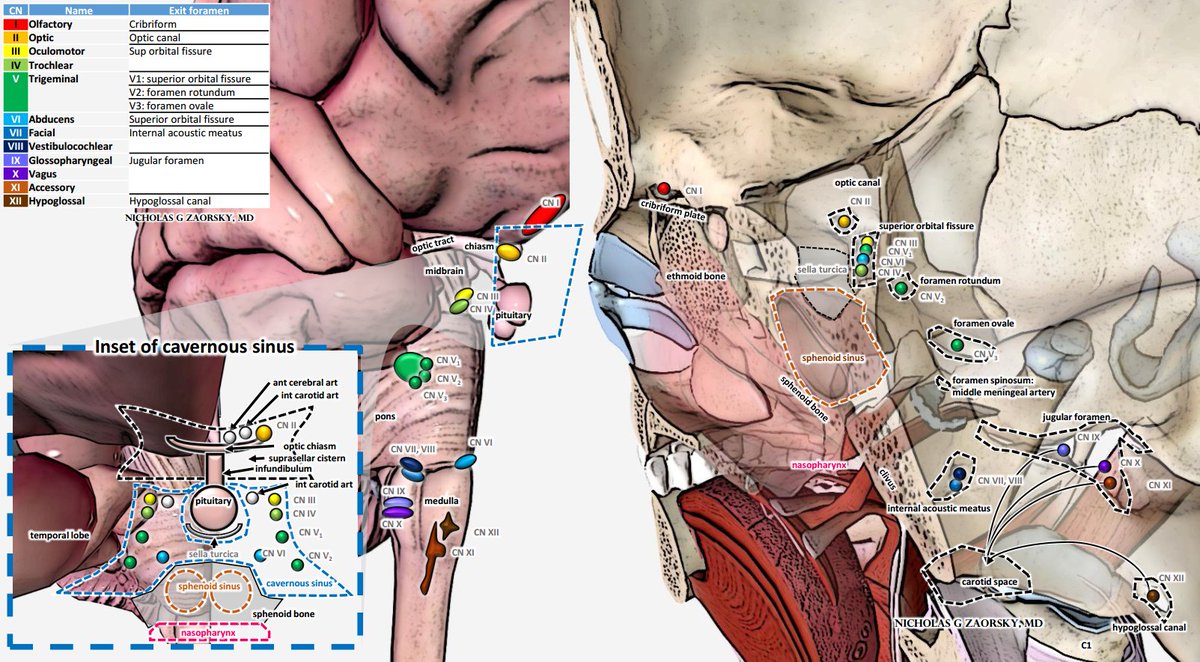
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 Superior orbital fissure has III, V1, VI, IV.
Foramen rotundum has V2.
Foramen ovale has V3.
SRO = Standing Room Only for exit of V1/2/3. Common mnemonic in #medtwitter #MedEd for @TheUSMLE exams.
Foramen rotundum has V2.
Foramen ovale has V3.
SRO = Standing Room Only for exit of V1/2/3. Common mnemonic in #medtwitter #MedEd for @TheUSMLE exams.
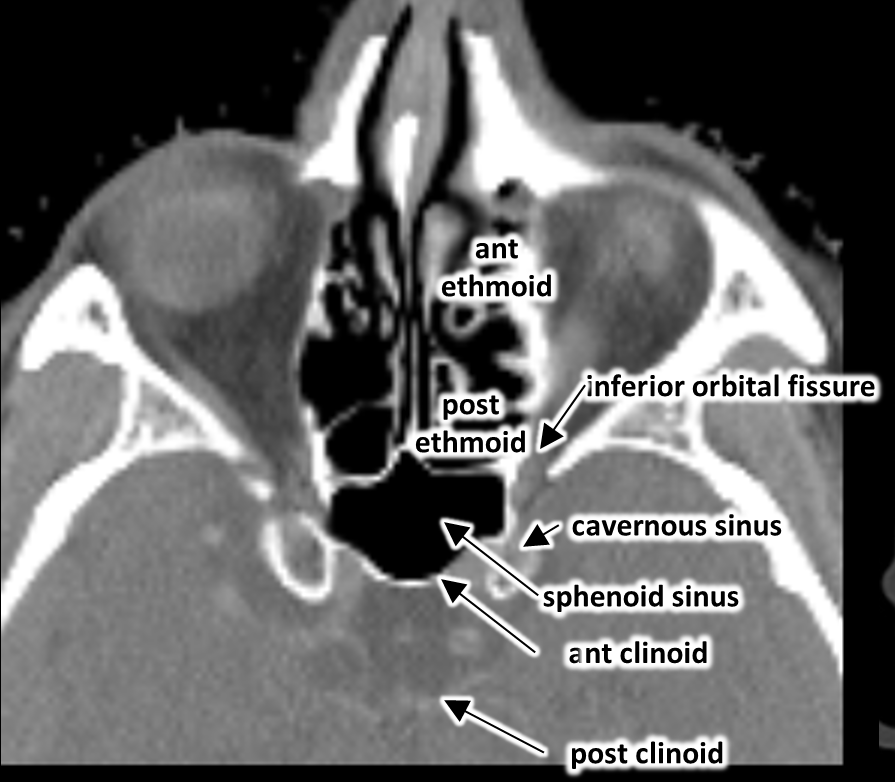
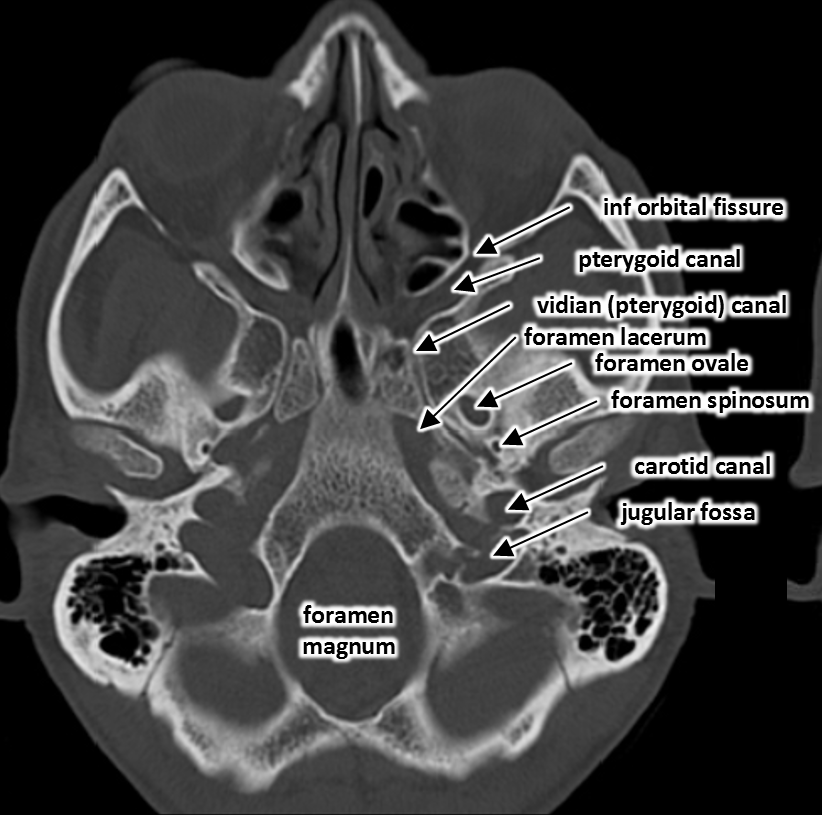
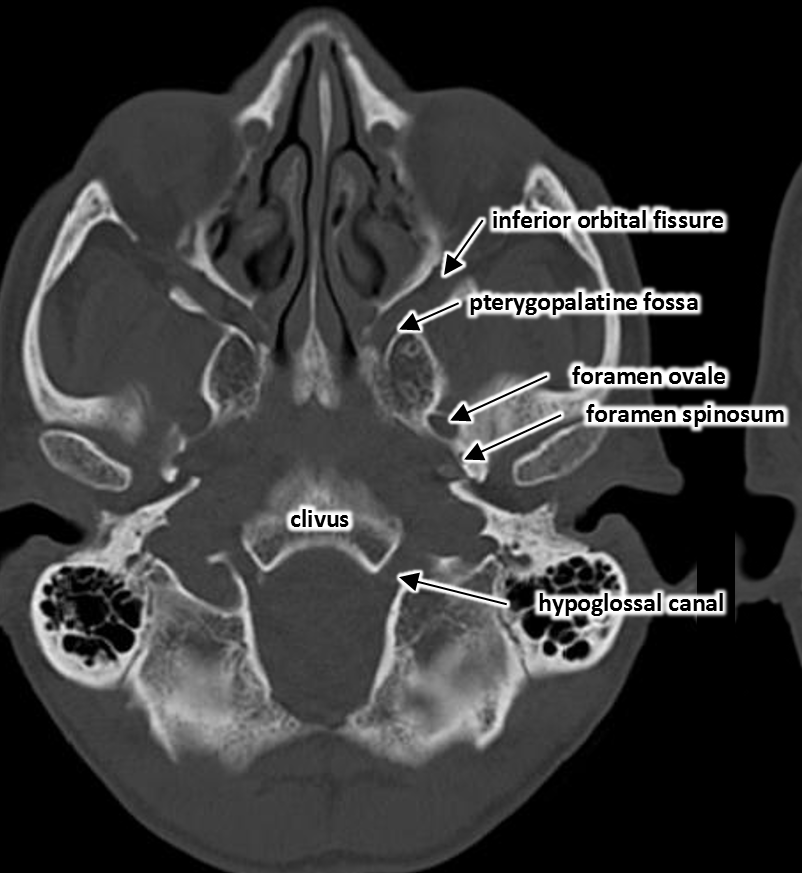
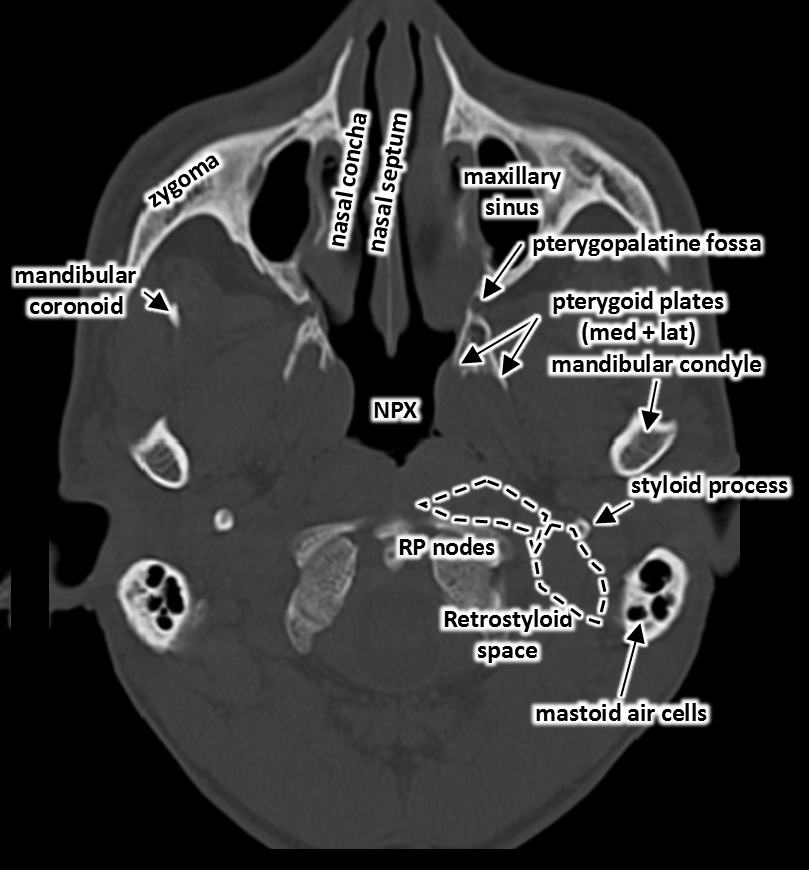
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE Now let's find them on the scans.
Here is an amazing website for more details: headneckbrainspine.com/Neuroanatomy-m…
@TheASNR @RadiologyACR
Here is an amazing website for more details: headneckbrainspine.com/Neuroanatomy-m…
@TheASNR @RadiologyACR
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR Brain anatomy: coronal slice and sagittal see-through image to show the insula, internal capsule, putamen, caudate, hippocampus, amygdala
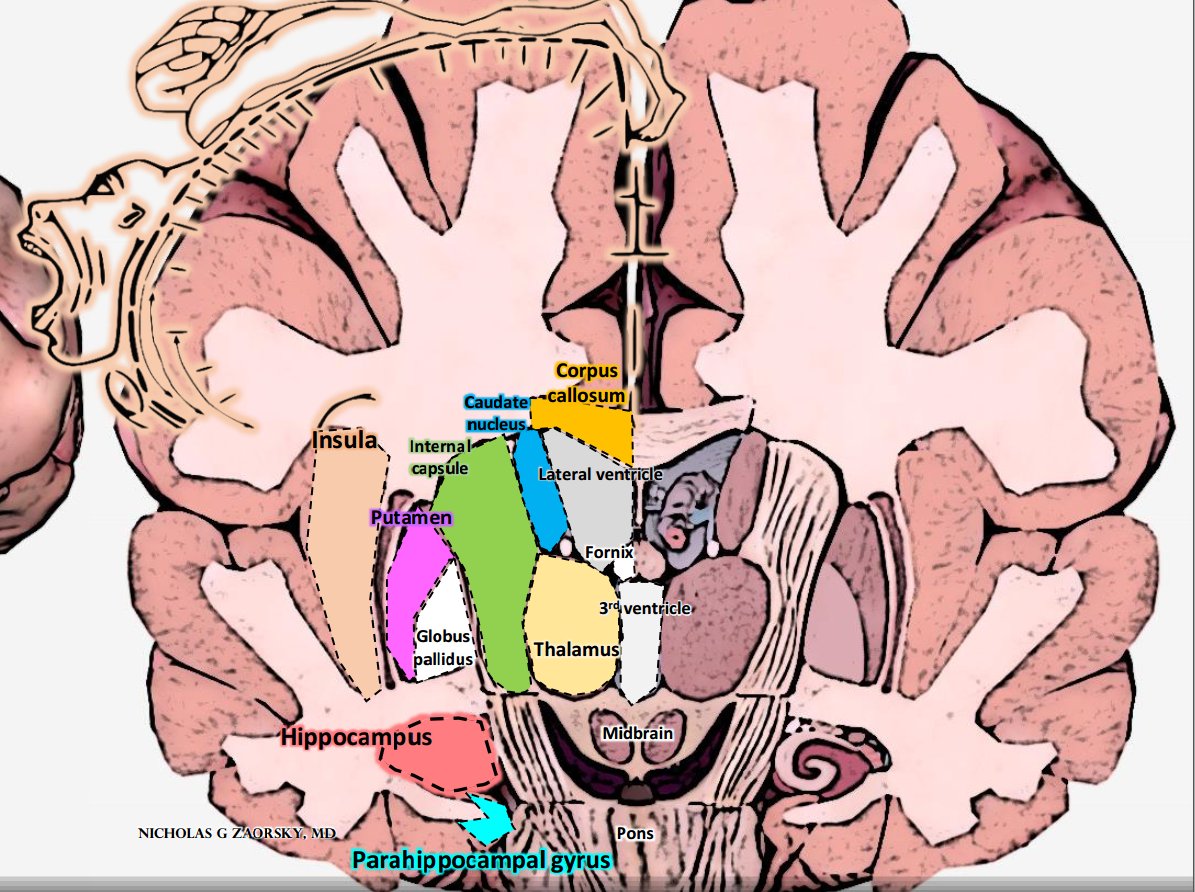
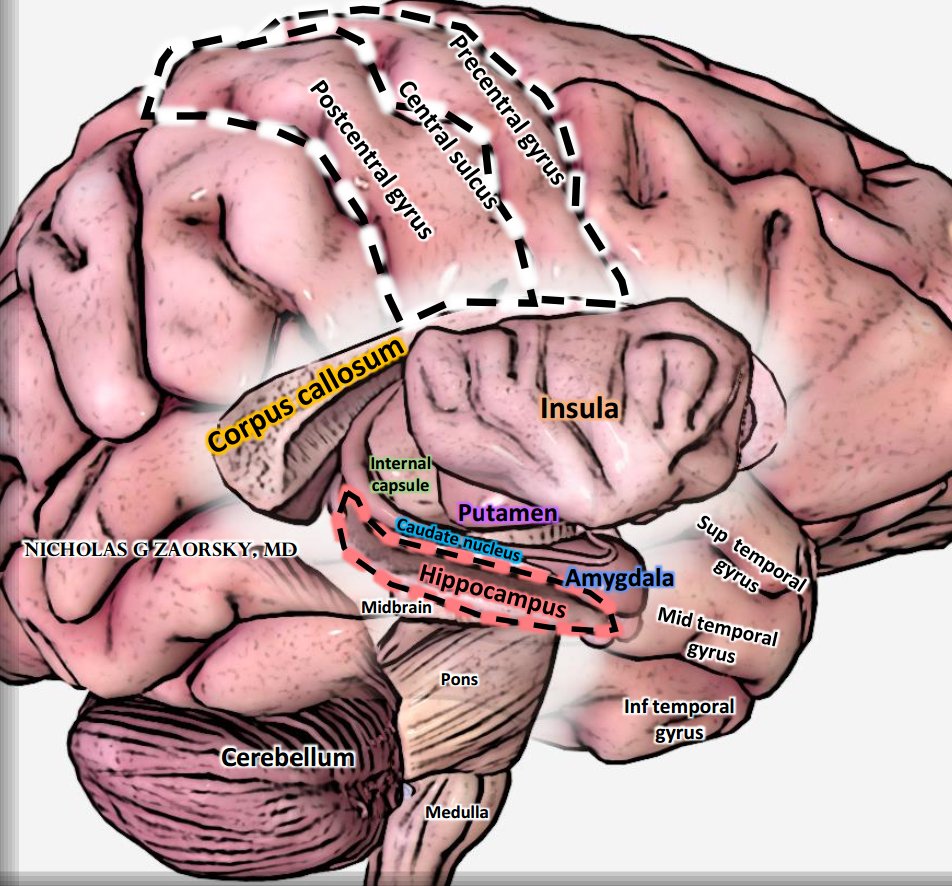
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR In #RadOnc, current radiotherapy studies led by @vinaigondi are preserving hippocampus
ncbi.nlm.nih.gov/pubmed/25349290
#BTSM
Here is the @NRGonc contouring atlas related to the anatomy
rtog.org/CoreLab/Contou…
ncbi.nlm.nih.gov/pubmed/25349290
#BTSM
Here is the @NRGonc contouring atlas related to the anatomy
rtog.org/CoreLab/Contou…
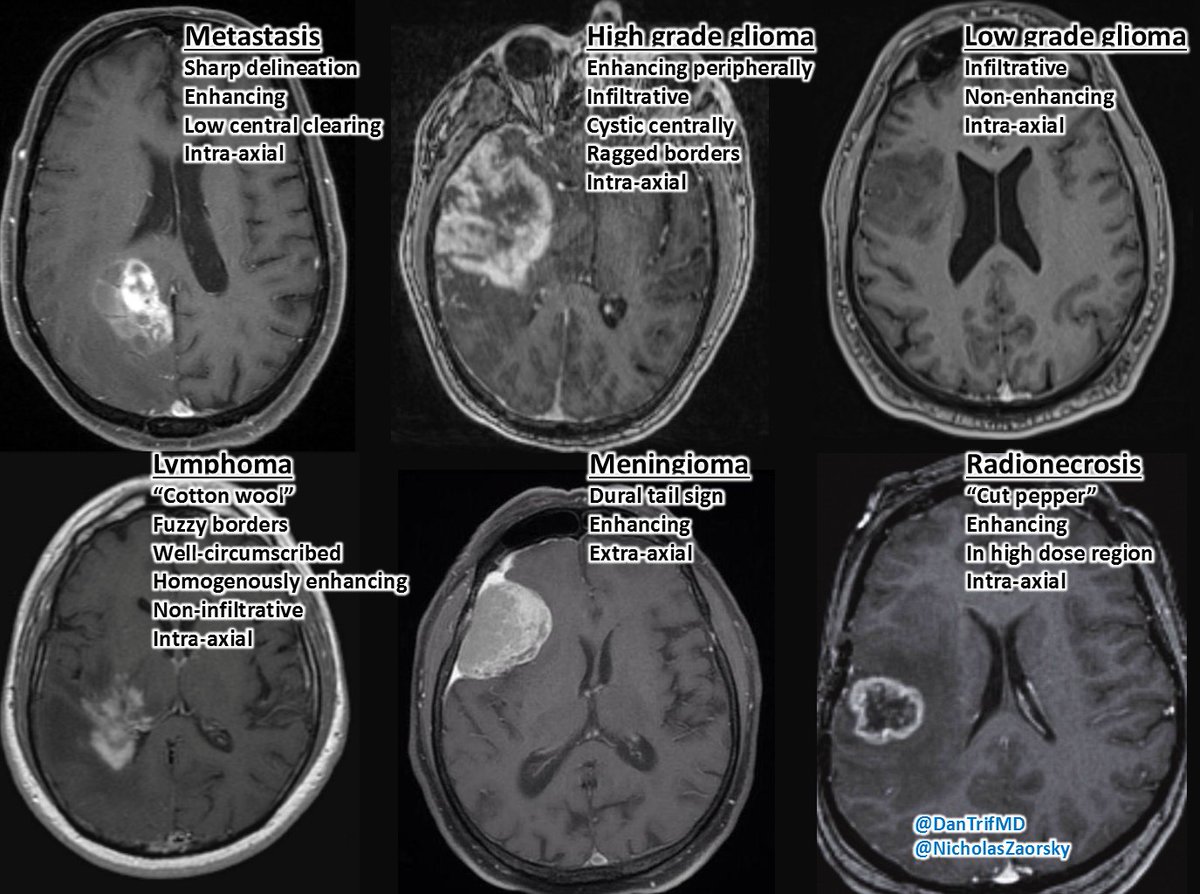
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc Cancer on brain MRI.
