Teaching Rounds
Diarrhea - Part 1
3 Misleading Mimics
&
2 Key Questions
Join us #medtwitter & #medstudenttwitter
Diarrhea - Part 1
3 Misleading Mimics
&
2 Key Questions
Join us #medtwitter & #medstudenttwitter
Diarrhea = increase in stool water content.
We tend to use the term loosely (Ha! 😉) so your patient may be referring to another change in bowel habits when they say diarrhea.
How do we know?
The Bristol Stool Chart!
bit.ly/2TWeVgS
🙏🙏 @Dietitianbytes
We tend to use the term loosely (Ha! 😉) so your patient may be referring to another change in bowel habits when they say diarrhea.
How do we know?
The Bristol Stool Chart!
bit.ly/2TWeVgS
🙏🙏 @Dietitianbytes
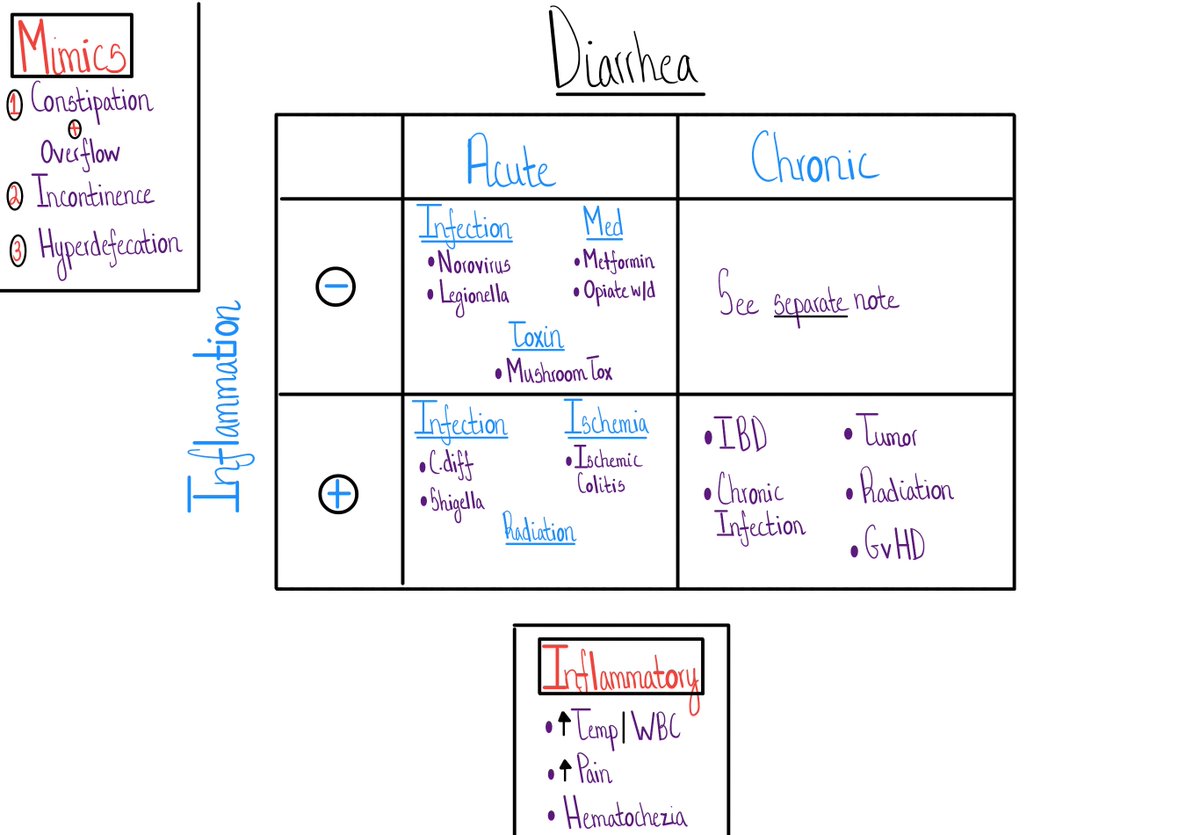
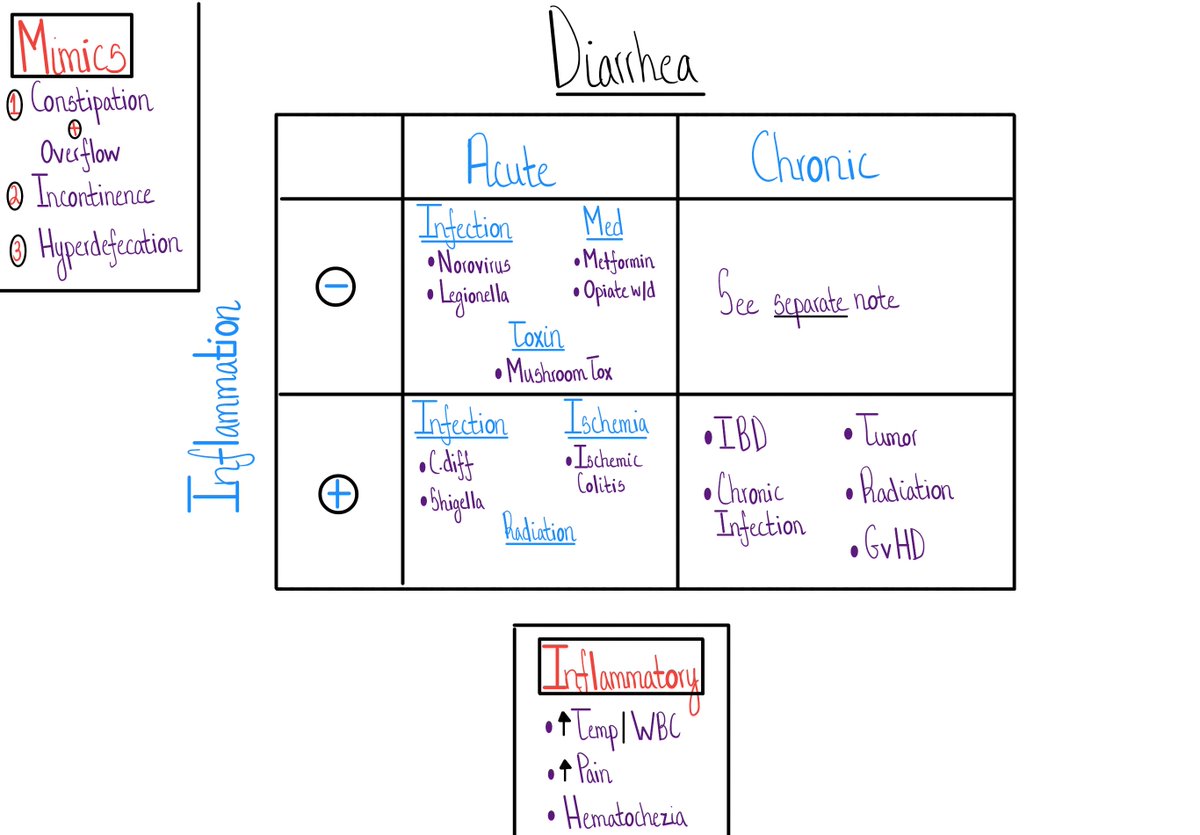
3 Misleading Mimics...
1. Constipation + overflow
2. Stool incontinence
3. Hyperdefecation
This amazing @COREIMpodcast case is a great example - bit.ly/332uDuR
I've been fooled by all 3...multiple times.
1. Constipation + overflow
2. Stool incontinence
3. Hyperdefecation
This amazing @COREIMpodcast case is a great example - bit.ly/332uDuR
I've been fooled by all 3...multiple times.

2 Key Questions...
If you are confident your patient has diarrhea, 2 pieces of data organize what is an incredibly long DDx.
1. Time course - acute (<2-4 weeks) or chronic (>2-4 wks)
2. Inflammation
If you are confident your patient has diarrhea, 2 pieces of data organize what is an incredibly long DDx.
1. Time course - acute (<2-4 weeks) or chronic (>2-4 wks)
2. Inflammation
How do we determine if there is inflammation?
I am so glad you asked!
Determining "inflammation" in general - bit.ly/2VXeky0
