1/
It’s time for a #tweetorial on hypersensitivity pneumonitis. It’s a greatly misunderstood entity. Potentially treatable, so can be very good news. OTOH, misdiagnosing UIP as chronic hypersensitivity pneumonitis can be very bad.
Follow this thread for a #pathtweetorial
It’s time for a #tweetorial on hypersensitivity pneumonitis. It’s a greatly misunderstood entity. Potentially treatable, so can be very good news. OTOH, misdiagnosing UIP as chronic hypersensitivity pneumonitis can be very bad.
Follow this thread for a #pathtweetorial
2/
Let’s start with a poll regarding a common misconception. What is the predominant inflammatory cell in hypersensitivity pneumonitis?
Let’s start with a poll regarding a common misconception. What is the predominant inflammatory cell in hypersensitivity pneumonitis?
3/
Hypersensitivity pneumonitis is an inflammatory reaction that occurs in individuals (classically never-smokers) who are exquisitely sensitive to an organic antigen.
Obvious exposures (moldy hay=farmer’s lung) can be fairly straightforward to recognize clinically.
Hypersensitivity pneumonitis is an inflammatory reaction that occurs in individuals (classically never-smokers) who are exquisitely sensitive to an organic antigen.
Obvious exposures (moldy hay=farmer’s lung) can be fairly straightforward to recognize clinically.
4/
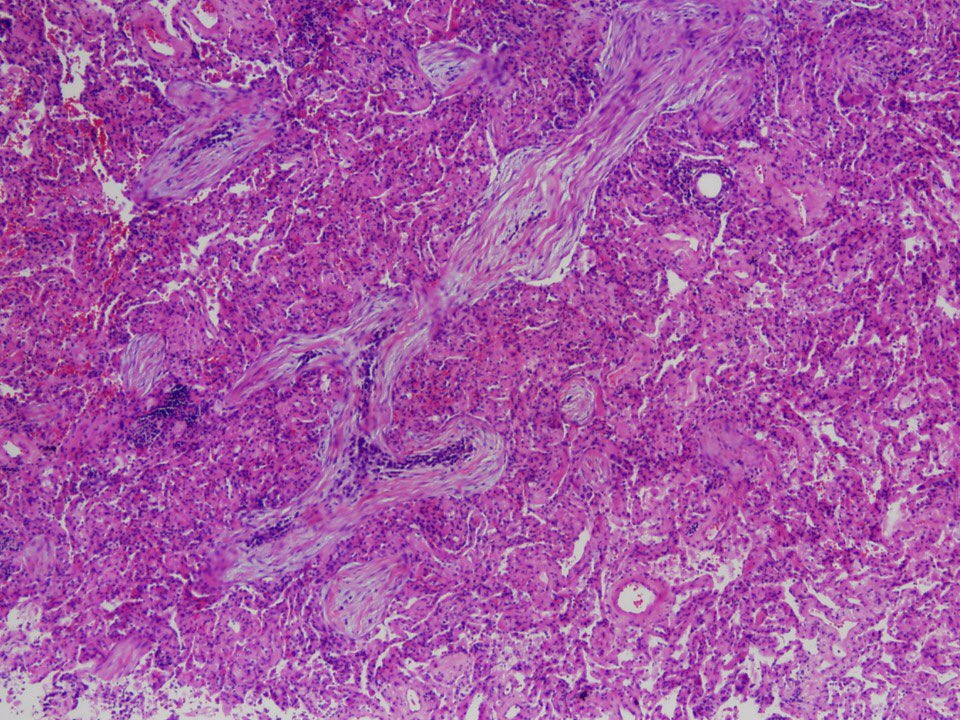
The pathologic inflammatory response involves mainly lymphocytes in the interstitium. Hypersensitivity pneumonitis is therefore a form of interstitial lung disease.
Interstitial thickening is usually mild and subtle.
The pathologic inflammatory response involves mainly lymphocytes in the interstitium. Hypersensitivity pneumonitis is therefore a form of interstitial lung disease.
Interstitial thickening is usually mild and subtle.