Mets are at g/w junction, sharp delineation.
HGG enhances peripherally, infiltrates, is cystic, ragged borders. LGG similar, but usually not enhancing.
Lymphoma is "cotton wool."
Meningioma has dural tail sign, extra-axial.
Radionecrosis is "cut pepper"
Mets are at g/w junction, sharp delineation.
HGG enhances peripherally, infiltrates, is cystic, ragged borders. LGG similar, but usually not enhancing.
Lymphoma is "cotton wool."
Meningioma has dural tail sign, extra-axial.
Radionecrosis is "cut pepper"
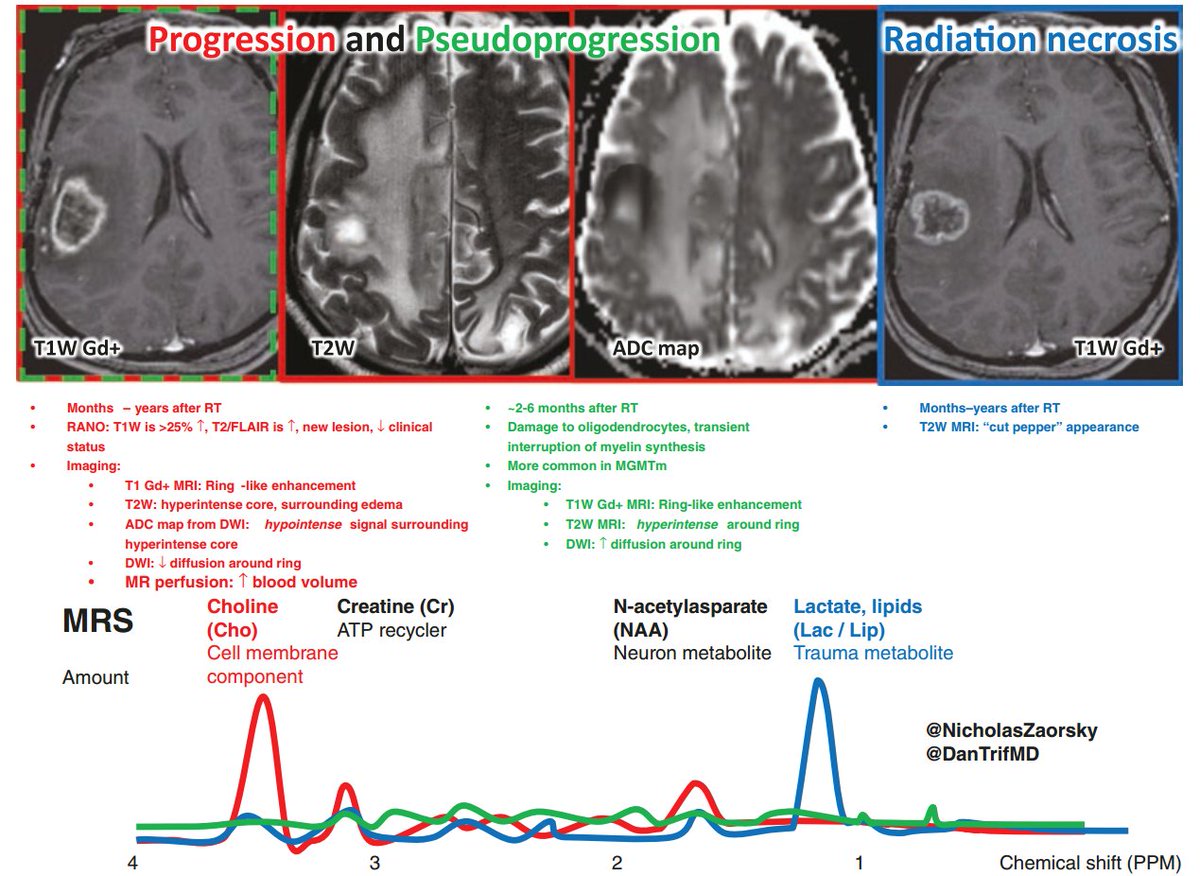
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor MR spectroscopy can help differentiate tumor progression vs pseudoprogression vs radiation necrosis.
Tumors have cells, and CHOLINE is part of cell membrane.
Necrotic tissue has LACTATE.
These are the 2 peaks on MRS.
Tumors have cells, and CHOLINE is part of cell membrane.
Necrotic tissue has LACTATE.
These are the 2 peaks on MRS.
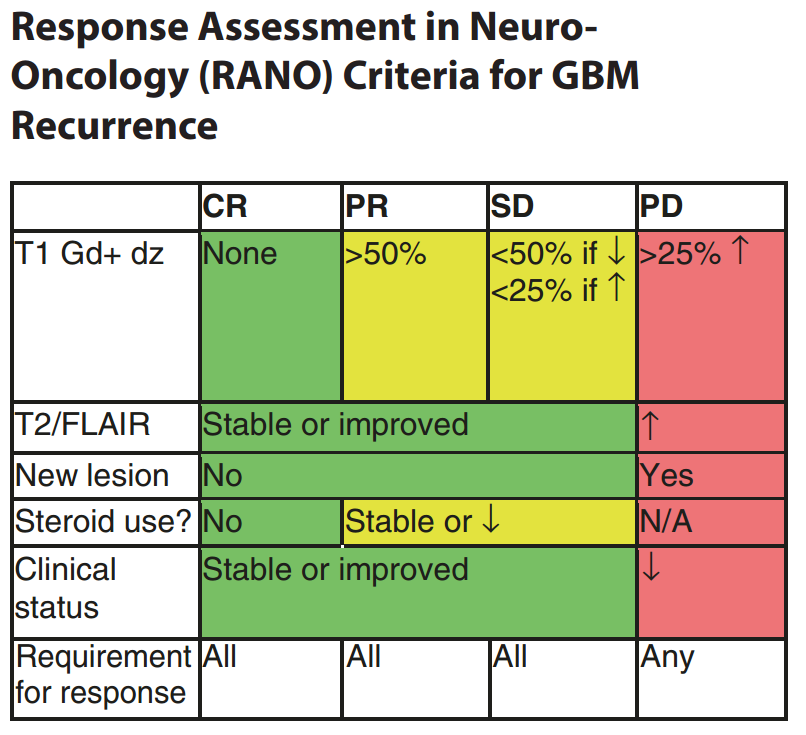
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor RANO criteria for GBM recurrence summarized
radiopaedia.org/articles/rano-…
#BTSM
radiopaedia.org/articles/rano-…
#BTSM
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor Trend in neuro-oncology moves away from whole brain RT and toward stereotactic radiosurgery. The volume irradiated greatly reduced w @lgksociety GammaKnife or @Accuray CyberKnife (vs WBRT).
Also SRS+immunotherapy is promising.
ncbi.nlm.nih.gov/pubmed/30241791
ncbi.nlm.nih.gov/pubmed/30301252
Also SRS+immunotherapy is promising.
ncbi.nlm.nih.gov/pubmed/30241791
ncbi.nlm.nih.gov/pubmed/30301252
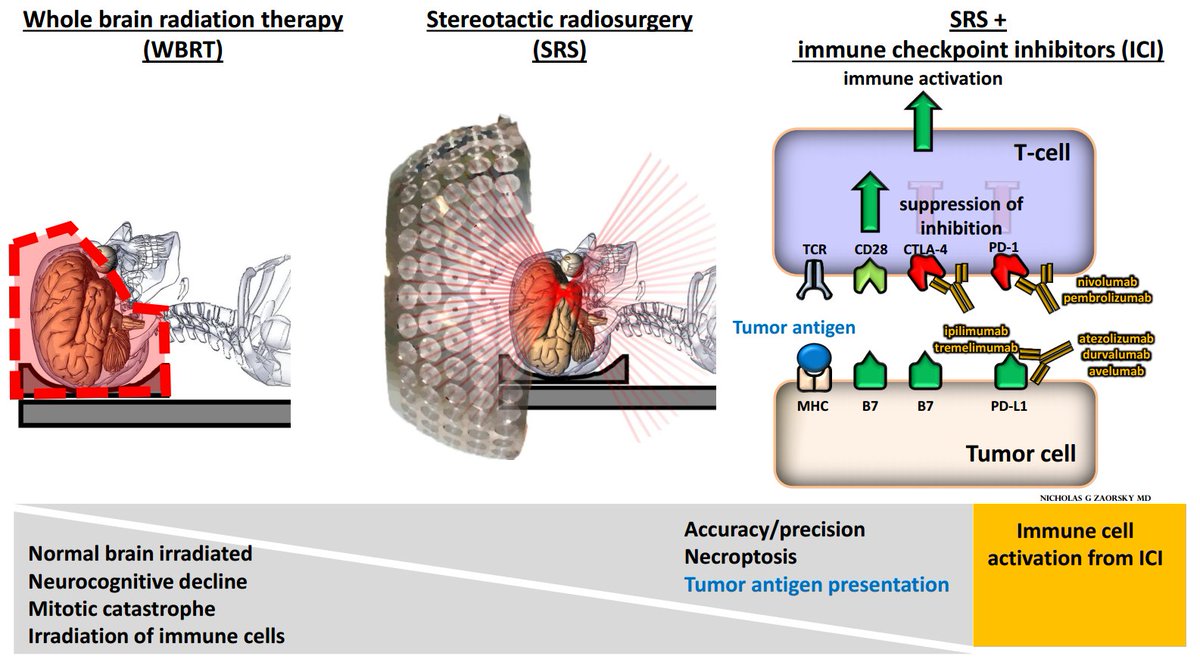
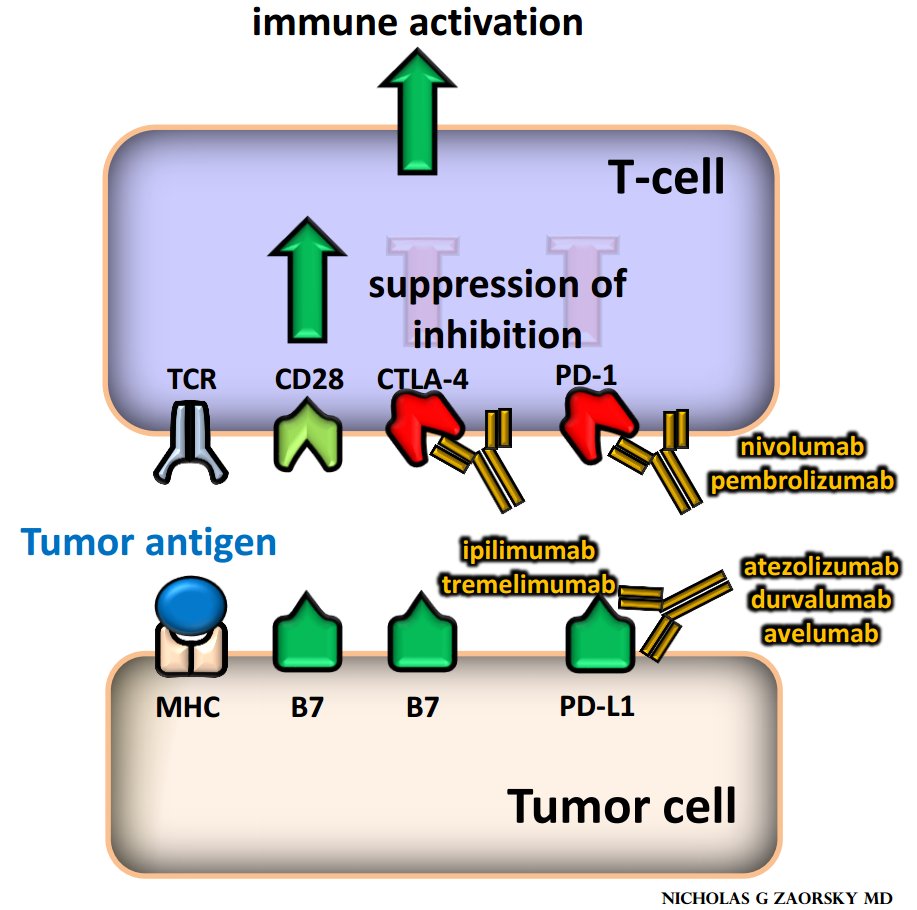
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer For reference, here are most common immuno-oncology drugs used and their purported mechanisms. Drugs are thought to either "release brakes" or "step on gas" of immune system so immune system targets cancer.
Figure I had made for Andrew Sharabi, @UCSDHealth #RadOnc
Figure I had made for Andrew Sharabi, @UCSDHealth #RadOnc
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth Anatomy on lateral view of cranial x-ray

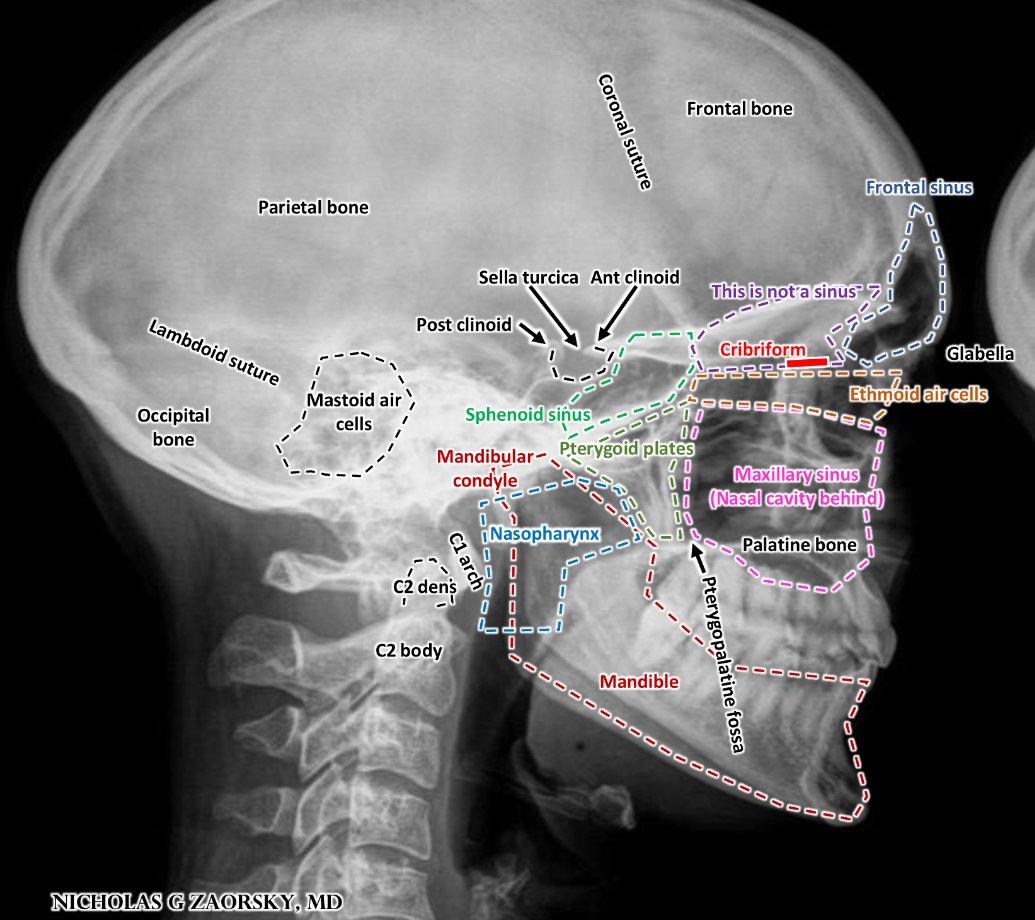
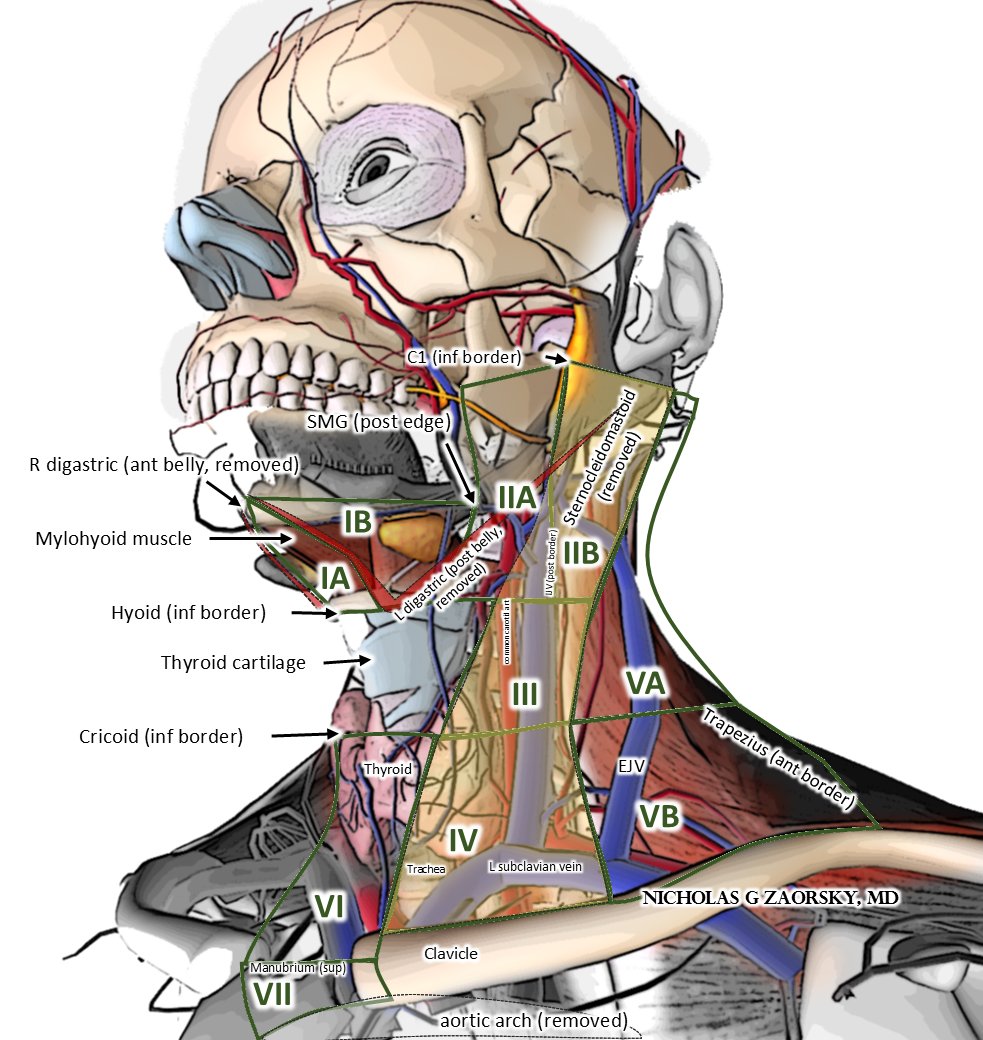
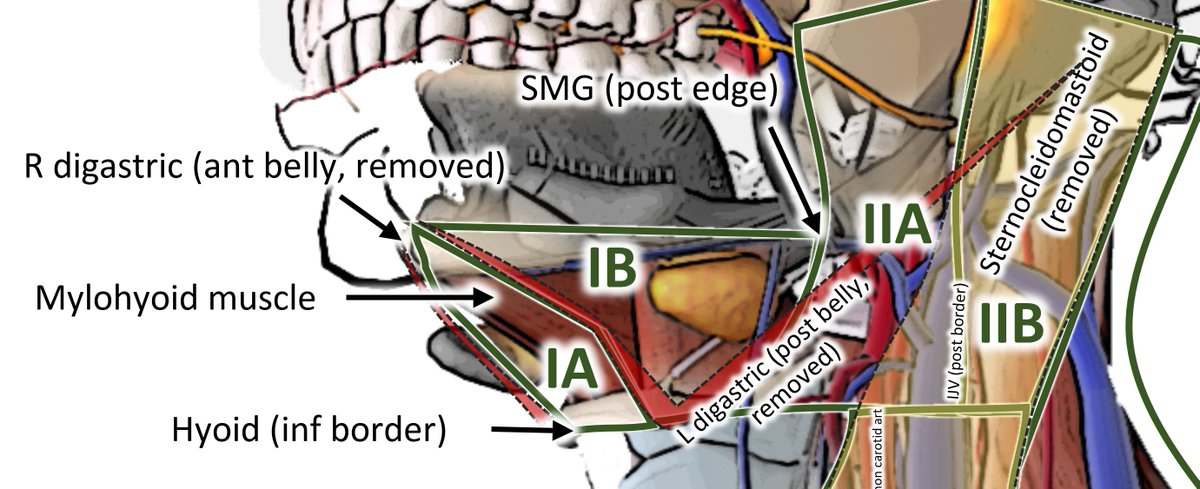
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth Head/neck anatomy w @HenryParkMD #HNCSM
If these lymph nodes involved, consider primary cancer from these:
I: OC, lip, skin
II: "grand central station" (all, tho IIB less from OC, LX, HPX)
III: NPX, OC, OPX, LX, HPX
IV: NPX, OPX, LX, HPX > OC
V: NPX, skin
VI: thyroid, LX, HPX
If these lymph nodes involved, consider primary cancer from these:
I: OC, lip, skin
II: "grand central station" (all, tho IIB less from OC, LX, HPX)
III: NPX, OC, OPX, LX, HPX
IV: NPX, OPX, LX, HPX > OC
V: NPX, skin
VI: thyroid, LX, HPX
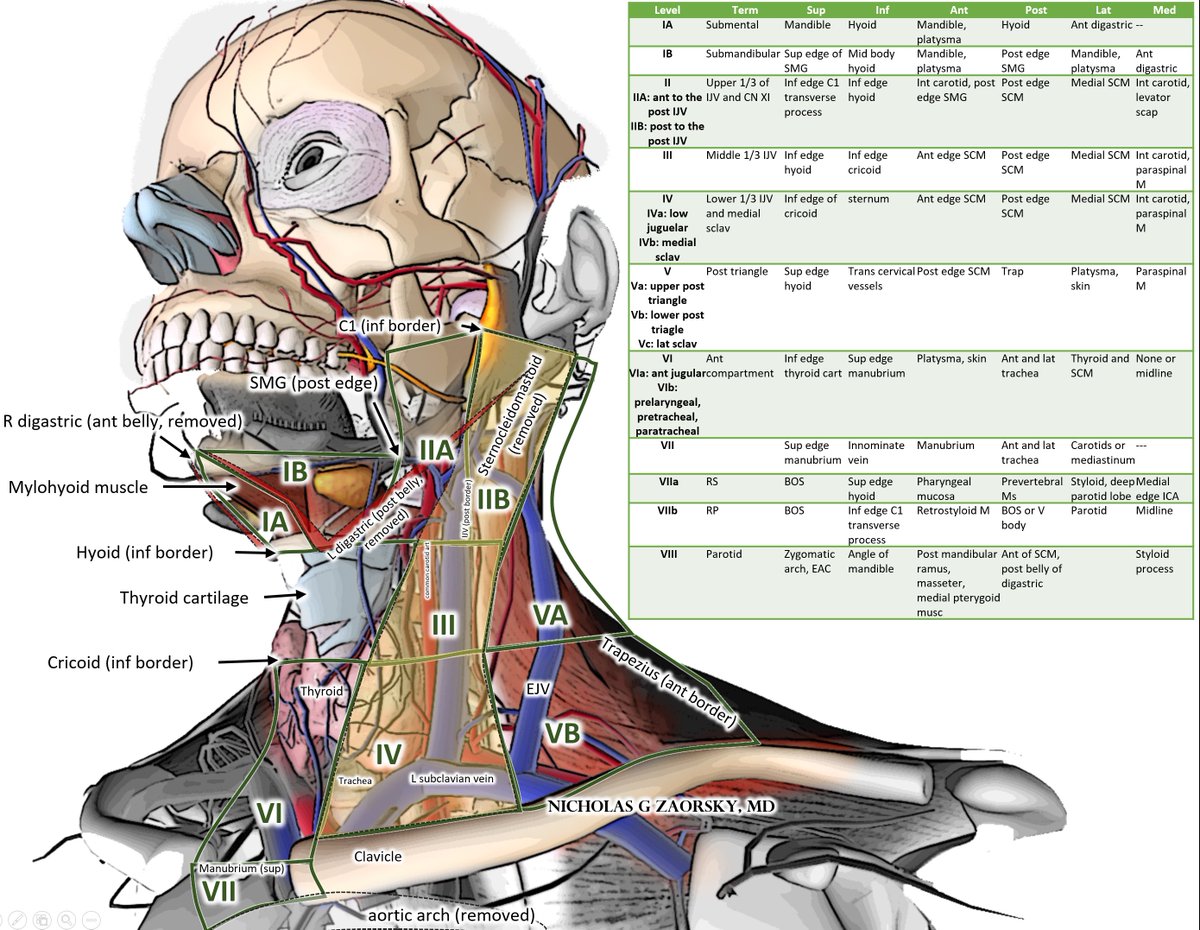
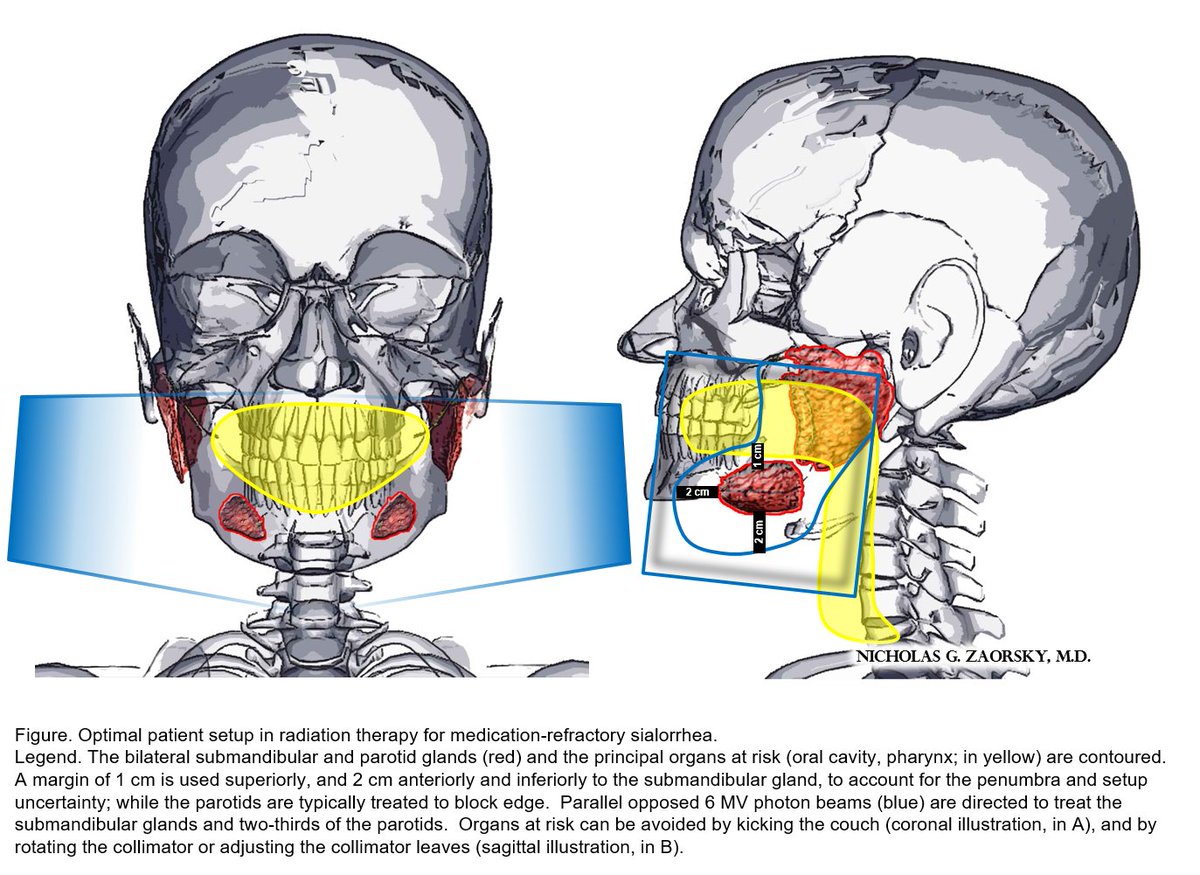
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD Interestingly, the SMG (yellow potato in pic) rarely has metastasis bc it is encapsulated. If you see cancer here, consider primary SMG cancer.