I am so glad you asked!
Determining "inflammation" in general - bit.ly/2VXeky0
For diarrhea, we usually have these 3 data points readily available.
There are other, more advanced, methods too, like the fecal calprotectin - bit.ly/38DW6UK
There are other, more advanced, methods too, like the fecal calprotectin - bit.ly/38DW6UK
So, after we've assessed for the 3 Misleading Mimics
and answered the 2 Key Questions, we end up with a 2x2 table
Let's chat about Acute Diarrhea
and answered the 2 Key Questions, we end up with a 2x2 table
Let's chat about Acute Diarrhea
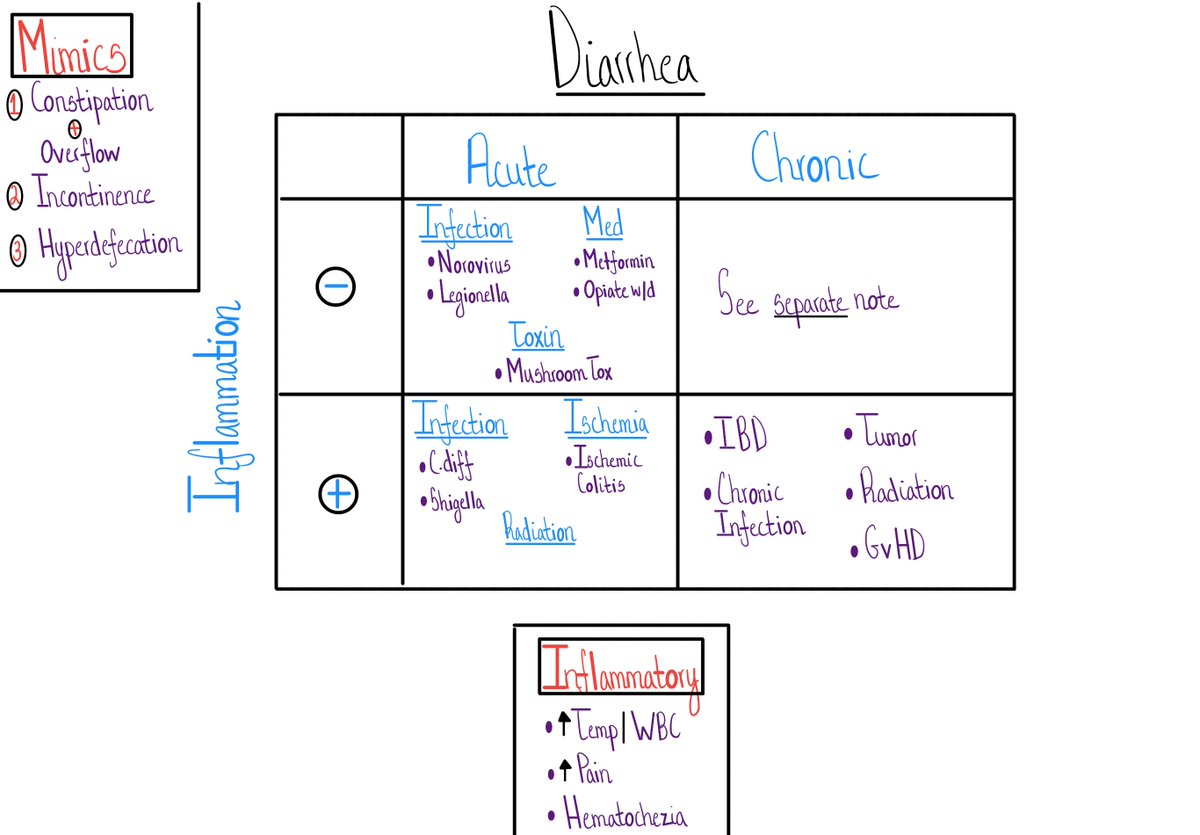
Acute Diarrhea...
Notice how we've simplified the mechanism from -
Osmotic, Secretory, Inflammatory
to
Non-inflammatory & Inflammatory.
Notice how we've simplified the mechanism from -
Osmotic, Secretory, Inflammatory
to
Non-inflammatory & Inflammatory.
Why?
The DDx of ACUTE diarrhea is limited enough, that the extra cognitive energy to classify as osmotic versus secretory isn't worth it.
Chronic diarrhea is a whole different equation.
We'll talk about that soon.
The DDx of ACUTE diarrhea is limited enough, that the extra cognitive energy to classify as osmotic versus secretory isn't worth it.
Chronic diarrhea is a whole different equation.
We'll talk about that soon.
Acute Non-Inflammatory Diarrhea
1. Infections
2. Meds
3. Toxins
1. Infections
2. Meds
3. Toxins

Y'all see Legionella up there?
Yes!
A reasonable # of extra-intestinal infections result in acute diarrhea
🤯🤯🤯
More here - go.nature.com/2Iz6nXI
Yes!
A reasonable # of extra-intestinal infections result in acute diarrhea
🤯🤯🤯
More here - go.nature.com/2Iz6nXI
