
One of the more interesting aspects of retrospective studies is the opportunity to examine historical definitions of common clinical entities and test just how strong these foundations really are.
Herewith, a thread.
Herewith, a thread.
1. Gather round, friends. These are the current WHO recommendations for the diagnosis of anaemia, published in 2011. 

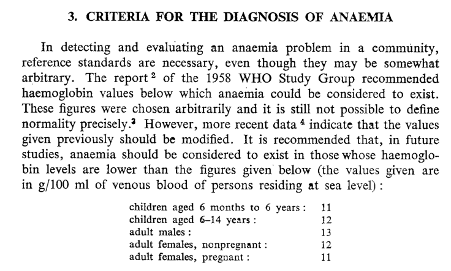
2. And, for comparison, these are the original WHO definitions, published in 1959. At the time, the committee stated that “it is necessary to have standards of reference, even if they are somewhat arbitrary”; so what we are looking at here is at best, an educated guess.

3. So how did the WHO justified picking these specific cut offs? To get that answer, we have to jump forward another eight years to 1968, when the WHO had another crack at it (this time with evidence).
4. 4.Now if these numbers look fairly similar to the 2011 WHO definition, it’s because they are. So, for the definition to remain largely unchanged for 40 years, the evidence on which it is based must be pretty good, right?
5. Well, yes and no. There’s no question that the WHO based these definitions on the best available evidence at the time. However, that doesn’t mean that by modern standards, it was comprehensive.
6. The WHO based most of their evidence on three observational studies, the largest of which was in Welsh coal miners. The remaining data was unpublished except for one paper which was in Swedish (and like many native English speakers, I am regrettably monolingual).
7. First of all, women are underrepresented. Secondly, iron status was only assessed in a very small number of participants. Even taking into account these (very) small numbers, women have a lower TSAT than men, reflecting a higher incidence of iron deficiency.

8. Now, we as clinicians are taught to treat anaemia as a disease. It is not. Anaemia is a symptom of an underlying pathological process. In many cases, this underlying process is iron deficiency. And iron deficiency anaemia is end-stage iron deficiency.
9. So, given that we suspect that women are more iron deficient, is it any surprise that their mean haemoglobin concentration was lower? Of course, it’s not! But just because a lower haemoglobin concentration for women is more common does not mean that it is optimal.
10. Now let’s jump back to the present day and the article recently published in @Anaes_Journal (onlinelibrary.wiley.com/doi/10.1111/an…). This hypothesis appears to be supported by Table 2.
11. Thanks to a variety of inflammatory pathologies, ferritin can be difficult to interpret in the perioperative context. So, let’s look at the TSAT instead – as Hb decreases across the groups, TSAT falls, suggesting a “dose-response” relationship between the two.

12. This suggests that women with “borderline anaemia” are more likely to have a worse iron status. There also appears to be an inverse correlation between [Hb] and creatinine and a positive correlation between Hb and albumin, hinting at additional underlying pathology.
13. So how do we bring it all together? It appears that relative a [Hb] ≥ 130 g/L, a [Hb] of 120 – 129 g/L has associations with worse iron status, a higher creatinine and a lower albumin. Not only that, this is a common finding, present in 25% of women in this series.
14. The last step we need to take is to link these findings with patient-centred outcomes. An example of this is length of hospital stay. After all, most patients want to go home as soon as they after an operation.
15. Let’s look at Figure 2. Now, if the WHO definitions are correct, and pathological consequences of low [Hb] do not occur until [Hb] is < 120 g/L, then we should not see an inflection in the trend line until pre-operative [Hb] is below this threshold, right?
16. Wrong.

17. This is not the only negative outcome these data are associated with. We found statistically significant and negative associations between borderline anaemia and transfusion requirement, post-operative complications and fewer days alive and out of hospital at POD 30 and 90.
18. Whilst these findings lost statistical significance when we performed a matched cohort analysis, certain trends remained consistent with what we had observed. This loss of significance was unsurprising (but you’ll have to download and read the paper to discover why).
19. So, what can we conclude from these findings? Well, firstly, a [Hb] of 120 – 129 g/L in a woman presenting for major elective abdominal surgery is common, but not necessarily optimal. This is despite WHO guidance suggesting that this [Hb] is completely normal.
20. Secondly, this “borderline anaemia” may be associated with worse post-operative outcomes, particularly a longer length of hospital stay (our primary outcome). However, after correction for a variety of factors, the strength of these associations was attenuated.
21. Finally, this “borderline anaemia” is not just due to absolute iron deficiency per se but may also reflect inflammatory changes (leading to the anaemia of inflammation). Remember: anaemia is a symptom, not a pathology. You need to find the underlying cause to treat it.
22. Larger series are needed to help clear up these ambiguities. So, if you have expertise in large retrospective database studies or widespread prospective audit, and are interested in collaborating, you might like to help us answer this question. My DMs are open!


