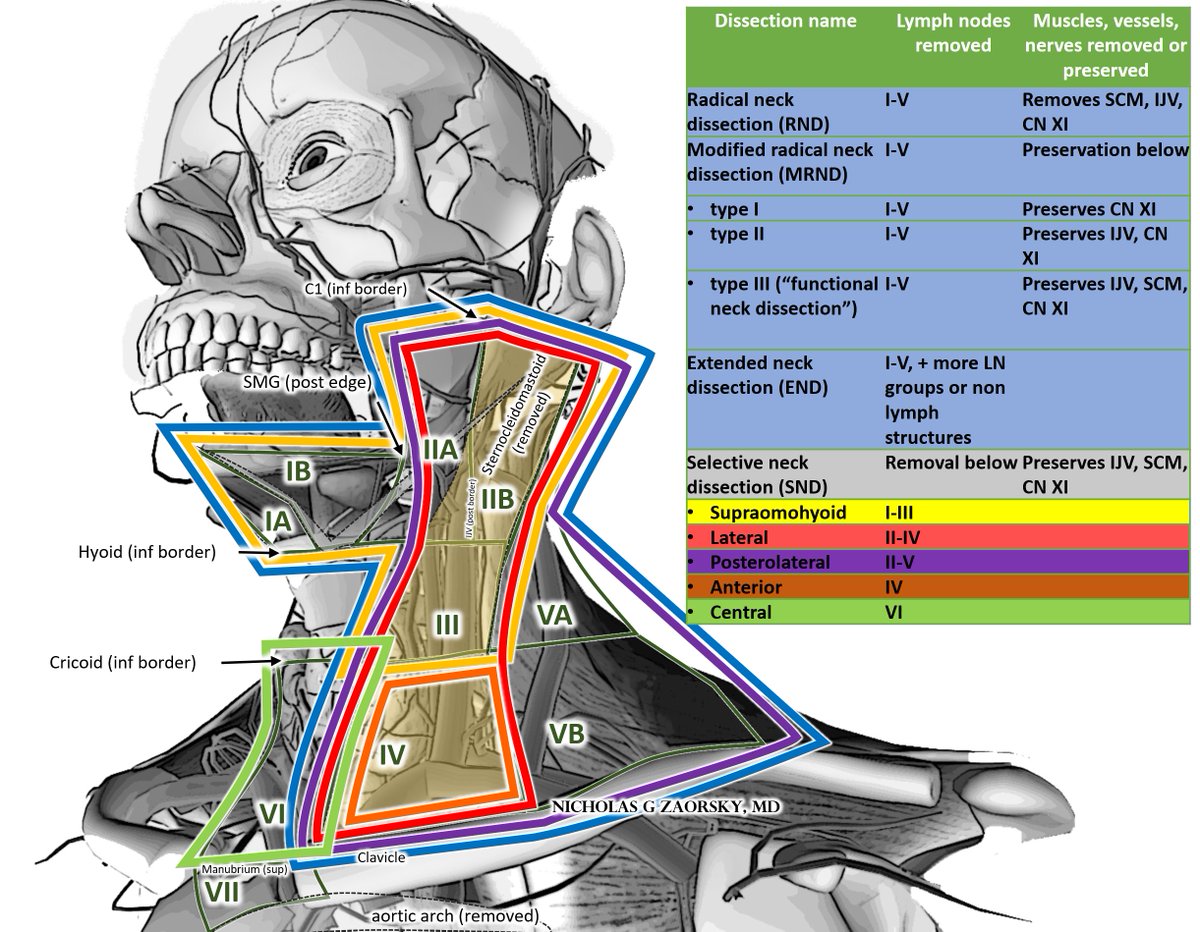
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD There are different types of neck dissections.
Modified radical neck dissections and selective neck dissections can preserve normal anatomy and function.
Modified radical neck dissections and selective neck dissections can preserve normal anatomy and function.
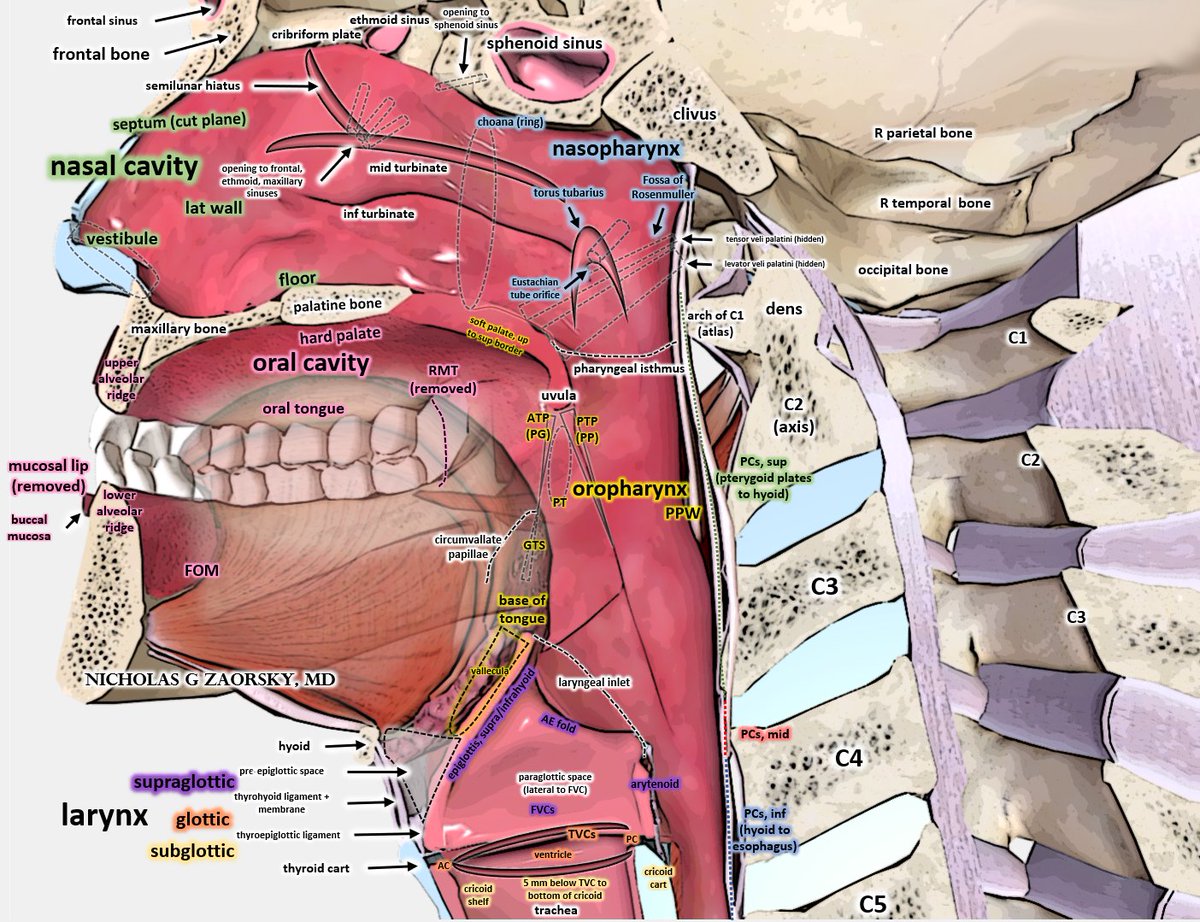
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD Primary head and neck cancers originate from several sites:
nasal cavity (NC), nasopharynx (NPX), oral cavity (OC), oropharynx (OPX), larynx (LX).
In developed countries today, there is rise in HPV+ cancers of the OPX, typically from base of tongue > tonsil.
#HNCSM
nasal cavity (NC), nasopharynx (NPX), oral cavity (OC), oropharynx (OPX), larynx (LX).
In developed countries today, there is rise in HPV+ cancers of the OPX, typically from base of tongue > tonsil.
#HNCSM
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD In fact, most HPV+ OPX cancers were "Stage IV" in @AJCCancer 6-7th ed manual. In contrast, in 8th ed (2017+), many HPV+ cancers are Stage I-II, treatment paradigm is for de-intensification.
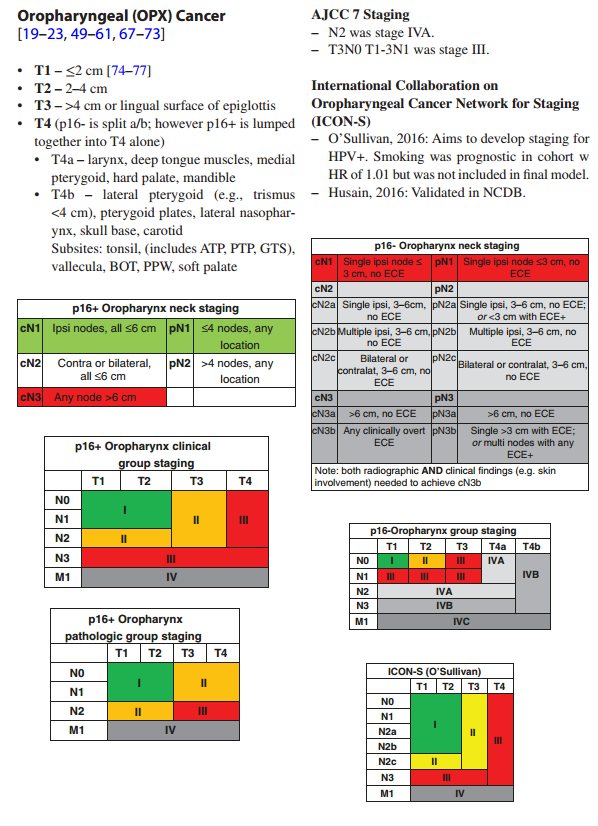
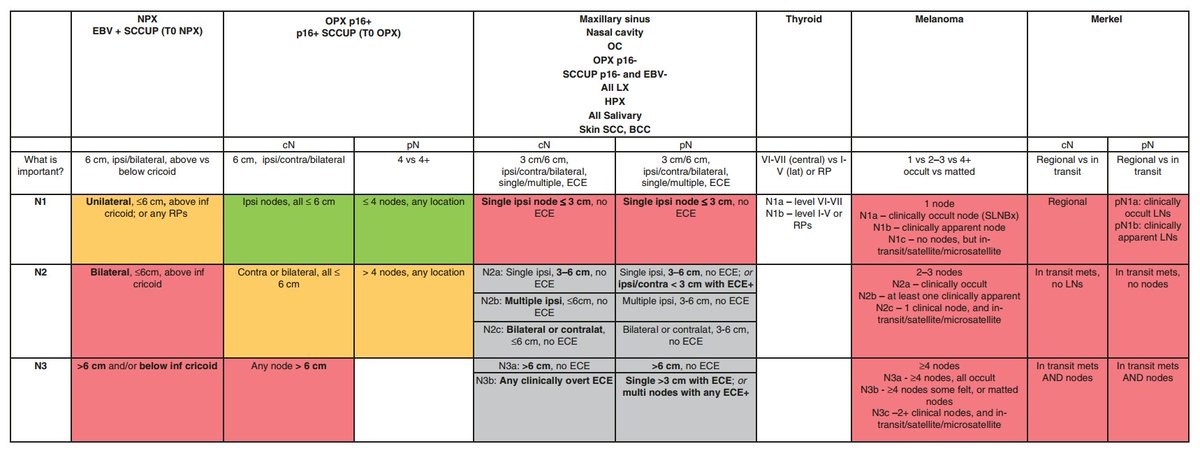
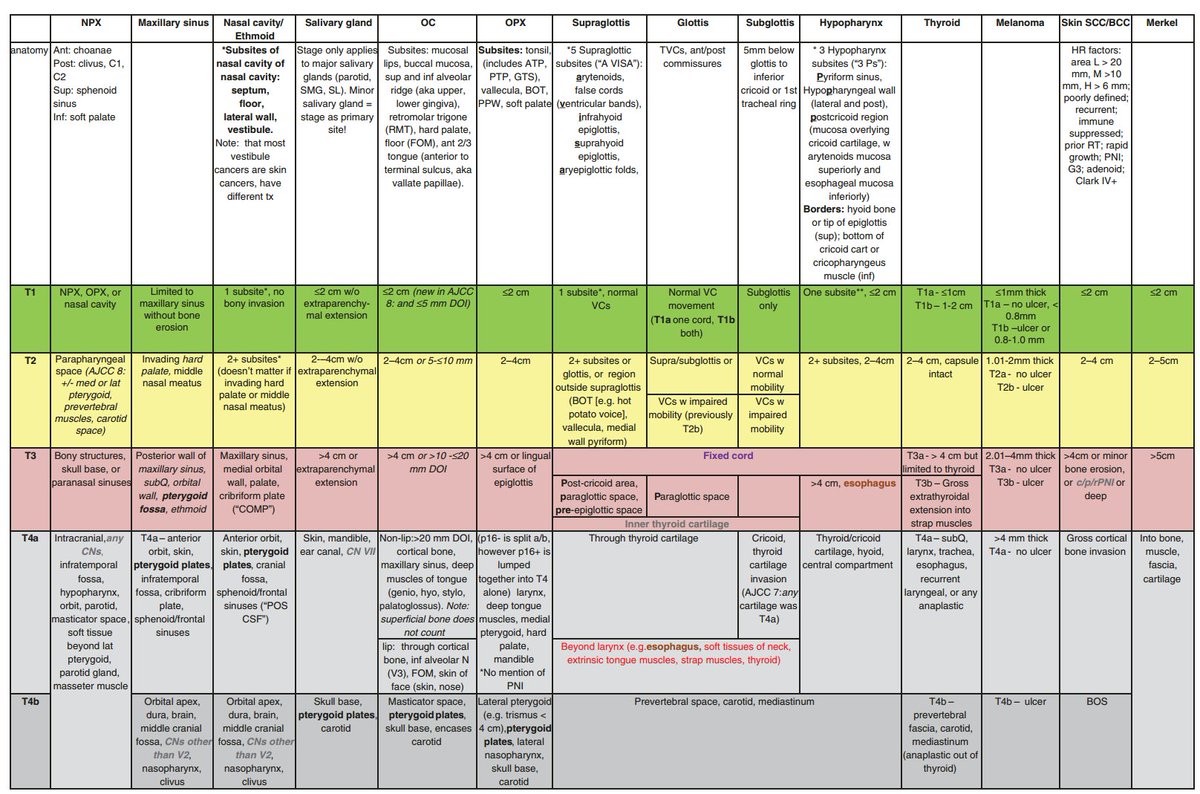
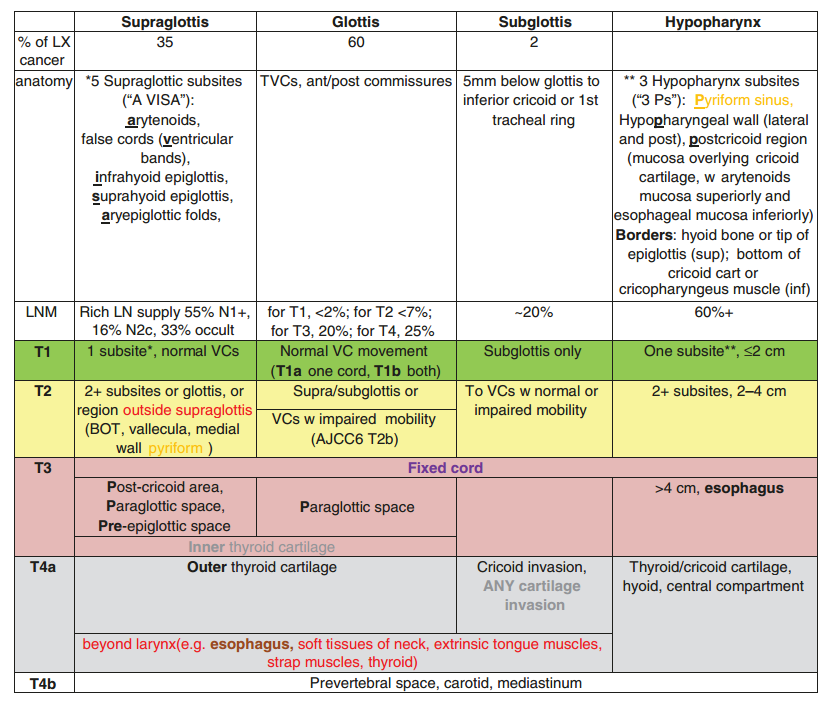
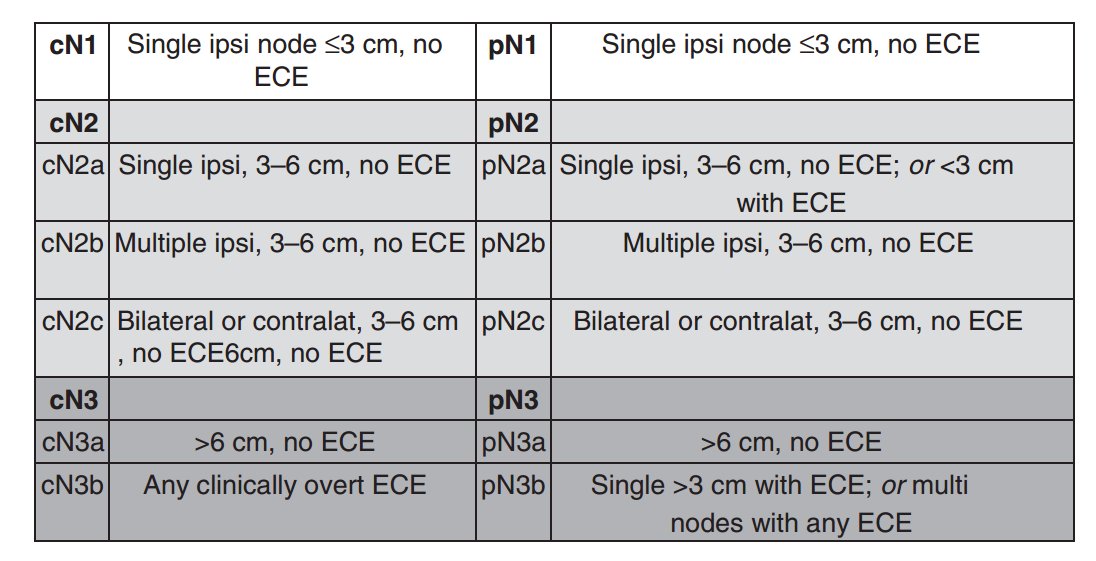
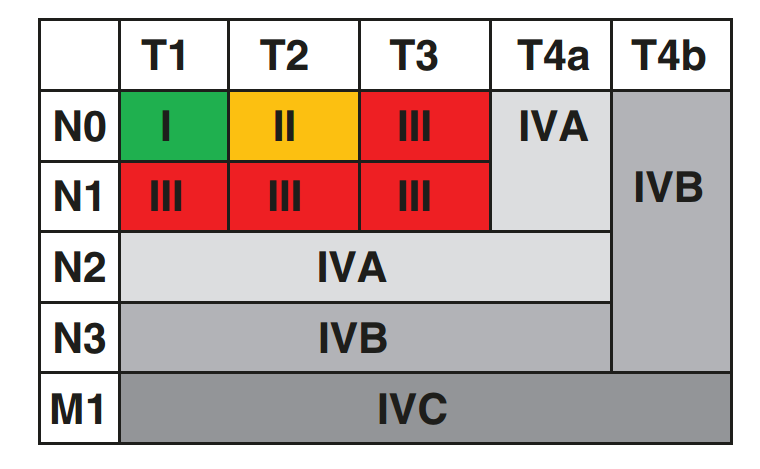
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer Staging for most other HN cancers still complex, so we distilled @AJCCancer staging into 2 pages.
