
Yesterday our #COVID-19 serology task force @MGHPathology hosted a meeting with labs around the country/world to share our results and to openly share ideas about platforms, validations, policy & implementation in our institutes & communities
#openscience
#allinthistogether
1/n
#openscience
#allinthistogether
1/n
We were joined by nearly 100 colleagues from >15 institutions – Mayo, Yale, Penn, BI, BCH, NYU, Mt. Sinai and others with of course many critical clinical colleagues from @MGHpathology and @MGHMedicine. It’s clear there are lots of smart people working on these needed tests!
In the spirit of #openscience and working together against #COVID-19, we are sharing our early results with hopes they help others rapidly role out assays in their own hospitals. We now have 2 assays we are confident in at MGH – a Point-of-Care Test and an ELISA. 1st – the POCT:
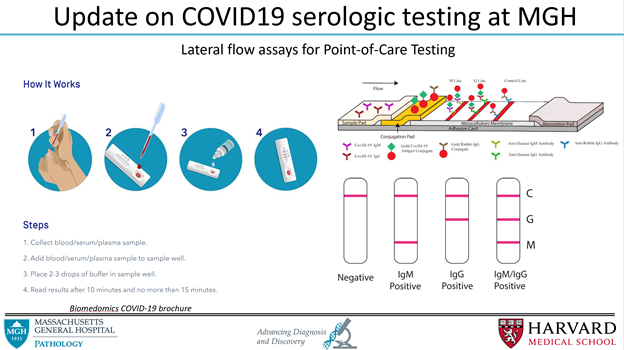
We tested commercially available kits & decided on an assay from BioMedomics to fully validate in-house. It’s looks like a pregnancy test & uses a drop of blood from your finger to tell if you have IgM or IgG antibodies against COVID-19. Available from @BioMedomics / @HenrySchein
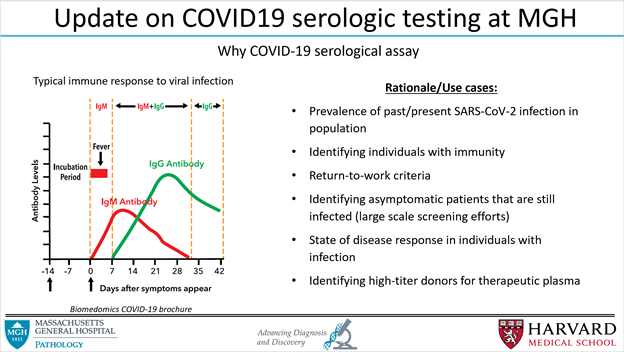
We used pre-COVID-19 outbreak samples as negatives & confirmed PCR-positive COVID-19 patients @ MGH. Your body takes time to create antibodies after the infection, so serological tests are only sensitive after about 7 days after onset of symptoms. Specific, and sensitive>7 days:
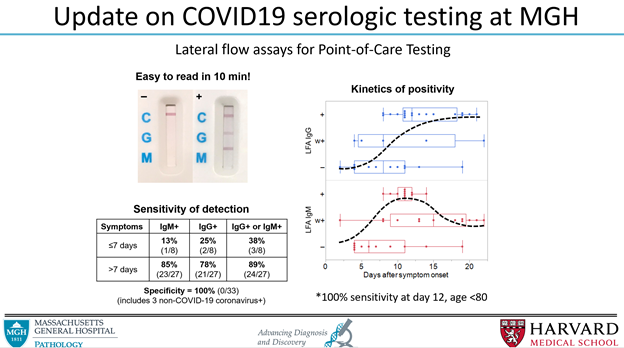
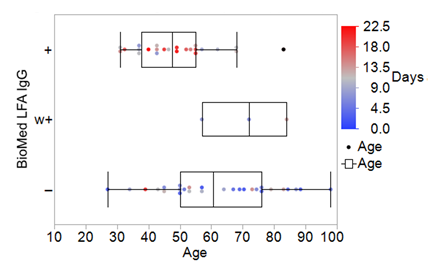
We also found age plays a role in the antibody response. The younger you were the quicker and more robust your antibody response was (young patient at later timepoint who was negative was on immunosuppressive therapy):
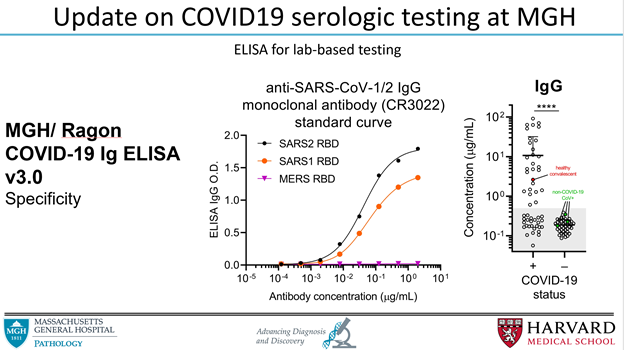
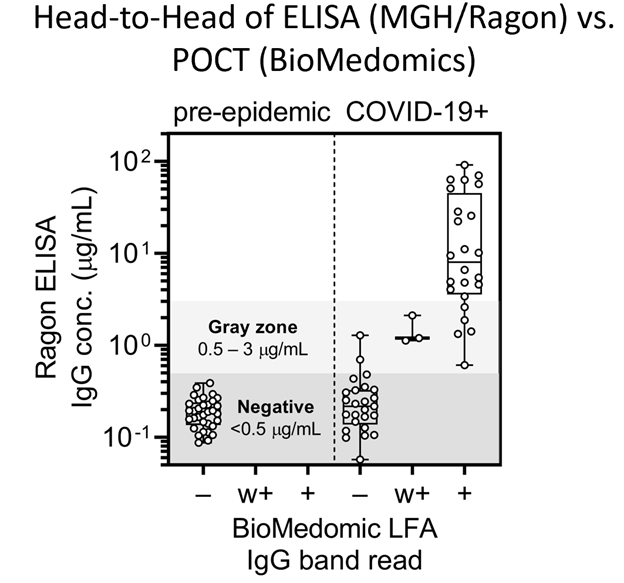
On to the next assay – ELISA. My co-Senior Clinical Pathology Resident Wilfredo Garcia Beltran is a brilliant immunologist. We tested a couple commercial assays, but they all were lacking in some way. So he collaborated with fantastic colleagues @ragoninstitute to create our own!
