1/
Patients with iron deficiency anemia generally dislike taking oral iron (nausea, constipation) and often stop taking iron tablets.
Does the way we prescribe ferrous sulfate contribute to this?
Read on to find out.
Patients with iron deficiency anemia generally dislike taking oral iron (nausea, constipation) and often stop taking iron tablets.
Does the way we prescribe ferrous sulfate contribute to this?
Read on to find out.
2/
For decades, the teaching has been to replace iron with oral ferrous sulfate 325 mg thrice a day. Each 325 mg tablet contains 65 mg elemental iron, so TID dosing delivers 195 mg elemental iron to the gut.
Of this, only around 15% (25 mg) is absorbed.
For decades, the teaching has been to replace iron with oral ferrous sulfate 325 mg thrice a day. Each 325 mg tablet contains 65 mg elemental iron, so TID dosing delivers 195 mg elemental iron to the gut.
Of this, only around 15% (25 mg) is absorbed.
3/
This 25 mg of iron a day usually produces an improvement in Hb of 1 gm/dL in approximately 10 days.
Ideally one should see a 2 gm increase in Hb over 3-4 weeks when treating iron deficiency anemia.
This 25 mg of iron a day usually produces an improvement in Hb of 1 gm/dL in approximately 10 days.
Ideally one should see a 2 gm increase in Hb over 3-4 weeks when treating iron deficiency anemia.
4/
The unabsorbed iron in the gut (195 mg minus 25 mg= 170 mg) is free to cause hara-kiri.
Unabsorbed iron --> dysbiosis + reactive iron species--> GI side effects.
The unabsorbed iron in the gut (195 mg minus 25 mg= 170 mg) is free to cause hara-kiri.
Unabsorbed iron --> dysbiosis + reactive iron species--> GI side effects.
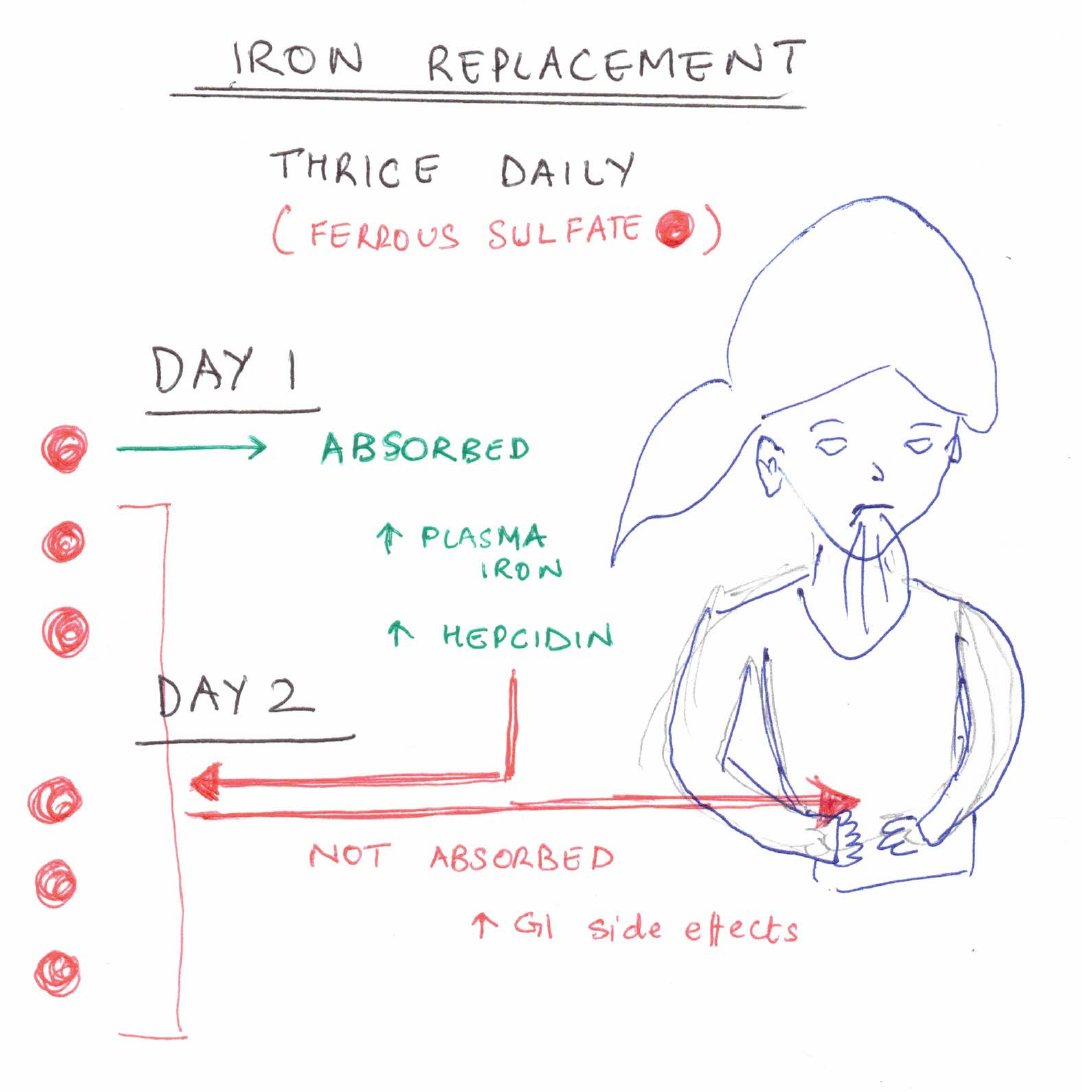
5/
But why is iron absorption so inefficient? If the body is iron-deficient, it should try to lap up every drop of available iron.
The answer is hepcidin. High circulating iron is toxic and promotes microbial growth, so the body tries to limit sudden increases in plasma iron.