#HNCSM
#HNCSM
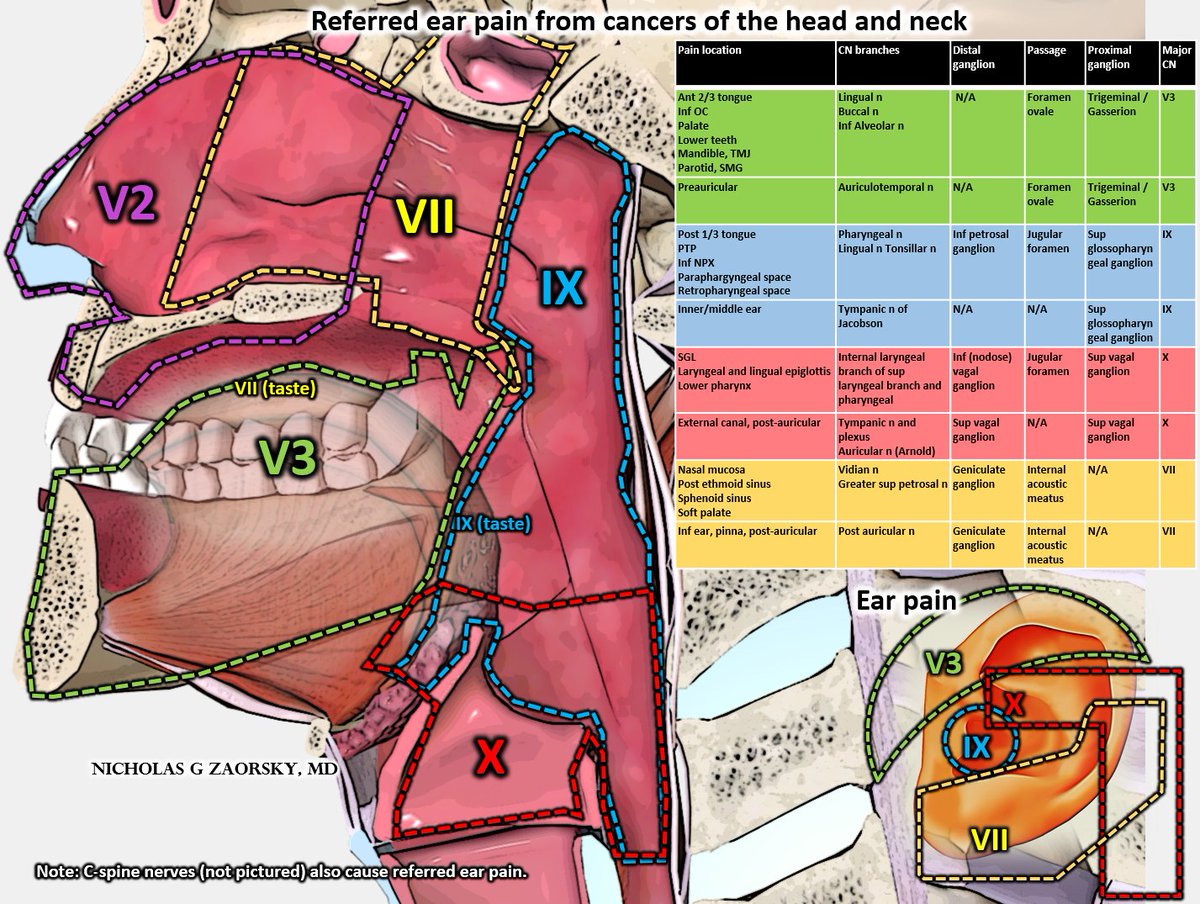
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer Certain HN cancers may cause referred pain, e.g. ear pain.
For pain in:
V3: think OC, palate, lower teeth, mandible
IX: PTP, NPX, RS space
X: LX, lingual epiglottis, external canal (post-auricular)
VII: NC, ethmoid, sphenoid
For pain in:
V3: think OC, palate, lower teeth, mandible
IX: PTP, NPX, RS space
X: LX, lingual epiglottis, external canal (post-auricular)
VII: NC, ethmoid, sphenoid
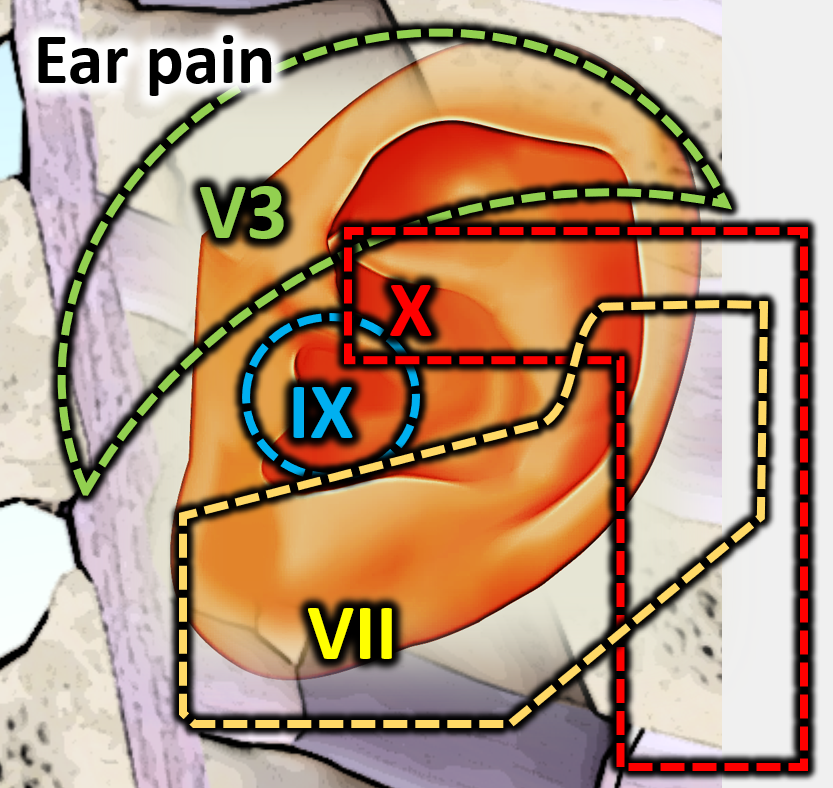
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer Ear pain can actually be caused by any of these 4 nerves, and c-spine pain:
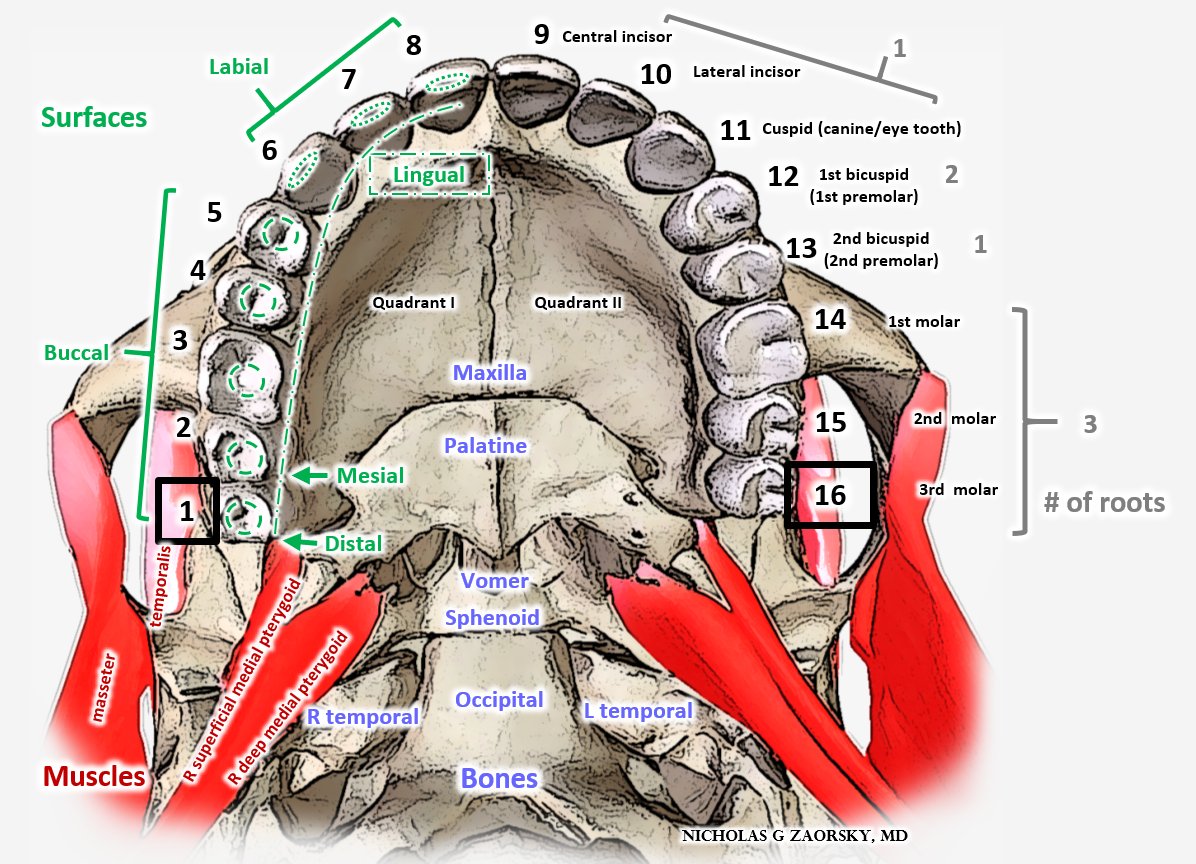
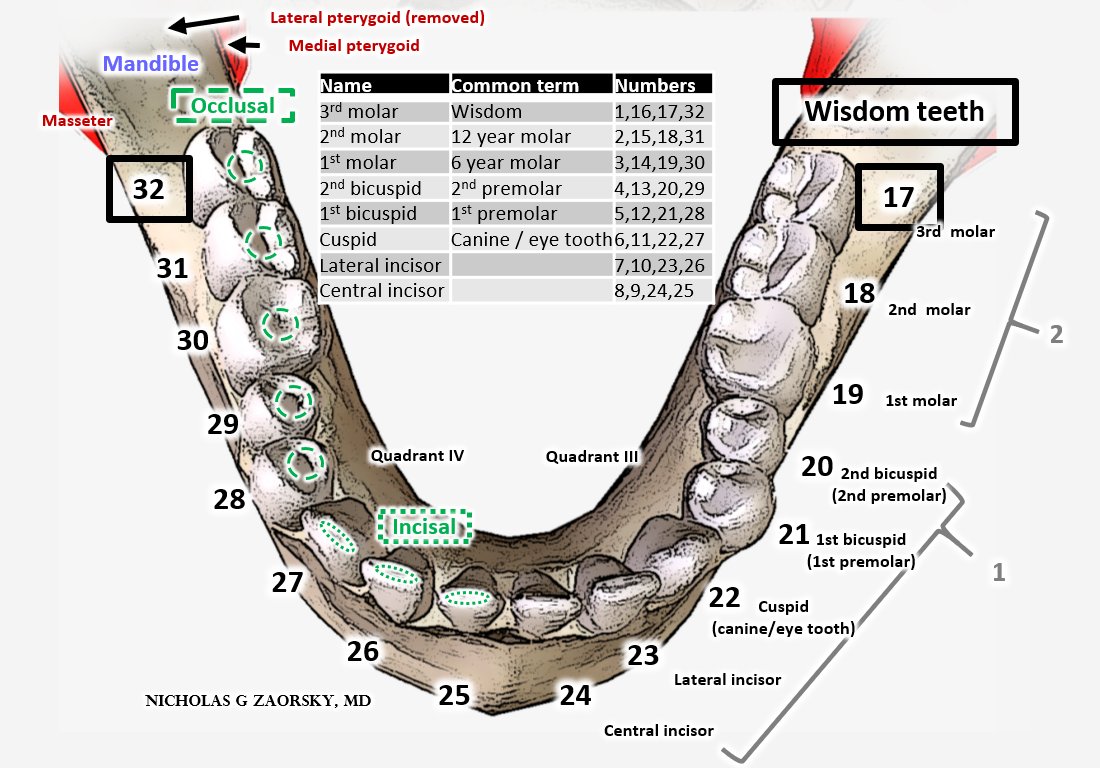
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer Counting teeth made simple. Top right back tooth is 1. Arcing tongue to the left goes to 16. Then go down one, that's 17. Arcing tongue to right goes to 32. 1/16/17/32 are wisdom teeth.
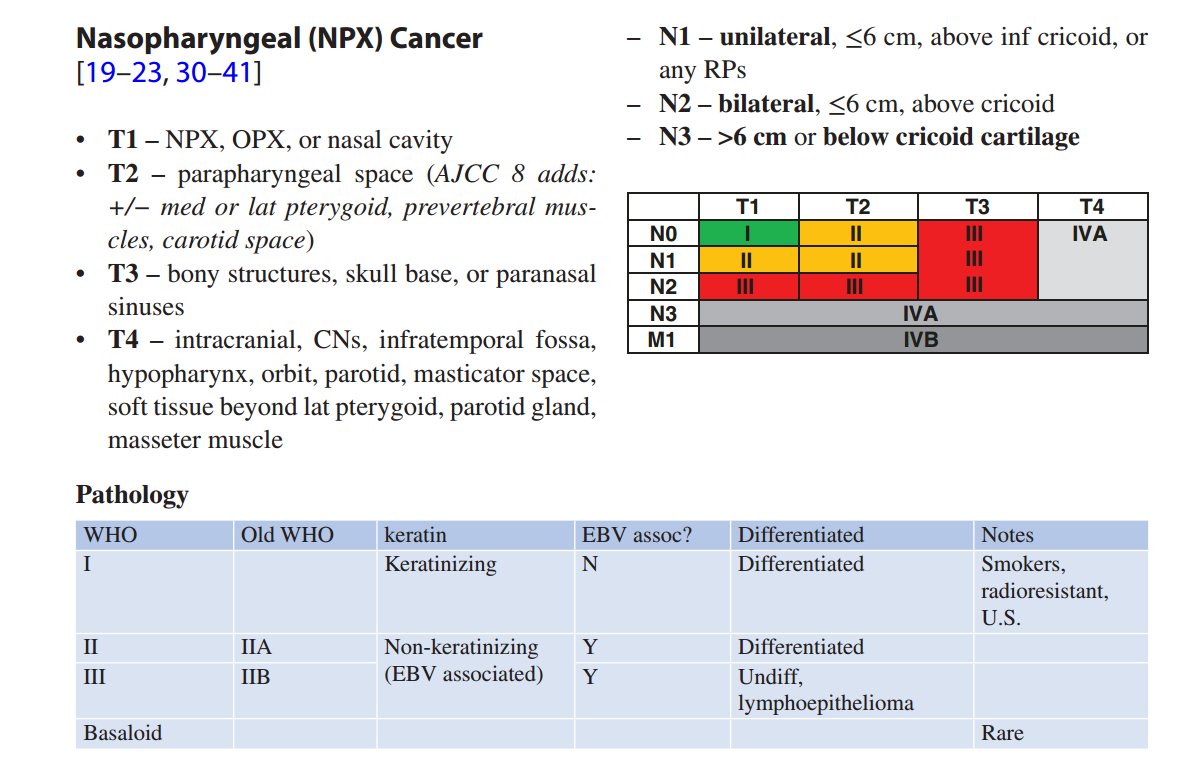
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn Nasopharynx cancer can be staged based on physical exam.
Can't open mouth / say "LAAA" = involvement of the "LAAAteral" pterygoid = at least T2.
Info from @TheUSMLE Step 1 exam returns.
#HNCSM
Can't open mouth / say "LAAA" = involvement of the "LAAAteral" pterygoid = at least T2.
Info from @TheUSMLE Step 1 exam returns.
#HNCSM
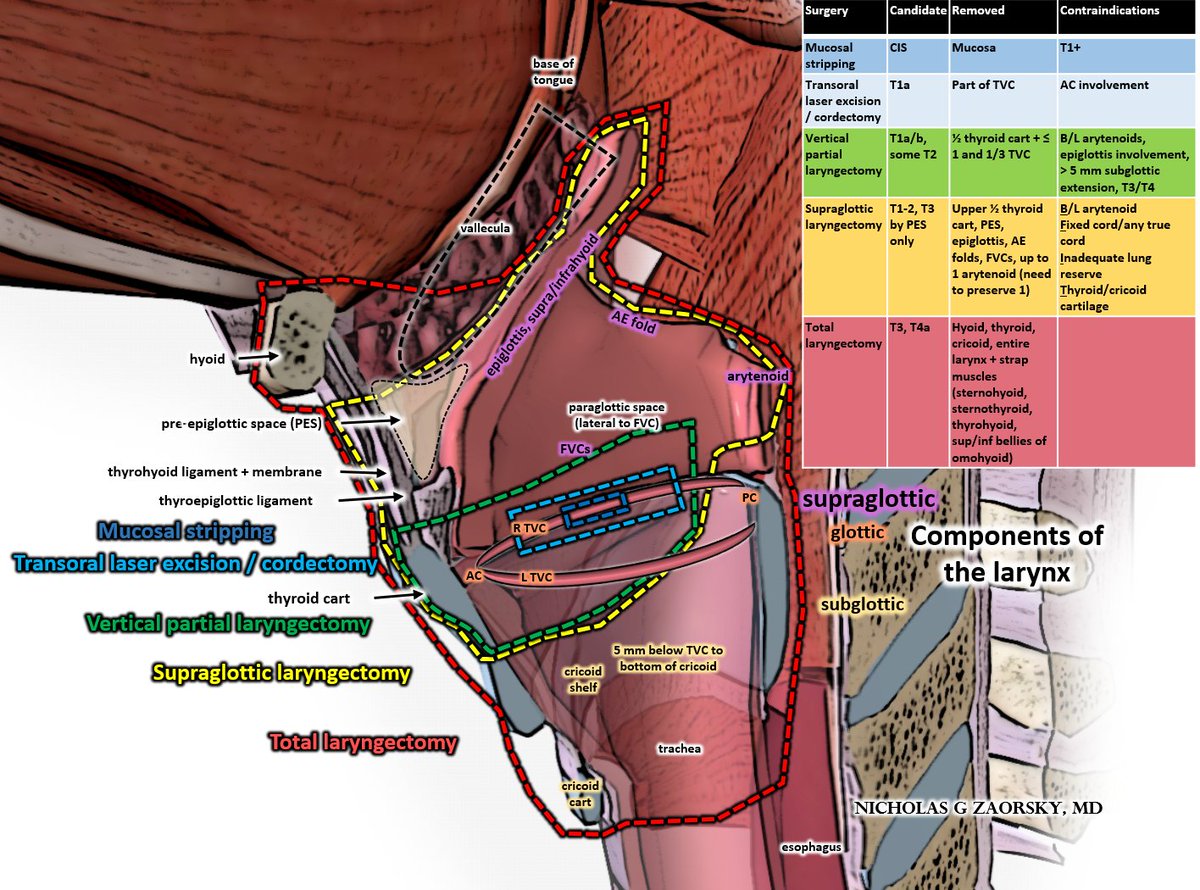
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn For larynx cancer, treatment options depend on involvement of larynx subsites and stage.