Acute Inflammatory Diarrhea
1. Infection
2. Ischemia
3. Radiation
1. Infection
2. Ischemia
3. Radiation

Infections + acute diarrhea
Yup - infections make it on both lists - inflammatory and non-inflammatory acute diarrhea
We don't need a specific microbiologic Dx for most acute infectious diarrhea - a large # is viral - but key your eye out for:
Yup - infections make it on both lists - inflammatory and non-inflammatory acute diarrhea
We don't need a specific microbiologic Dx for most acute infectious diarrhea - a large # is viral - but key your eye out for:
1. C.diff!!
2. Traveler's diarrhea - a large fraction is bacterial
(the majority don't need antibiotics)
Great review from @adamcifu here - bit.ly/2TAtmIp
2. Traveler's diarrhea - a large fraction is bacterial
(the majority don't need antibiotics)
Great review from @adamcifu here - bit.ly/2TAtmIp
Alright friends, let's recap
1. Before you deploy a schema for diarrhea, consider the 3 Misleading Mimics.
2. Make the incredibly long DDx of diarrhea simpler by studying the 2 Key Variables - Time Course & Inflammation
1. Before you deploy a schema for diarrhea, consider the 3 Misleading Mimics.
2. Make the incredibly long DDx of diarrhea simpler by studying the 2 Key Variables - Time Course & Inflammation
3. Infections can lead to both a non-inflammatory and inflammatory acute diarrhea
4. Most patients with acute infectious diarrhea outside C.diff, don't need antibiotics.
4. Most patients with acute infectious diarrhea outside C.diff, don't need antibiotics.
Next time - we'll take on a tougher Dx problem - chronic non-inflammatory diarrhea
See ya then!
See ya then!