I'm inclined to share a few thoughts on this (rather nauseating) news, having worked at Practice Fusion for a couple of yrs, though not when this episode occurred.
As @chrissyfarr notes, PF has become a bit of a cautionary tale. Perhaps there are useful lessons in that tale. 1/n
As @chrissyfarr notes, PF has become a bit of a cautionary tale. Perhaps there are useful lessons in that tale. 1/n
As full disclosure, this is partly speculative. I was at the company in the 2013 - 2015 time frame, and did not work on the pharma/life sciences business at any point.
From what I can glean via purely public info, the opioid episode seems to have happened in late 2016 and 2017.
From what I can glean via purely public info, the opioid episode seems to have happened in late 2016 and 2017.
At the outset, PF's basic thesis was arguably similar to @flatironhealth or perhaps AmeriSource's IntrinsiQ.
I.e. that cloud-based EHRs could help transform a fragmented care delivery landscape into a connected clinical community, while generating useful data for research/RWE.
I.e. that cloud-based EHRs could help transform a fragmented care delivery landscape into a connected clinical community, while generating useful data for research/RWE.
Those research-oriented businesses, however, take years to develop. In the meantime, pharma advertising is a huge pool of spend, and a straightforward sales opportunity. In 2016, for example, drugmakers spent ~$20 billion advertising to physicians and other prescribers. 

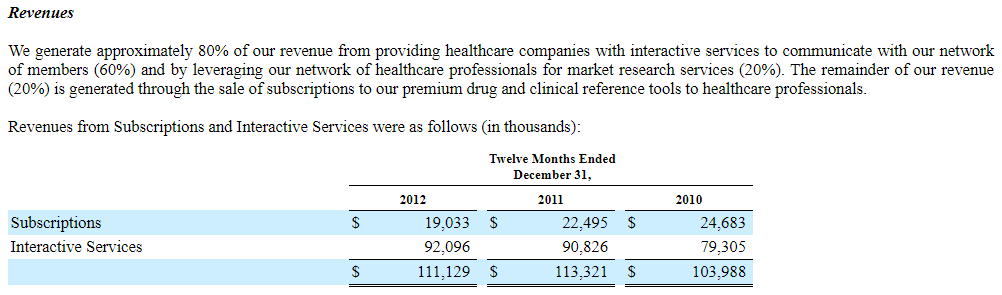
Pharma ad dollars were also a well-trodden path. McKesson's iKnowMed oncology EMR has historically sent pharma-sponsored emails to users, some Allscripts workflows include banner ads, and Epocrates (now owned by Athena) derived ~80% of revenue (👇) from pharma marketing.
Go further back, and you find pharma marketers putting their brands on doctors' prescription pads, and radiology clinics filling orthopedic surgeons' offices w/ branded clipboards and imaging order forms - the analog versions of a banner ad in the e-prescribing/ordering workflow.
But, once you choose that ad-driven path, commercial gravity tugs in the direction of selling more ad inventory, and creating more effective advertising tools (See: Facebook). All the more so, perhaps, if the company is venture-backed and trying to reach breakeven.
I can't be sure, but the likely template for the opioid campaign came in a totally different area: Vaccination.
Specifically, in 2014/15, PF worked with Merck to develop workflow tools based on CDC guidelines that would try to boost pneumococcal vaccination in the elderly.
Specifically, in 2014/15, PF worked with Merck to develop workflow tools based on CDC guidelines that would try to boost pneumococcal vaccination in the elderly.
That's no small thing - pneumonia contributes to ~600K hospitalizations annually for Medicare patients, yet ~1/3 of those >65 have not been vaccinated.
That campaign was reported at the time, in a largely positive light, and Merck's role was transparent:
forbes.com/sites/zinamouk…
That campaign was reported at the time, in a largely positive light, and Merck's role was transparent:
forbes.com/sites/zinamouk…
Still, reasonable people can disagree about this effort.
Obviously, Merck funded the work to sell more vaccine doses. On the other hand, channeling pharma resources in this way can serve public health - there are similar "uptake" incentives in some Hep C treatment contracts.
Obviously, Merck funded the work to sell more vaccine doses. On the other hand, channeling pharma resources in this way can serve public health - there are similar "uptake" incentives in some Hep C treatment contracts.
But then...applying this vaccination template to opioids is just an appalling, utterly inexcusable lapse in ethics and basic judgment.
FWIW, I also don't think "hindsight" claims are an excuse - Sam Quinones's "Dreamland" came out in 2015, and Meier's "Pain Killer" years before.