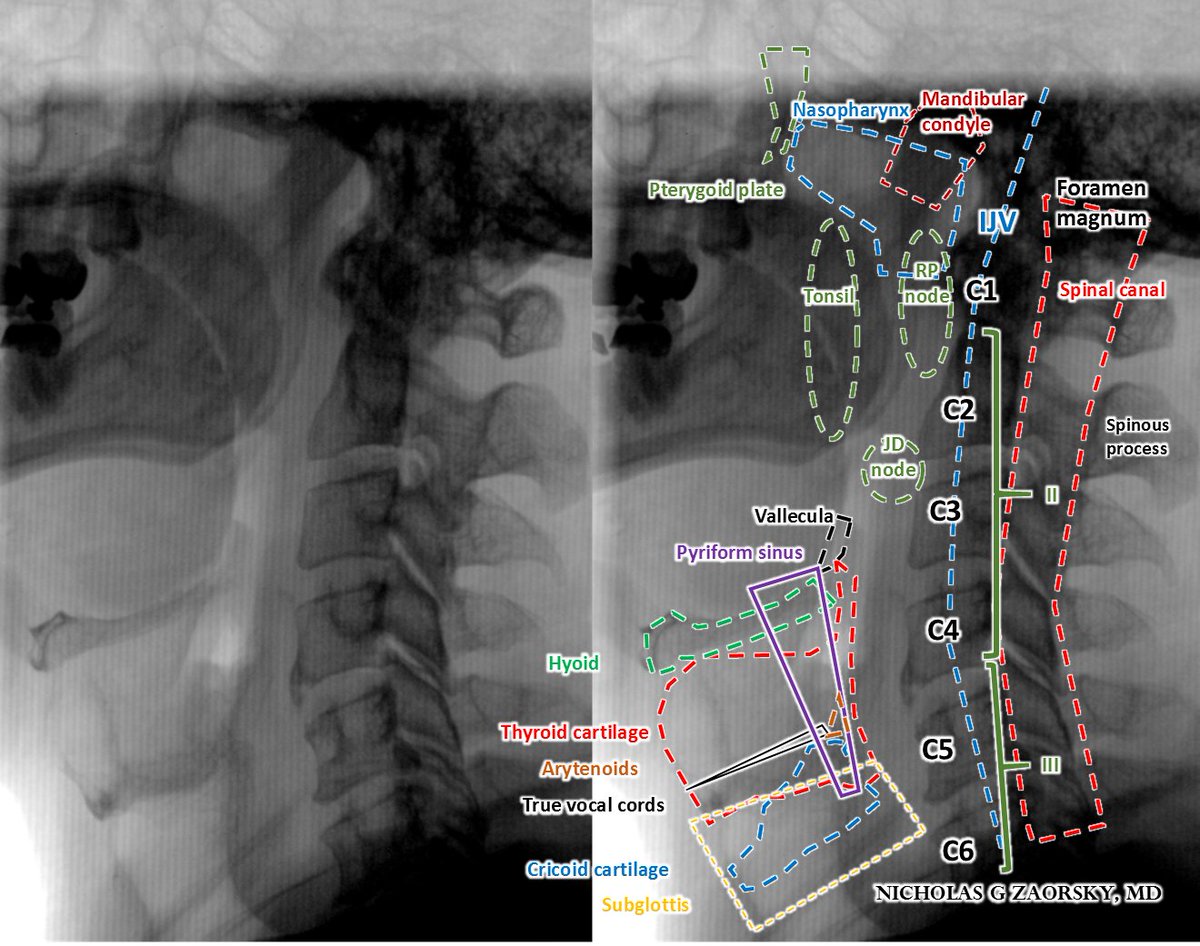
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn Head and neck anatomy on a lateral x-ray
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn Radiation therapy can also be used for benign conditions, like sialorrhea, which is commonly seen in those with ALS, Parkinson dz.
For most head/neck cancers, we avoid salivary glands; here, we treat bilat SMGs and 2/3 parotids.
ncbi.nlm.nih.gov/pubmed/26152655
#ALS #Parkinsons
For most head/neck cancers, we avoid salivary glands; here, we treat bilat SMGs and 2/3 parotids.
ncbi.nlm.nih.gov/pubmed/26152655
#ALS #Parkinsons
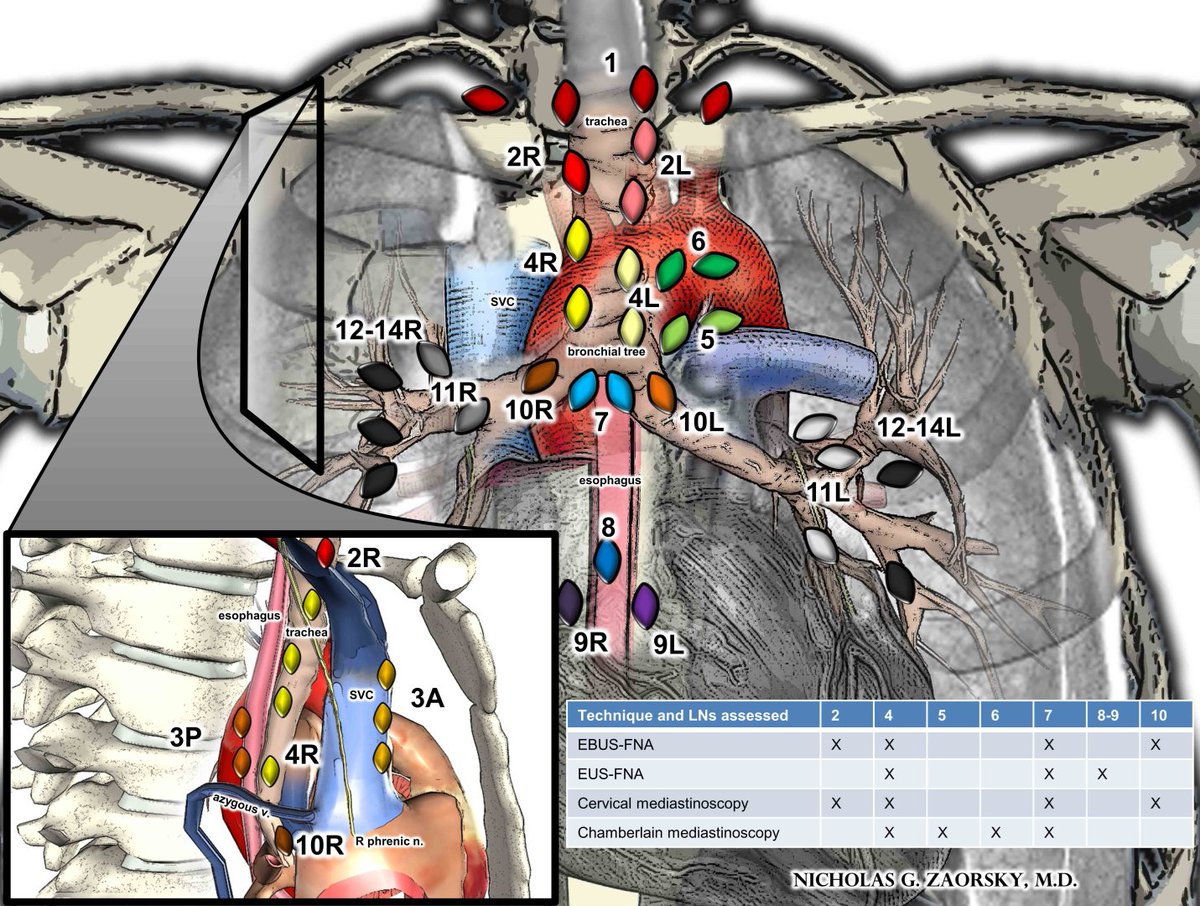
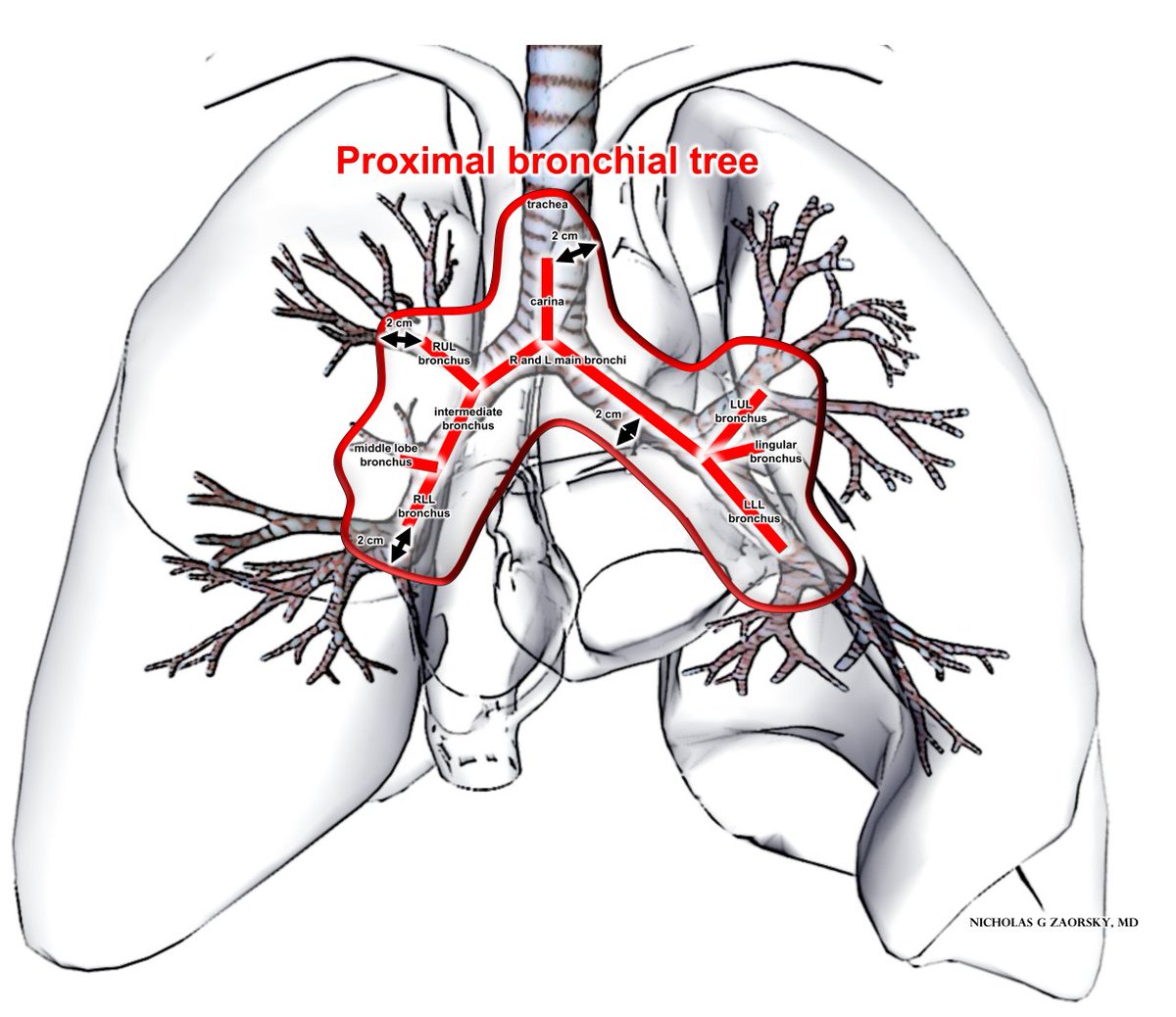
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn LN stations in lungs: single digit numbers (N2) typically near trachea and great vessels, double digit (N1) near main stem bronchi and projections.
N2 disease is Stage III.
EBUS, EUS popular assessment tools but can't access stations 5/6.
#LCSM
N2 disease is Stage III.
EBUS, EUS popular assessment tools but can't access stations 5/6.
#LCSM
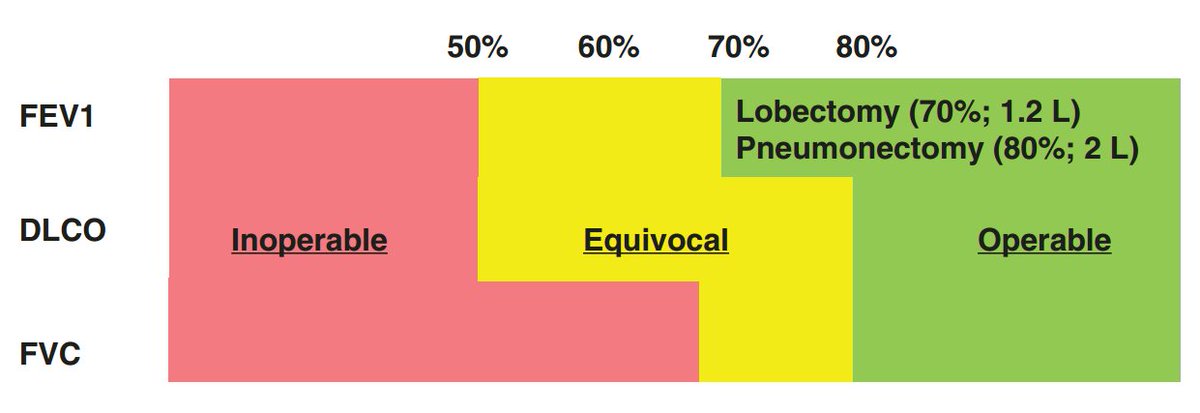
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC Stereotactic body radiotherapy is a great option as definitive tx for lung ca, esp if inoperable. However, SBRT near the central "no fly zone" is associated with worse toxicity.
More from @JoeChangMD:
ncbi.nlm.nih.gov/pubmed/24661665
#LCSM
More from @JoeChangMD:
ncbi.nlm.nih.gov/pubmed/24661665
#LCSM
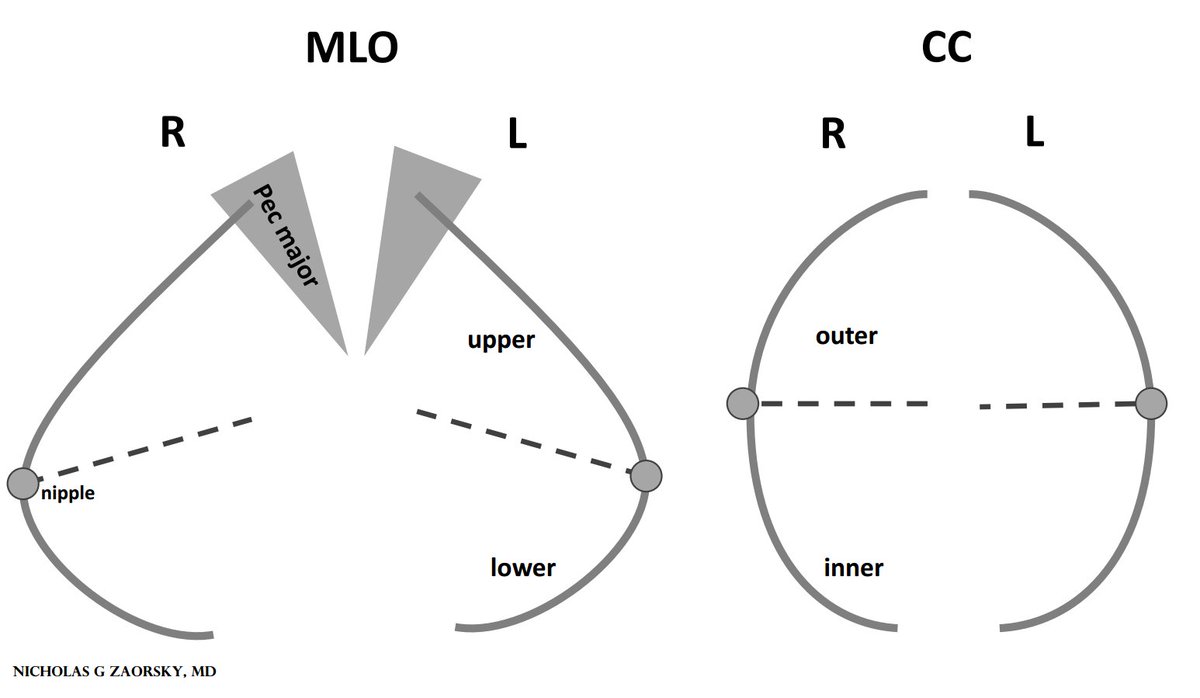
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD Mammographs typically have 2 views: medio-lateral-oblique (MLO) and cranio-caudal (CC).
Here they are simplified. Sometimes, less is more in an illustration.
#BCSM
Here they are simplified. Sometimes, less is more in an illustration.
#BCSM
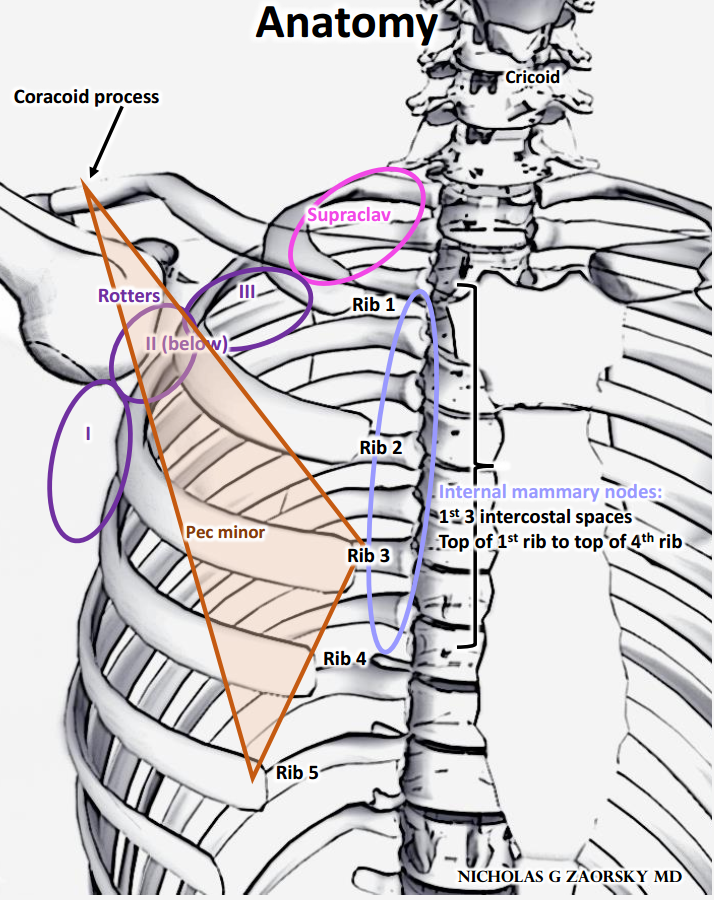
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD Lymph node stations for breast cancer
I: lateral to pec minor
II: under pec minor
III: medial to pec minor
IM nodes are from top 1st rib to top of 4th rib
Lumpectomy + LND typically only gets levels I, II.
In #RadOnc, "treat the nodes" is RT to I-III + supraclav.
#bcsm
I: lateral to pec minor
II: under pec minor
III: medial to pec minor
IM nodes are from top 1st rib to top of 4th rib
Lumpectomy + LND typically only gets levels I, II.
In #RadOnc, "treat the nodes" is RT to I-III + supraclav.
#bcsm
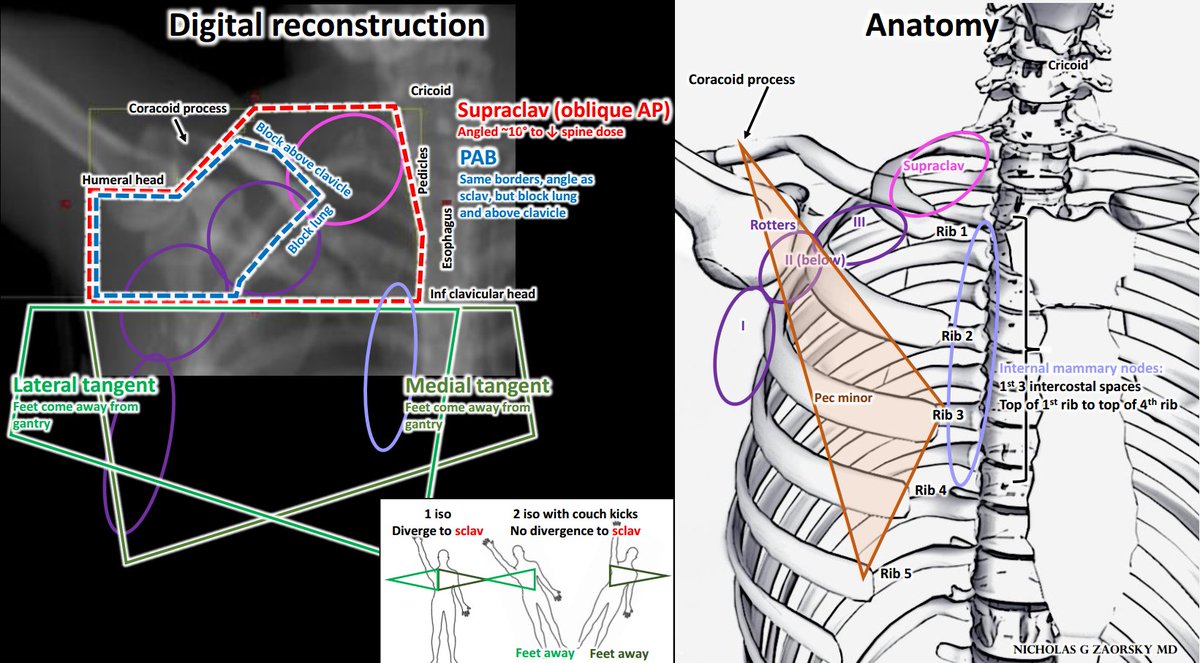
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD For breast RT, there are 2 tangent beams (green).