WGB and crew used the RBD antigen from SARS-CoV-2 as the bait (most specific recognized part of virus). Cool thing was they had a monoclonal antibody from SARS-CoV-1 that cross-reacted with SARS-CoV-2, so they could create a standard curve and titer IgG
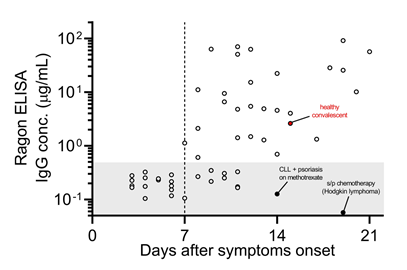
Viral titer correlated with day post-symptom onset. Interestingly, the 2 patients who did not have good responses past 10 days were immunosuppressed (would likely be the type of patients who would benefit most from convalescent pooled plasma transfusions).
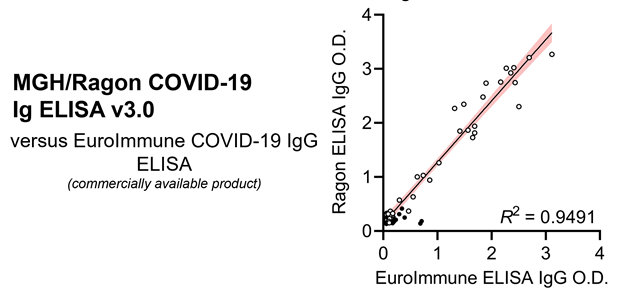
The in-house MGH/Ragon ELISA worked slightly better than even the best commercial assay we tested (slightly less background and wider dynamic range), but was largely concordant. (If you don't have capacity to make in-house ELISA, the EuroImmune assays worked well)
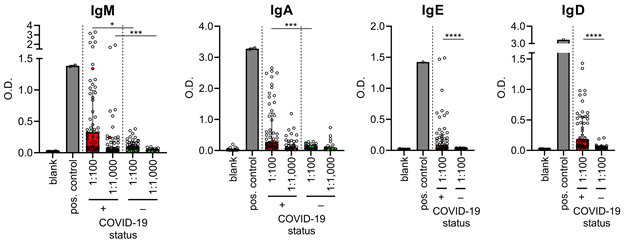
They didn’t stop there – they could detect all the other isotypes (pretty sure Wilfredo got these results around 4am one night/morning)
There was remarkable concordance between the ELISA and the POCT – these are both valuable assays to have and could fulfill different purposes. The POCT in the field as part of screening/surveillance, while using the ELISA to understand titer and track in-house patient responses
This is all really new data, some collected just over the last couple days. It will continue to evolve and I hope to continue to keep the community updated. Now, we need to finalize validation and figure out the best way to implement these assays into the clinic (not trivial)
As you can imagine, there are a huge number of people involved in this effort. There are so many pieces that go into launching a clinical assay, much of it behind the scenes (training, EPIC integration, clinical workflow, etc, etc). Normally >3-6 months: it happened in 2 weeks.
Huge shout-out to John Iafrate who has been leading the task force, Joe, Hetal, Lauren & the CID-team for providing the infrastructure, effort, & know-how to launch an assay in 2 weeks, & the many people below who worked round the clock (literally) to make this happen #MGHStrong
Also a big shout-out to my research mentor @bradbernstein who came to me ~3 weeks ago saying we need a serology assay, we should help (even though we do cancer epigenetic research). We are both CP-trained, wanted to contribute to the cause, sent some emails, and now here we are…
Last, and most importantly, thank you to my wife and kids, and to all the other families who have put up with not having us around to help at home through a very stressful time. None of us could do this without their support at home 💕