But why is iron absorption so inefficient? If the body is iron-deficient, it should try to lap up every drop of available iron.
The answer is hepcidin. High circulating iron is toxic and promotes microbial growth, so the body tries to limit sudden increases in plasma iron.
6/
PO iron-> absorption -> ↑ plasma iron-> ↑ hepcidin-> impaired further iron absorption (up to 48 hours).
Thus after an iron load, the body cannot absorb iron well for up to 2 days. Further doses the same of next day will not be absorbed, but will cause side effects.
PO iron-> absorption -> ↑ plasma iron-> ↑ hepcidin-> impaired further iron absorption (up to 48 hours).
Thus after an iron load, the body cannot absorb iron well for up to 2 days. Further doses the same of next day will not be absorbed, but will cause side effects.
7/
Absorption efficiency has been shown to be best for approximately 60 mg of iron (1 tablet ferrous sulfate) at a MAXIMUM OF ONCE A DAY.
One trial demonstrated increased absorption of iron and lower nausea with ALTERNATIVE DAY ferrous sulfate vs. daily dosing.
Absorption efficiency has been shown to be best for approximately 60 mg of iron (1 tablet ferrous sulfate) at a MAXIMUM OF ONCE A DAY.
One trial demonstrated increased absorption of iron and lower nausea with ALTERNATIVE DAY ferrous sulfate vs. daily dosing.
8/
More and more hematologists now recommend 1 table of ferrous sulfate 325 mg on alternate days, or a Monday-Wednesday-Friday schedule for treating iron deficiency.
More and more hematologists now recommend 1 table of ferrous sulfate 325 mg on alternate days, or a Monday-Wednesday-Friday schedule for treating iron deficiency.
9/
This will achieve the primary aim of repleting iron, and also reduce side effects, and inappropriate labeling of ‘PO failure’ and unnecessary switch to IV iron.
Further trials in the works, hope guidelines soon emerge.
This will achieve the primary aim of repleting iron, and also reduce side effects, and inappropriate labeling of ‘PO failure’ and unnecessary switch to IV iron.
Further trials in the works, hope guidelines soon emerge.