Supraclav beam is oblique AP.
Posterior axillary boost similar but block lung + above clavicle.
If treating breast + LNs, avoid divergence of tangents (move feet away from gantry)
Thanks for teaching me @hayesradonc @NickiSimone4
Supraclav beam is oblique AP.
Posterior axillary boost similar but block lung + above clavicle.
If treating breast + LNs, avoid divergence of tangents (move feet away from gantry)
Thanks for teaching me @hayesradonc @NickiSimone4
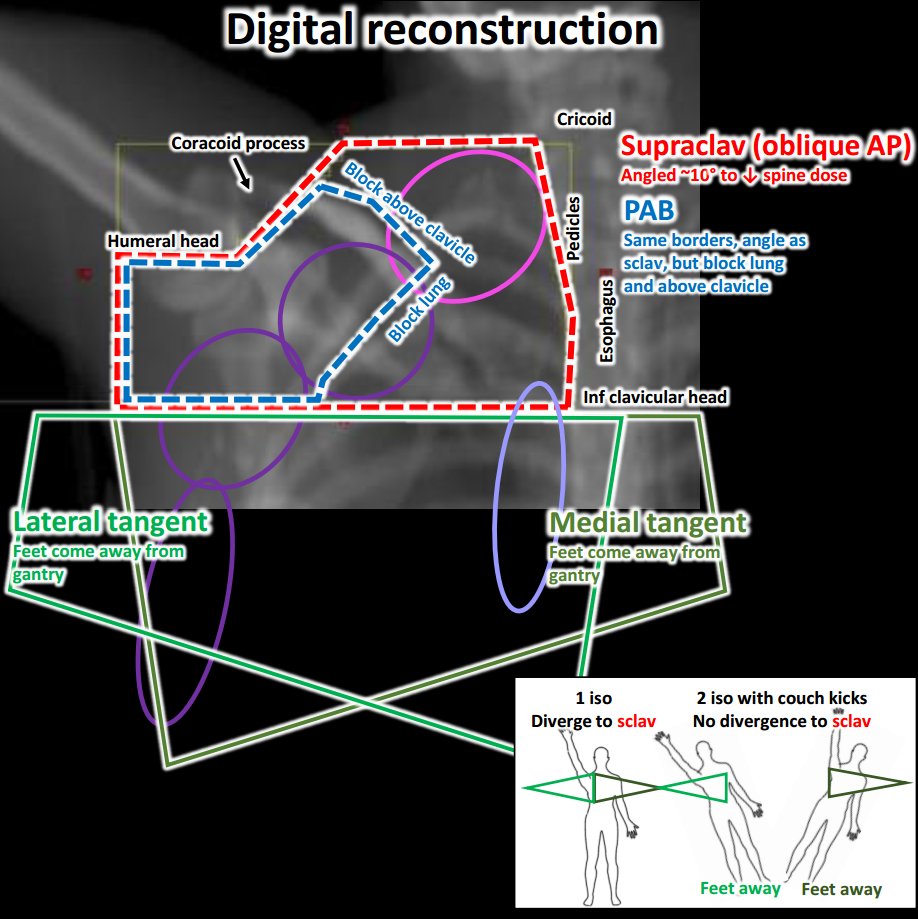
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 Here are the digitally reconstructed radiograph and the anatomy juxtaposed.
Inf border of clavicular head is a good bony landmark.
#BCSM
Inf border of clavicular head is a good bony landmark.
#BCSM
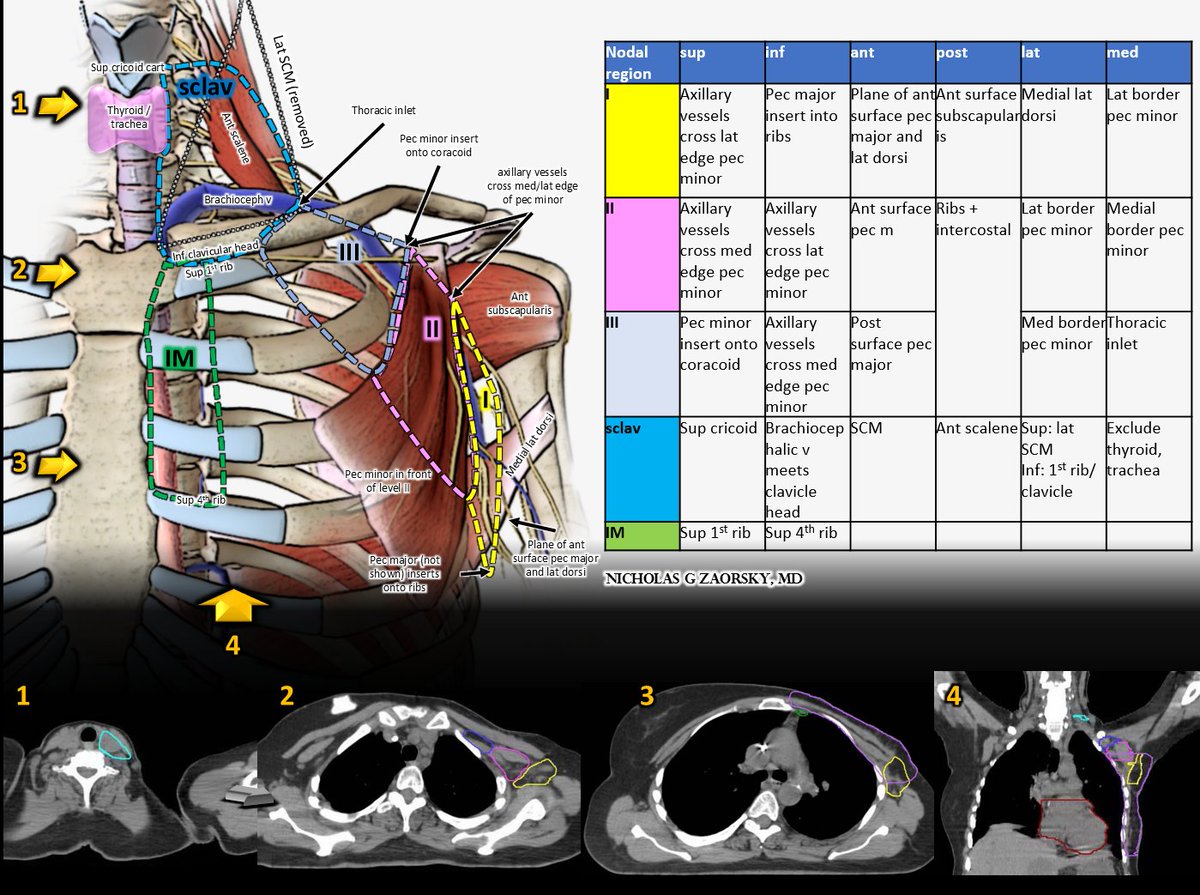
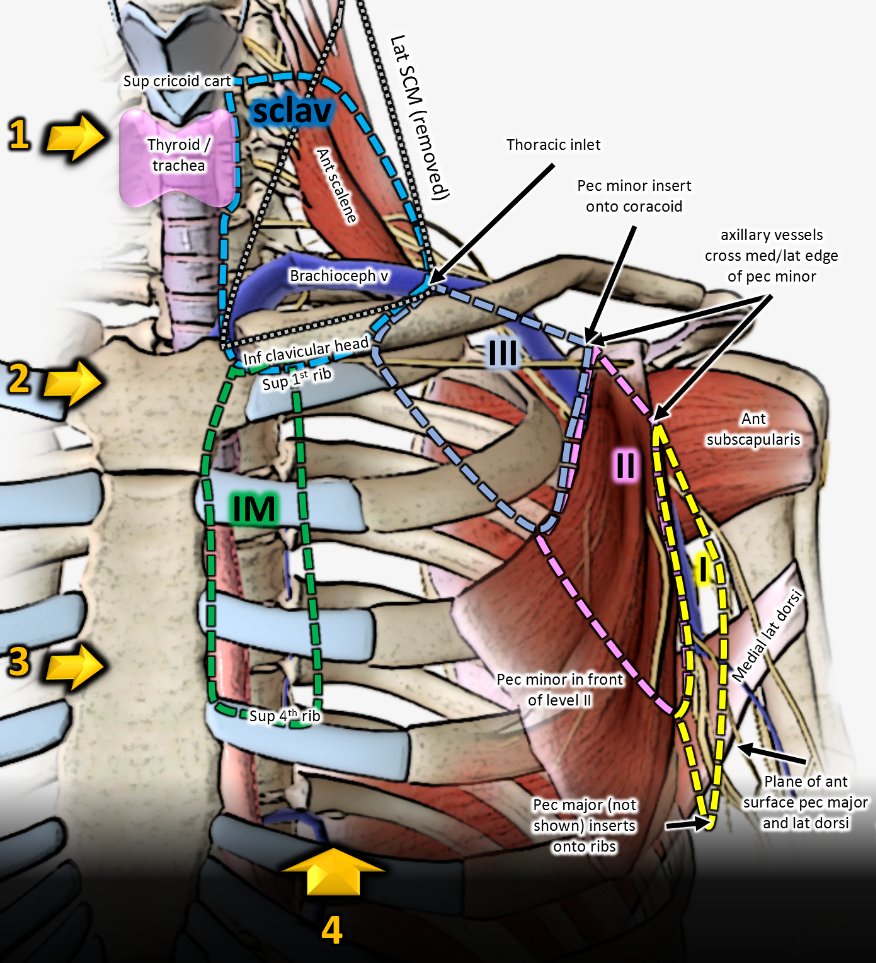
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 Contouring lymph node stations based on @NRGonc contouring atlas. #bcsm
Anatomic landmarks on 4 key CT slices, with corresponding arrows on 3D model. Slices #1-3 are axial; 4 is coronal.
There are 5 main stations: I, II, III, sclav, IM.
rtog.org/CoreLab/Contou…
Anatomic landmarks on 4 key CT slices, with corresponding arrows on 3D model. Slices #1-3 are axial; 4 is coronal.
There are 5 main stations: I, II, III, sclav, IM.
rtog.org/CoreLab/Contou…
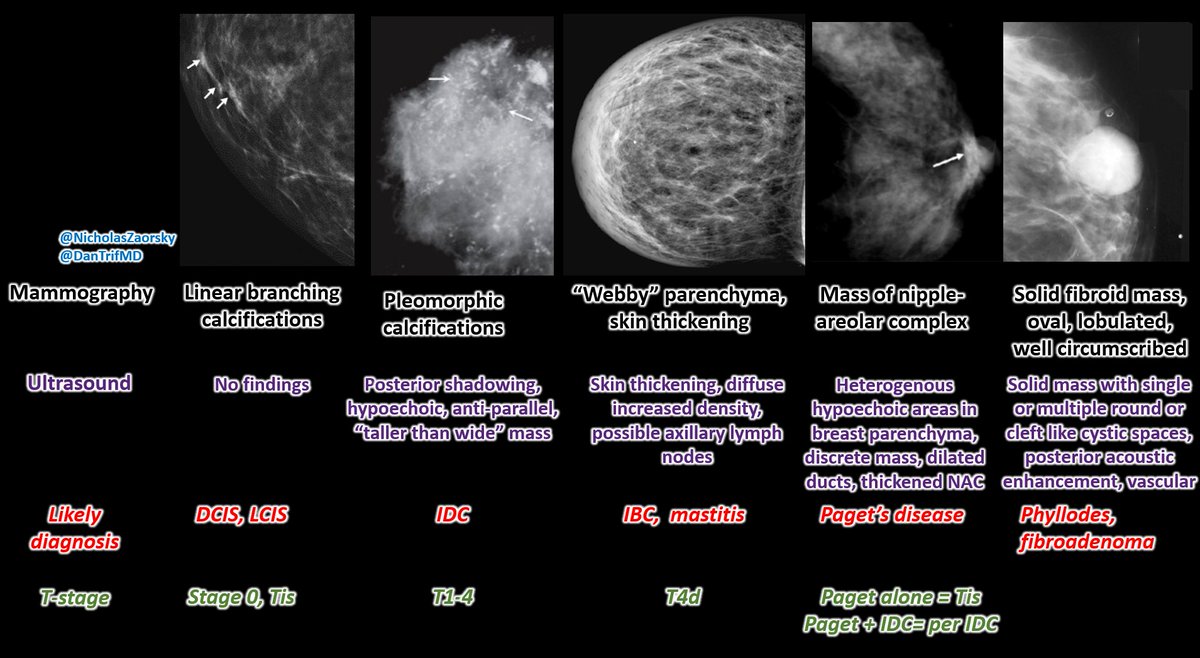
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 Mammography interpretation in as few words as possible.
When you see these findings, consider these diagnoses.
#bcsm
When you see these findings, consider these diagnoses.
#bcsm
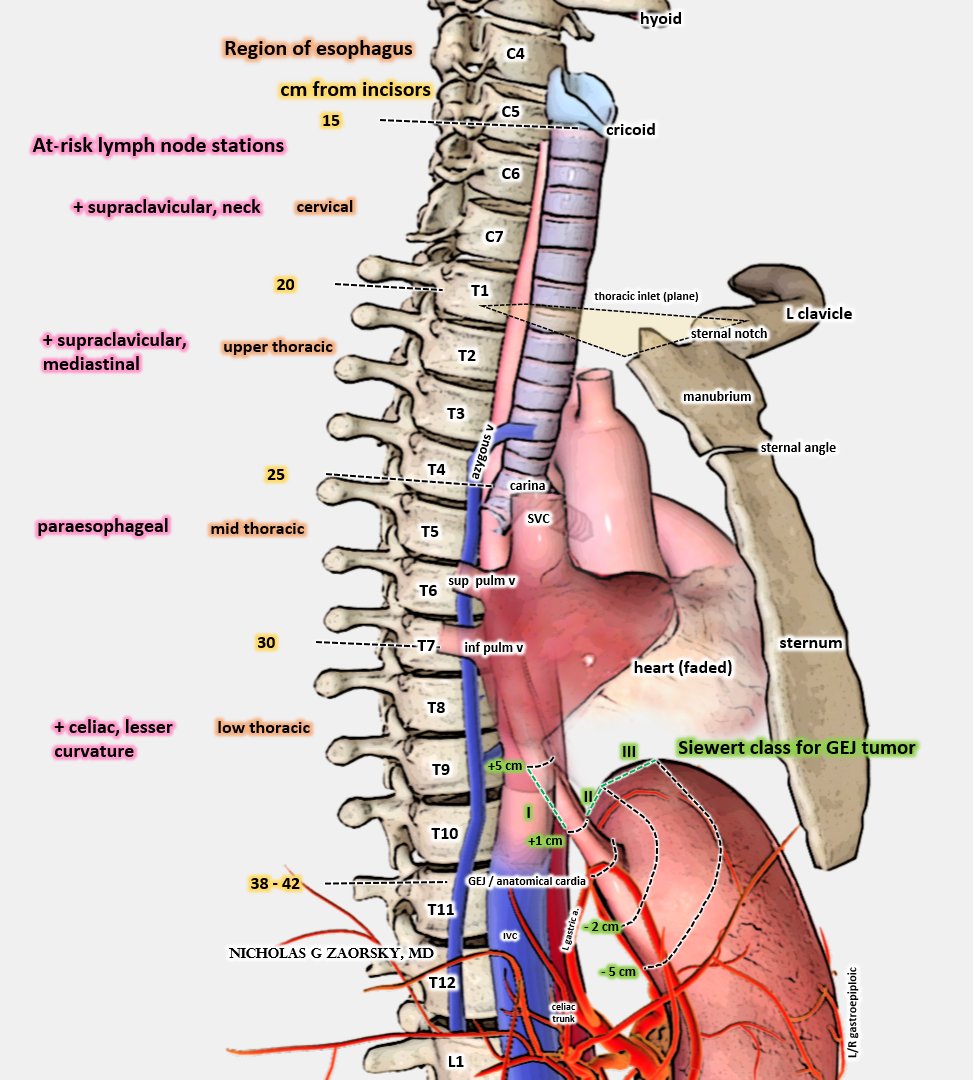
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 Esophageal cancer w @LeilaTchelebi.
Distance from incisors matters.
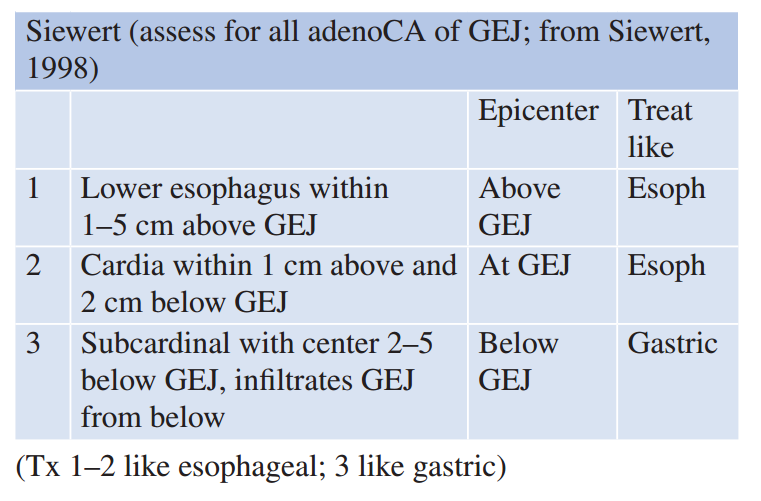
Near gastroesophageal junction, tumors treated like esophagus vs stomach ca based on Siewert.
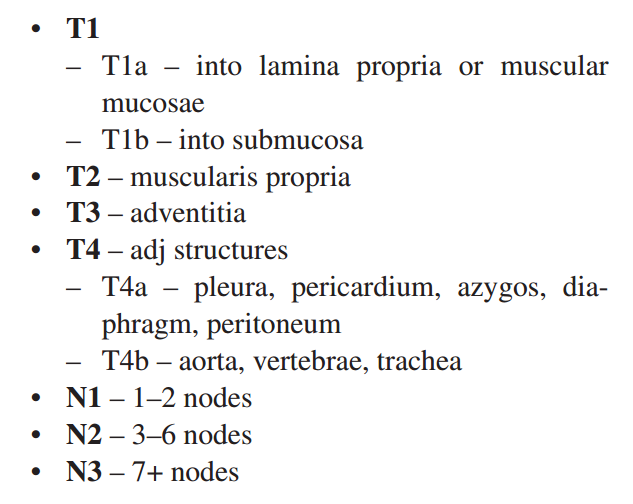
T/N stage depends on depth. T1b has 20% risk of LN involvement!
Thx for input @NirajGusani
#esocsm #GIcsm
Distance from incisors matters.
Near gastroesophageal junction, tumors treated like esophagus vs stomach ca based on Siewert.
T/N stage depends on depth. T1b has 20% risk of LN involvement!
Thx for input @NirajGusani
#esocsm #GIcsm

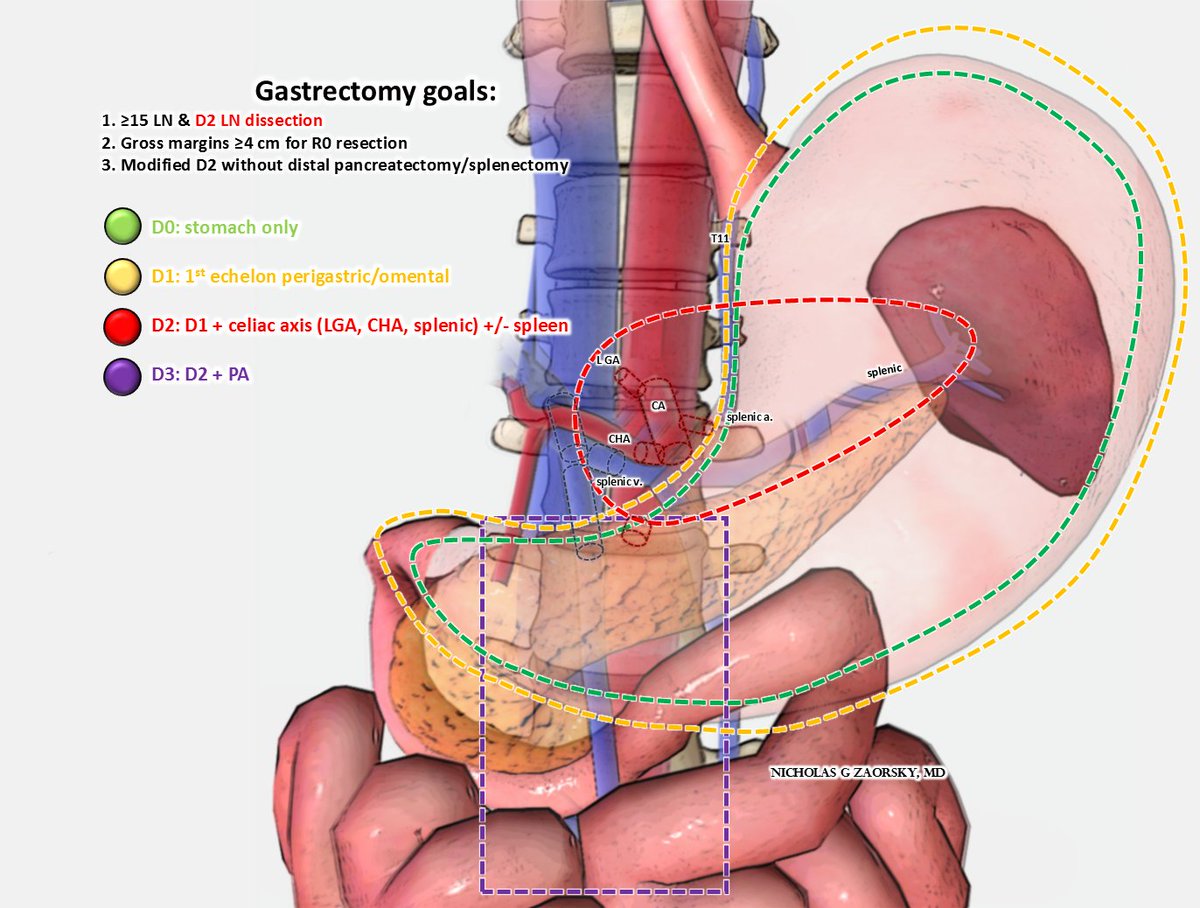
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani For gastric cancer, lymph nodes removed along w the stomach.