FWIW, I also don't think "hindsight" claims are an excuse - Sam Quinones's "Dreamland" came out in 2015, and Meier's "Pain Killer" years before.
We can get a bit of insight into what the opioid decision support campaign probably looked like - as with the vaccination program, it was apparently shared publicly at the time. In this case, as a poster at a 2017 AMIA conference.
See 👇 (found on the public web)
See 👇 (found on the public web)

This was shared as research on decision support efficacy, in a legitimate forum, w/ clear acknowledgment of Purdue's involvement.
And - at least in this case - the program does not seem to have explicitly nudged physicians to prescribe pain meds, only to document a pain score.
And - at least in this case - the program does not seem to have explicitly nudged physicians to prescribe pain meds, only to document a pain score.
And yet... Obviously Purdue paid for the program for a reason, and that reason almost certainly involved selling pills (I mean...c'mon).
Most likely, nudging an MD to document pain boosts the propensity to prescribe pain pills. Just like those "talk to your doctor about X" ads.
Most likely, nudging an MD to document pain boosts the propensity to prescribe pain pills. Just like those "talk to your doctor about X" ads.
One way or another, it is difficult to even imagine the internal decision cycle that approved this work, without triggering ethical or legal alarm bells. In a $45 - 50M business, a $1M deal would presumably have been discussed at the Board level, at least in passing.
Zoom out, and perhaps this is a reminder of the profound risk when an (overcapitalized?) startup is scrambling to make its number amidst the deeply conflicted - and often squarely unethical - financial practices that dot American healthcare.
Another lesson probably speaks to early business model choices.
It is harder to build a business focused on clinical quality or patient value than to milk the status quo. But once established, revenue models take on a life and logic of their own. Please choose carefully.
It is harder to build a business focused on clinical quality or patient value than to milk the status quo. But once established, revenue models take on a life and logic of their own. Please choose carefully.
But whatever the pressure, ethics just have to win, so leadership matters. Some things are just wrong.
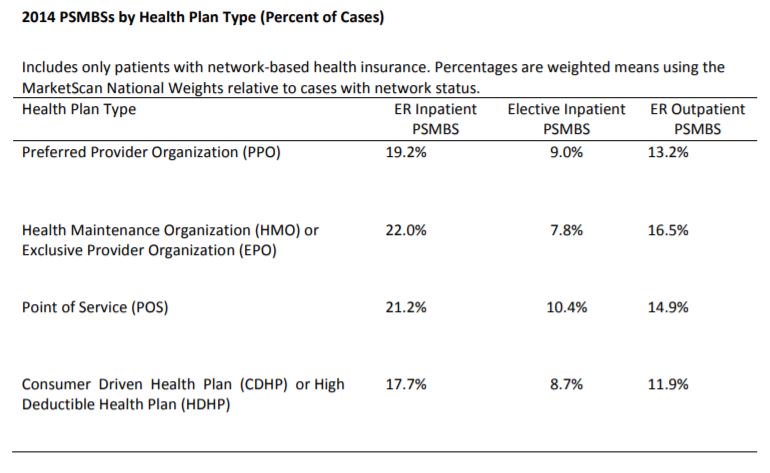
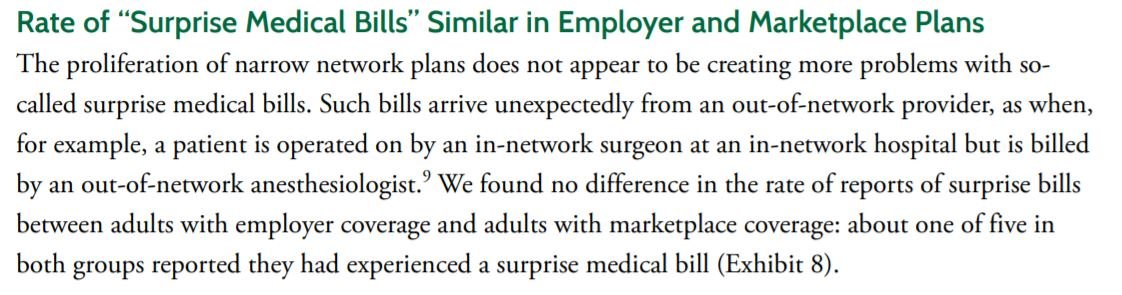
True of surprise billing, extractive hospital collections, and Valeant-style abusive drug pricing. And it sure as hell is wrong to push addictive pills through an EHR. /n
True of surprise billing, extractive hospital collections, and Valeant-style abusive drug pricing. And it sure as hell is wrong to push addictive pills through an EHR. /n