No RCT for D1 vs D2.
D2 dissections are associated with more complications, but improved CSS.
Historically, in US, D0 dissections more common (e.g. INT 0116 trial); in contrast, in Asia, D2+ dissections common.
#GICSM
No RCT for D1 vs D2.
D2 dissections are associated with more complications, but improved CSS.
Historically, in US, D0 dissections more common (e.g. INT 0116 trial); in contrast, in Asia, D2+ dissections common.
#GICSM
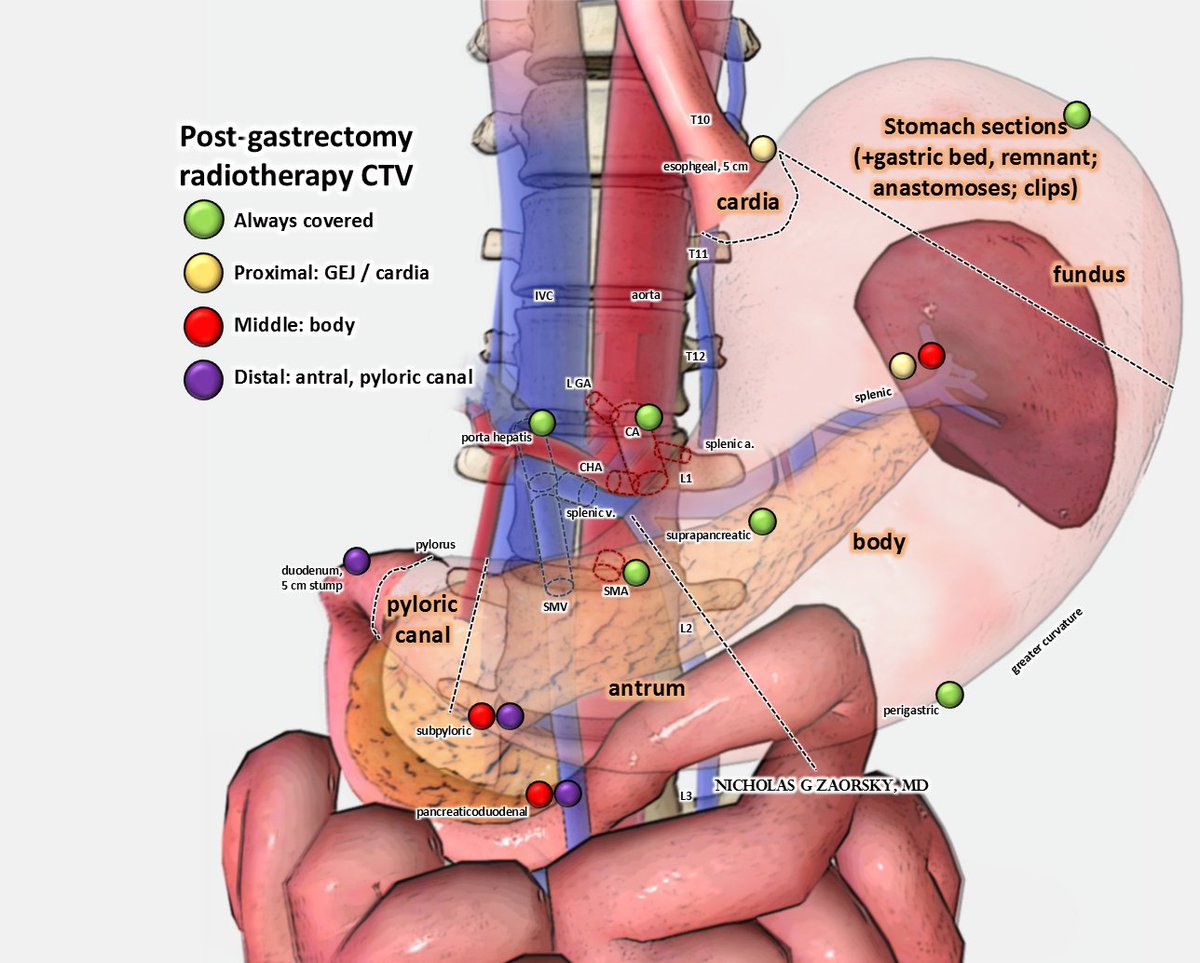
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani If delivering post op radiation therapy for gastric cancer, consider covering the following LNs
#GICSM
#GICSM
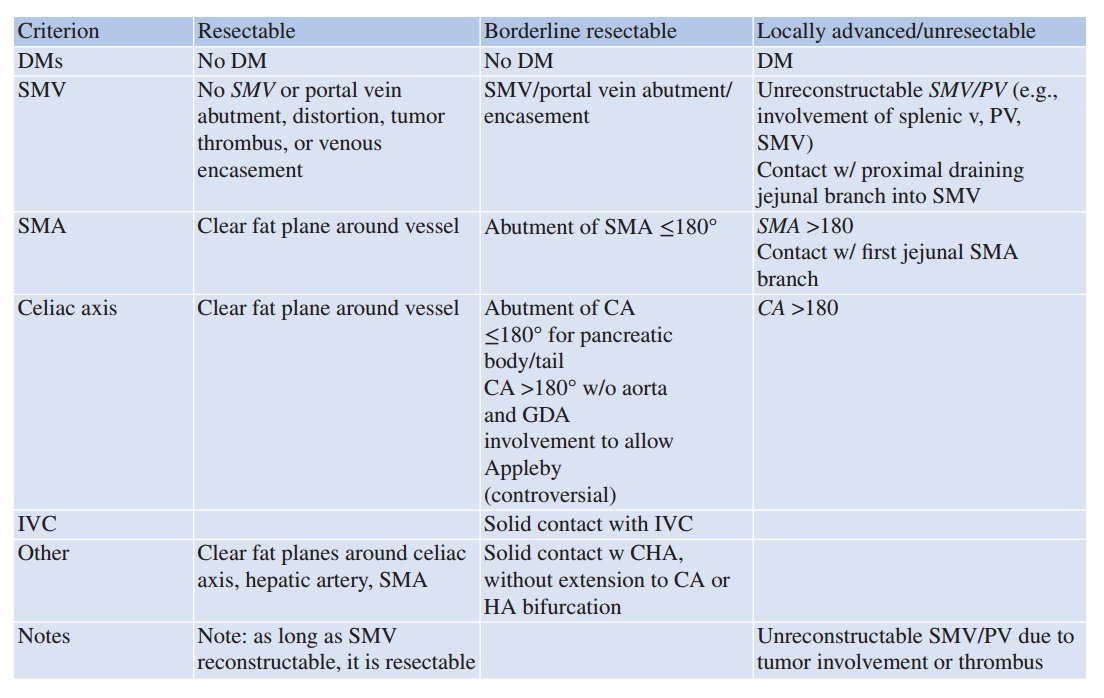
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani Pancreatic cancer resectability in as few words as possible.
Blue is tumor. Red is critical vessel like the SMA, celiac axis.
I'll defer to the experts though, @SanjaySReddy @NirajGusani
#PancreaticCancer
Blue is tumor. Red is critical vessel like the SMA, celiac axis.
I'll defer to the experts though, @SanjaySReddy @NirajGusani
#PancreaticCancer
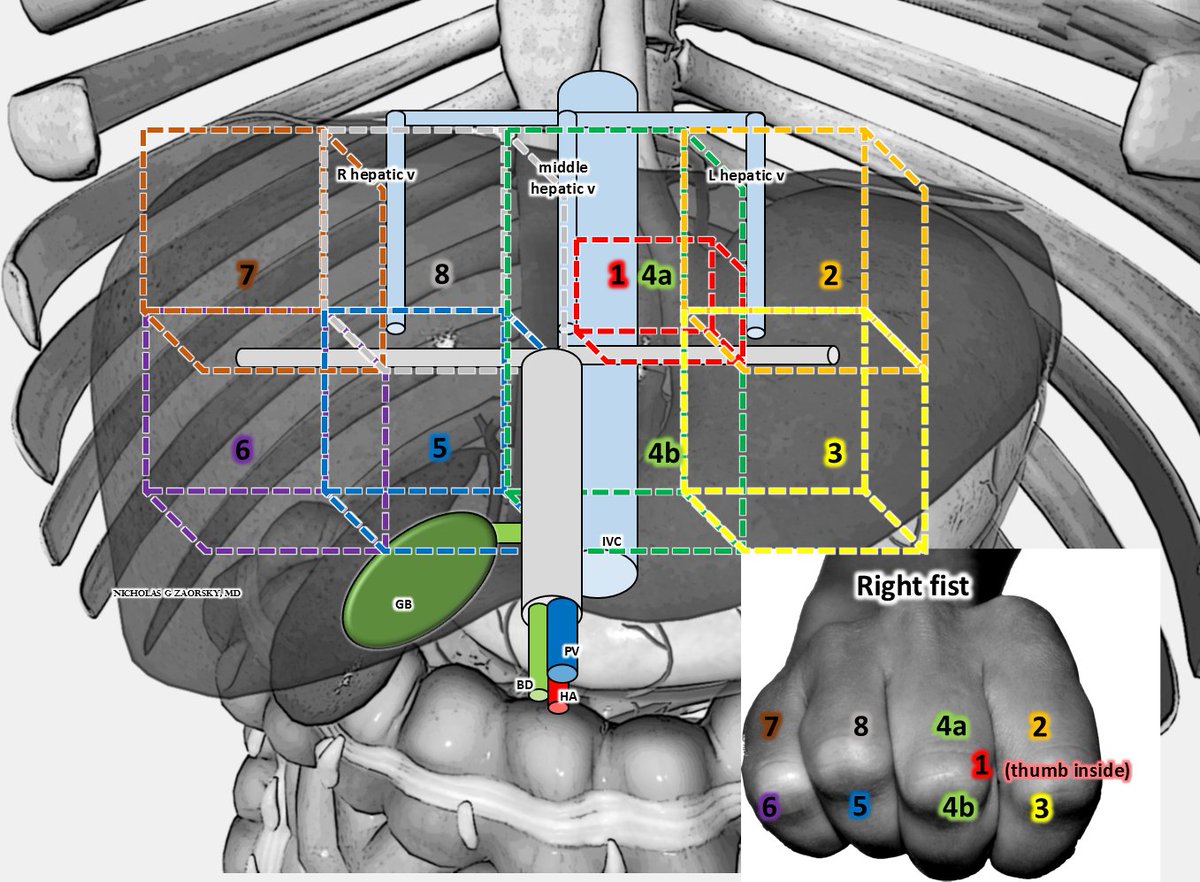
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy Liver anatomy explained using your right fist.
#GICSM #LiverCancer #Cholangiocarcinoma
#GICSM #LiverCancer #Cholangiocarcinoma
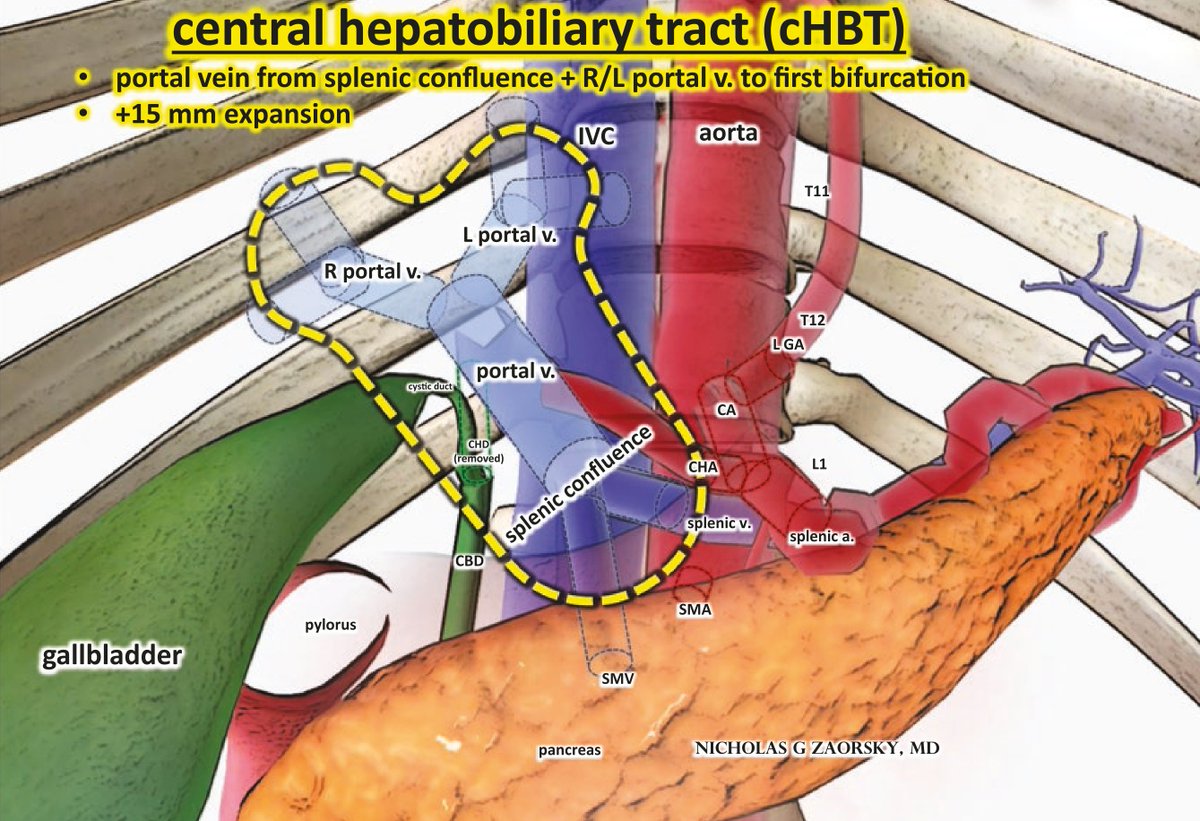
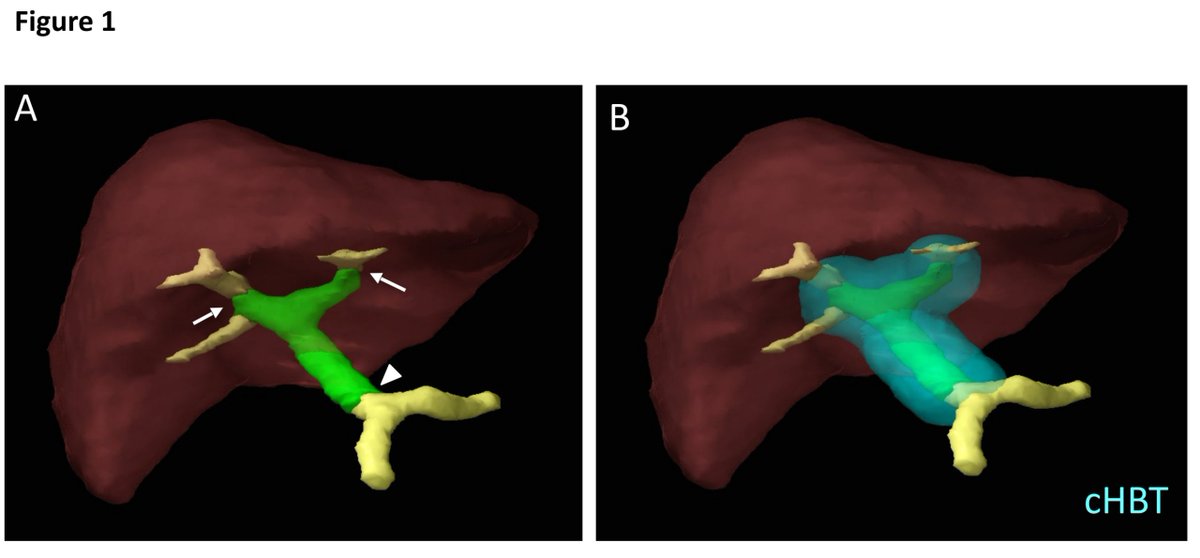
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy Similar to the "no fly zone" in lung cancer, there is one in liver cancer
Work from Daniel T Chang, @ACKoongMDPhD
ncbi.nlm.nih.gov/pubmed/25659885
#GICSM
Work from Daniel T Chang, @ACKoongMDPhD
ncbi.nlm.nih.gov/pubmed/25659885
#GICSM
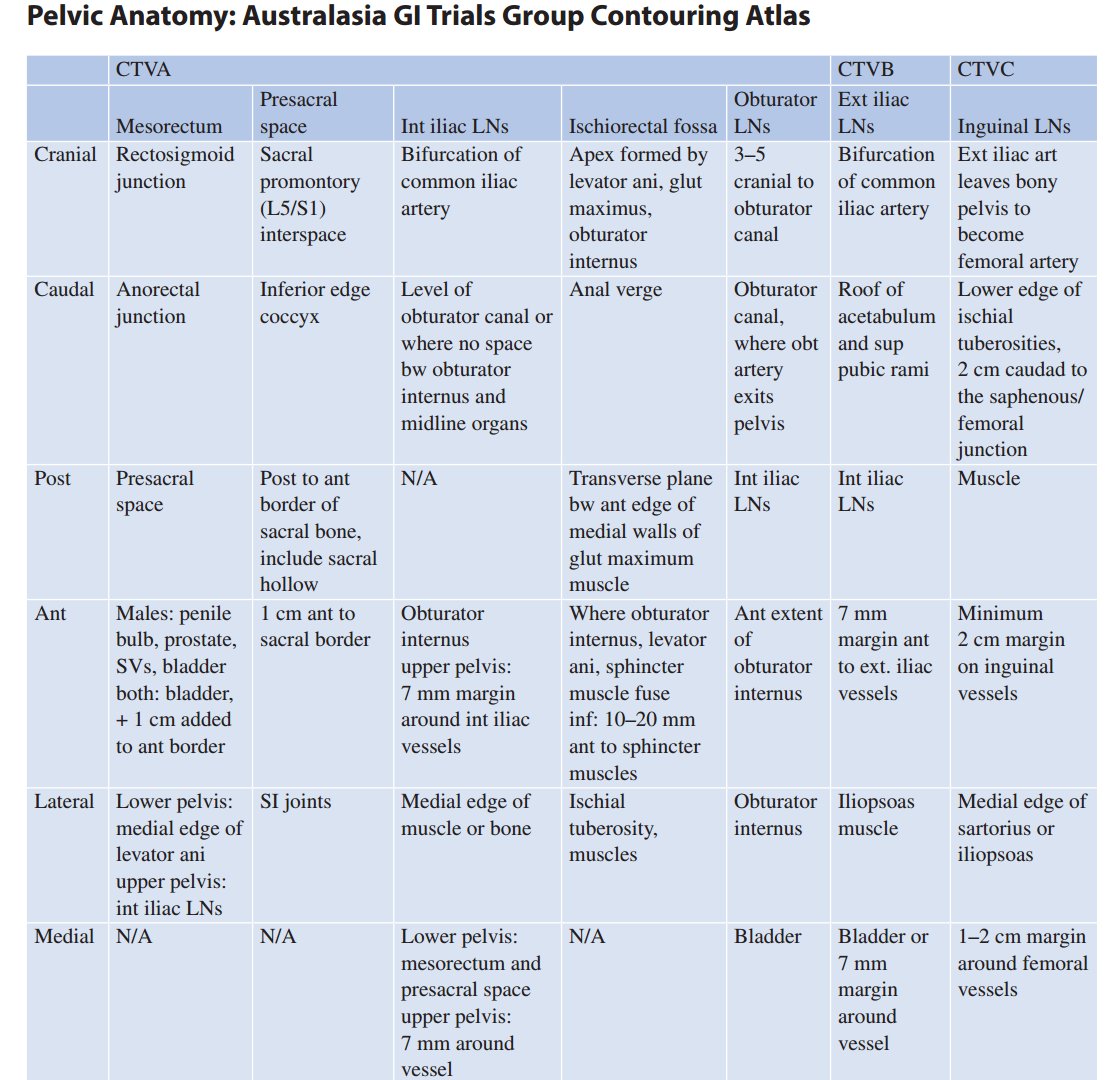
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD Pelvic anatomy, lateral and AP
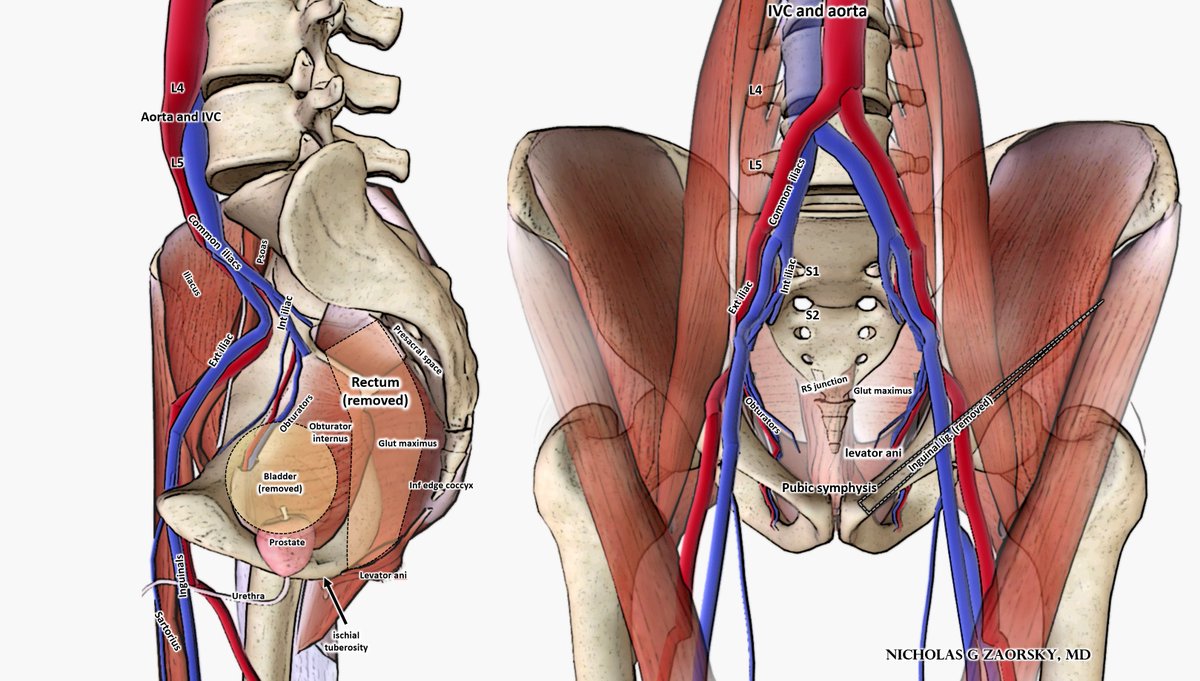
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD LN definitions come from Australasian Gastrointestinal Trials Group (AGITG) consensus guidelines, from @lisakachnic1
ncbi.nlm.nih.gov/pubmed/22401917
ncbi.nlm.nih.gov/pubmed/22401917
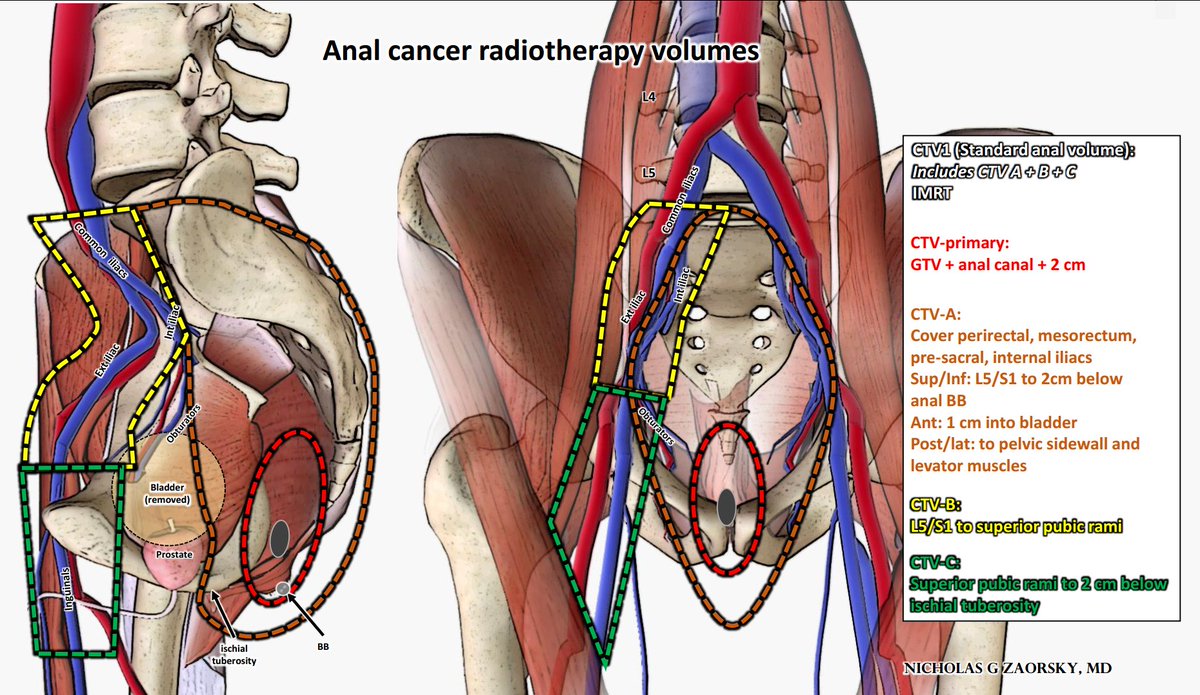
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD @lisakachnic1 For anal cancer, treatment typically includes CTV A, B, C, from @NRGonc anorectal contouring atlas
rtog.org/LinkClick.aspx…
From chapter with @LeilaTchelebi
#GICSM
rtog.org/LinkClick.aspx…
From chapter with @LeilaTchelebi
#GICSM
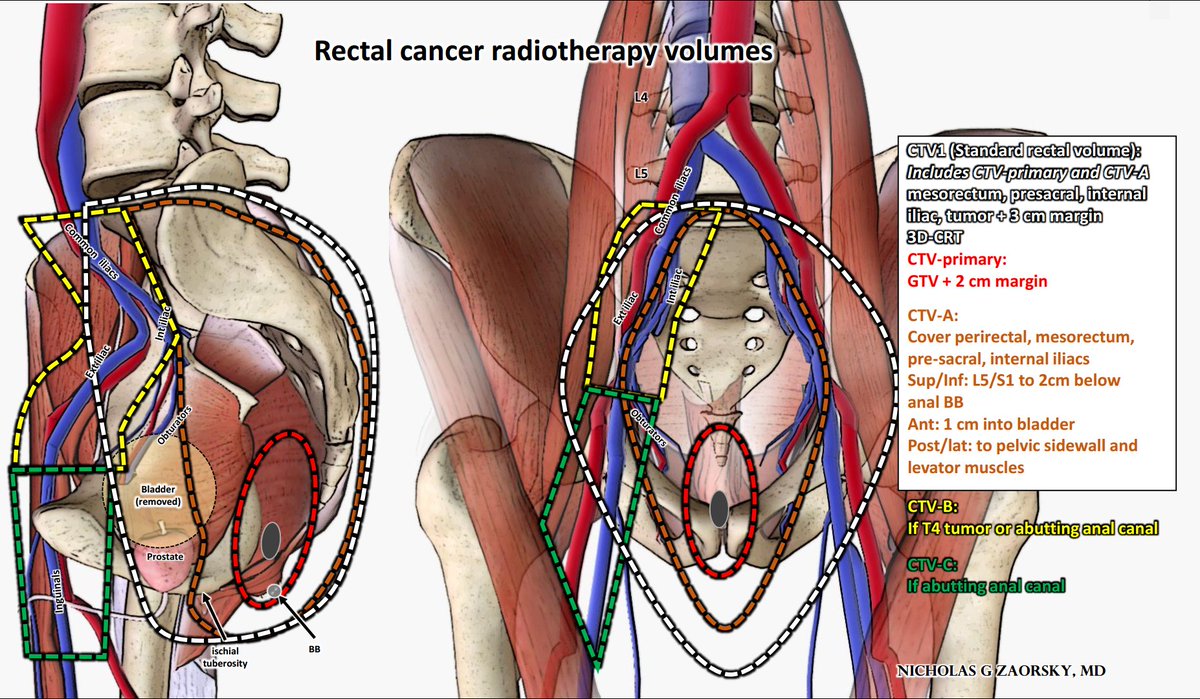
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD @lisakachnic1 For rectal cancer, treatment typically includes just CTV A, from @NRGonc anorectal contouring atlas
rtog.org/LinkClick.aspx…
From chapter with @LeilaTchelebi
#GICSM
rtog.org/LinkClick.aspx…
From chapter with @LeilaTchelebi
#GICSM
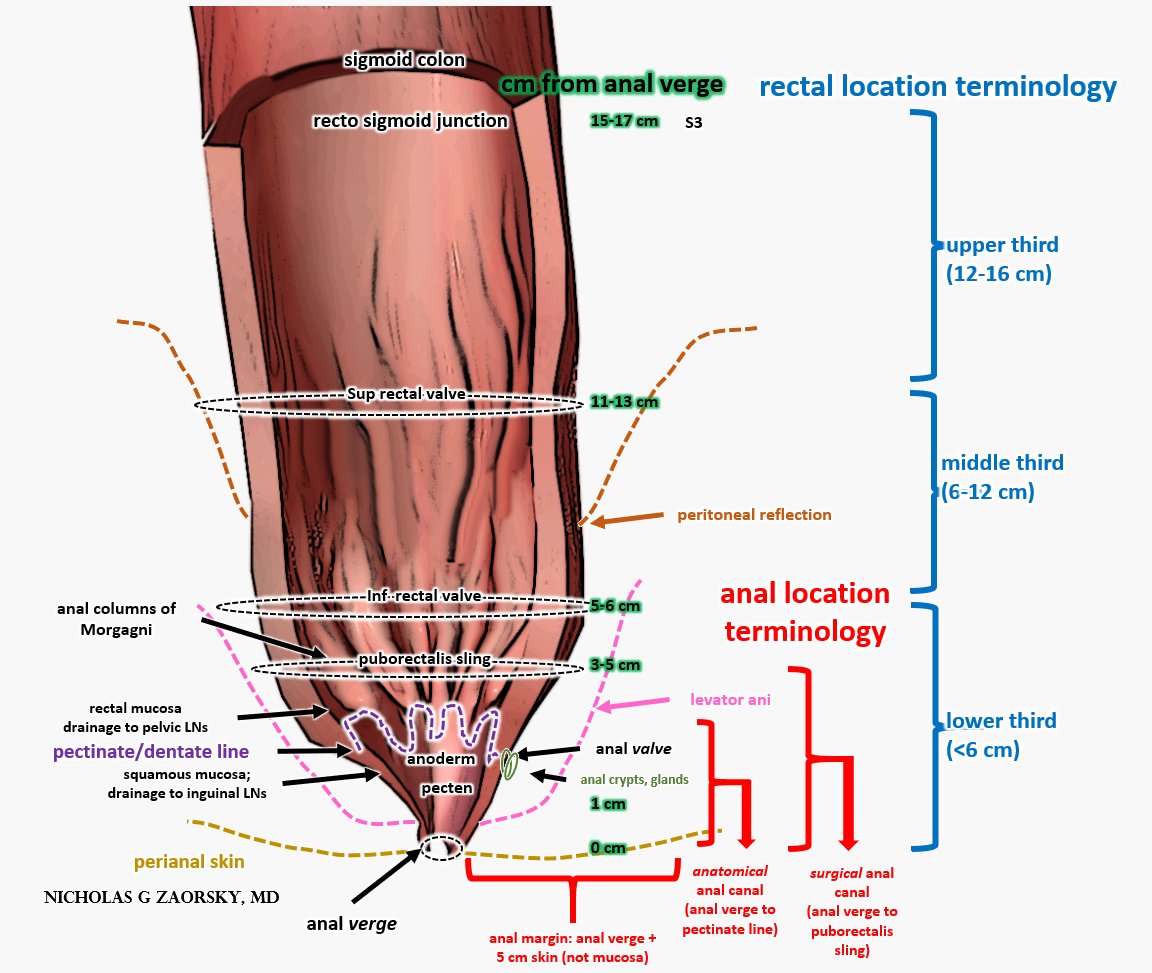
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD @lisakachnic1 Anal and rectal cancer anatomy and terminology
From chapter with @LeilaTchelebi
More great info from @eContourRadOnc @ErinGillespieMD
econtour.org/training/recta…
#GICSM #colorectalcancer #Colorectalsurgery
From chapter with @LeilaTchelebi
More great info from @eContourRadOnc @ErinGillespieMD
econtour.org/training/recta…
#GICSM #colorectalcancer #Colorectalsurgery
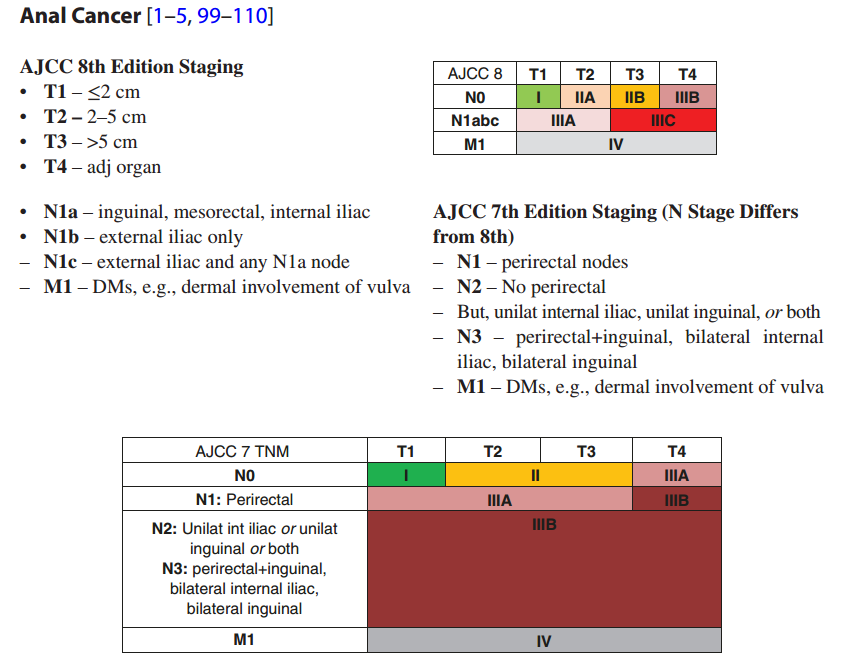
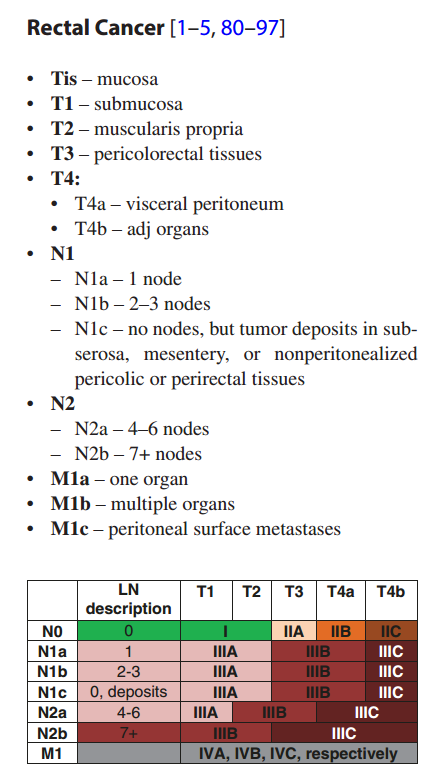
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD @lisakachnic1 @eContourRadOnc @ErinGillespieMD The @AJCCancer anal cancer staging changed from 7th to 8th edition. Rectal cancer staging mostly unchanged.
Chapter from @LeilaTchelebi
Chapter from @LeilaTchelebi
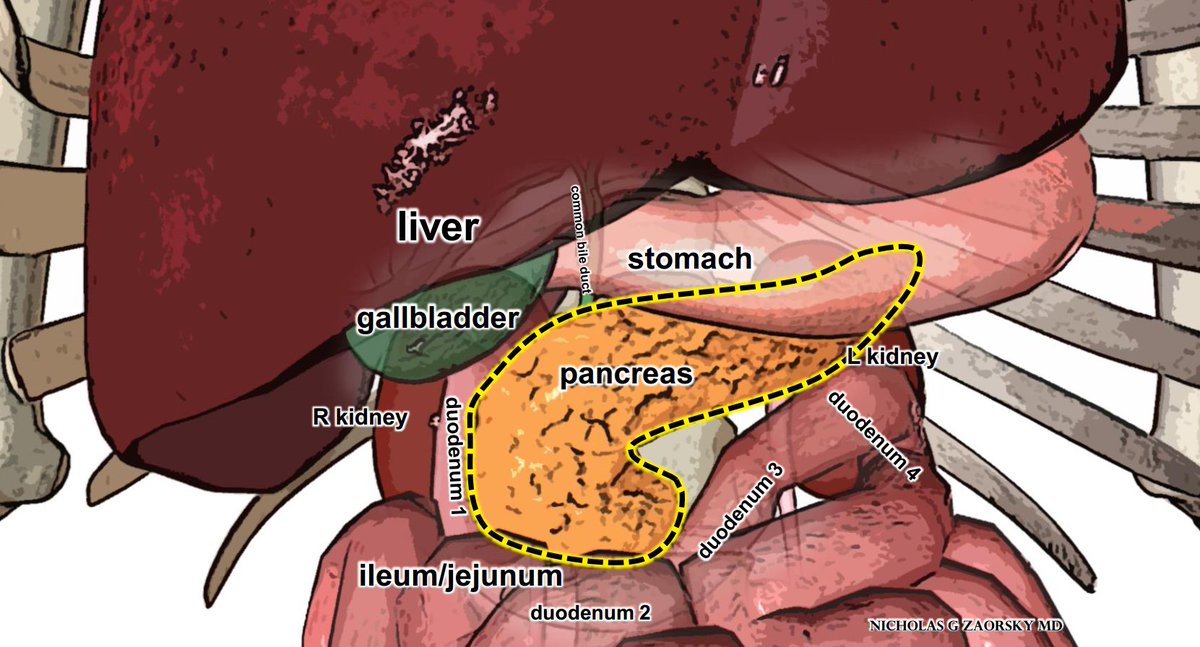
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD @lisakachnic1 @eContourRadOnc @ErinGillespieMD One of the reasons pancreatic cancer is hard to treat: the organ is surrounded by exquisitely radiosensitive structures. Stomach is superior, 4 segments of the duodenum are lateral and inferior, ileum/jejunum nearby.
From paper with @LeilaTchelebi
#PancreaticCancer #RadOnc
From paper with @LeilaTchelebi
#PancreaticCancer #RadOnc
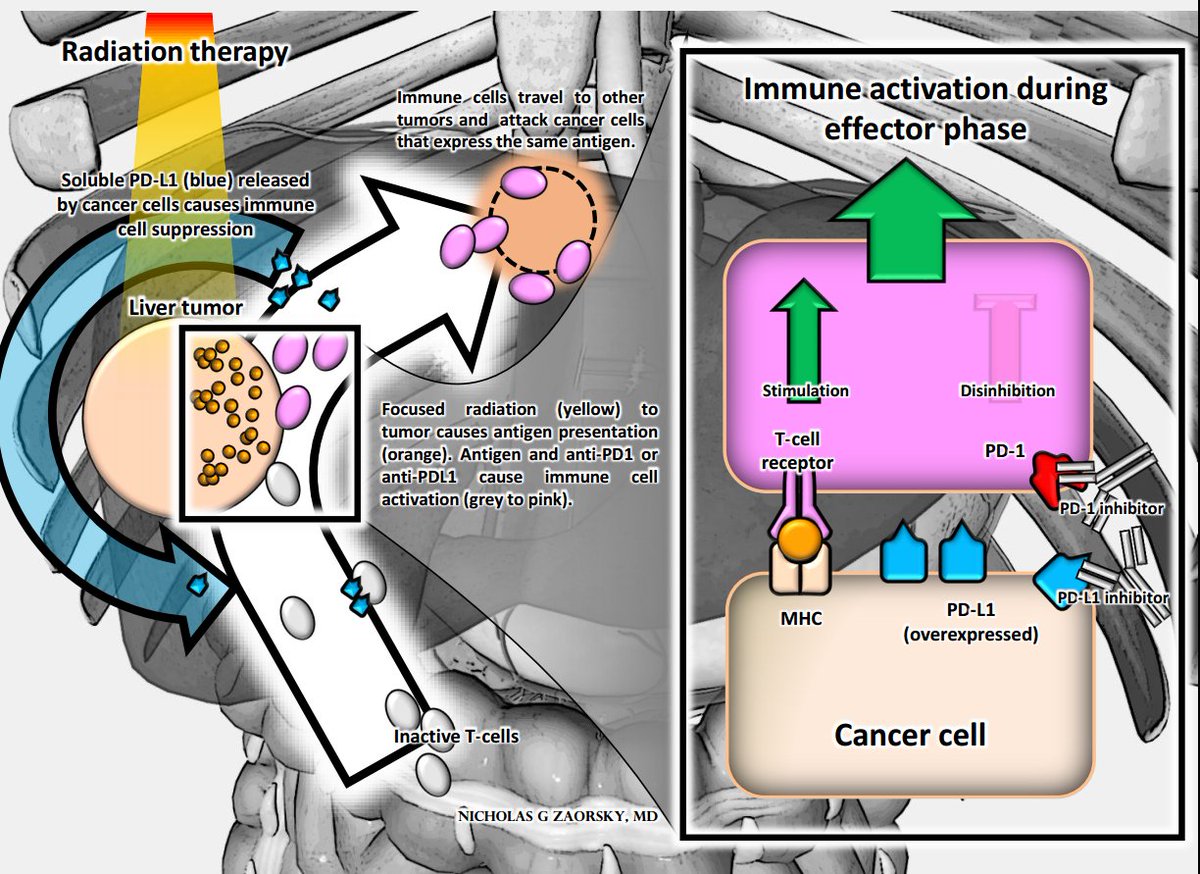
@DanTrifMD @ARRO_org @SpringerNature @cgr0105 @TheUSMLE @TheASNR @RadiologyACR @vinaigondi @NRGonc @NeuroOnc @AANSNeurosurg @FightBrainTumor @lgksociety @Accuray @EricLehrer @UCSDHealth @HenryParkMD @AJCCancer @AmerDentalAssn @LungAssociation @IASLC @JoeChangMD @hayesradonc @NickiSimone4 @LeilaTchelebi @NirajGusani @SanjaySReddy @ACKoongMDPhD @lisakachnic1 @eContourRadOnc @ErinGillespieMD Stereotactic radiotherapy use is increasing for upper GI cancers like those of the liver, pancreas. For certain tumors, there is biologic rationale to combine radiotherapy + immune checkpoint inhibition. Radiotherapy "primes" the immune system.
ncbi.nlm.nih.gov/pubmed/29301352
ncbi.nlm.nih.gov/pubmed/29301352