5/
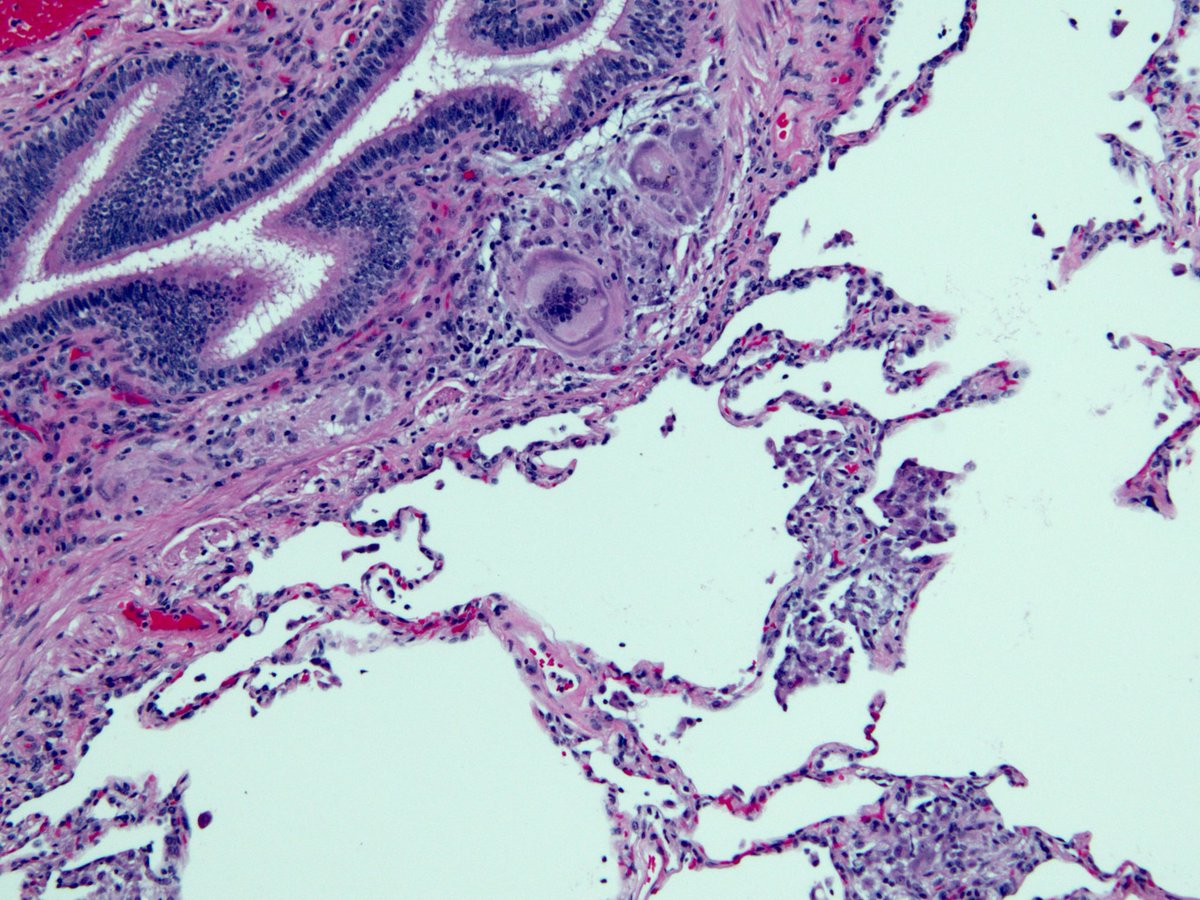
Bronchioles are inflamed too (chronic bronchiolitis). The antigen enters through the airways, after all.
Along with lymphocytes, there are often mutinucleated giant cells. The appearance shown below is not specific. You can see this in sarcoidosis and NTM infection.
Bronchioles are inflamed too (chronic bronchiolitis). The antigen enters through the airways, after all.
Along with lymphocytes, there are often mutinucleated giant cells. The appearance shown below is not specific. You can see this in sarcoidosis and NTM infection.

6/
Let’s recap:
Chronic bronchiolitis + interstitial lymphocyte infiltrate + occasional giant cells.
Read more about the #pathology of this disease here:
emedicine.medscape.com/article/207843…
Let’s recap:
Chronic bronchiolitis + interstitial lymphocyte infiltrate + occasional giant cells.
Read more about the #pathology of this disease here:
emedicine.medscape.com/article/207843…
7/
Giant cells are often seen in the interstitium where bronchioles transition into alveoli...respiratory bronchioles and alveolar ducts.
Giant cells are often seen in the interstitium where bronchioles transition into alveoli...respiratory bronchioles and alveolar ducts.

8/
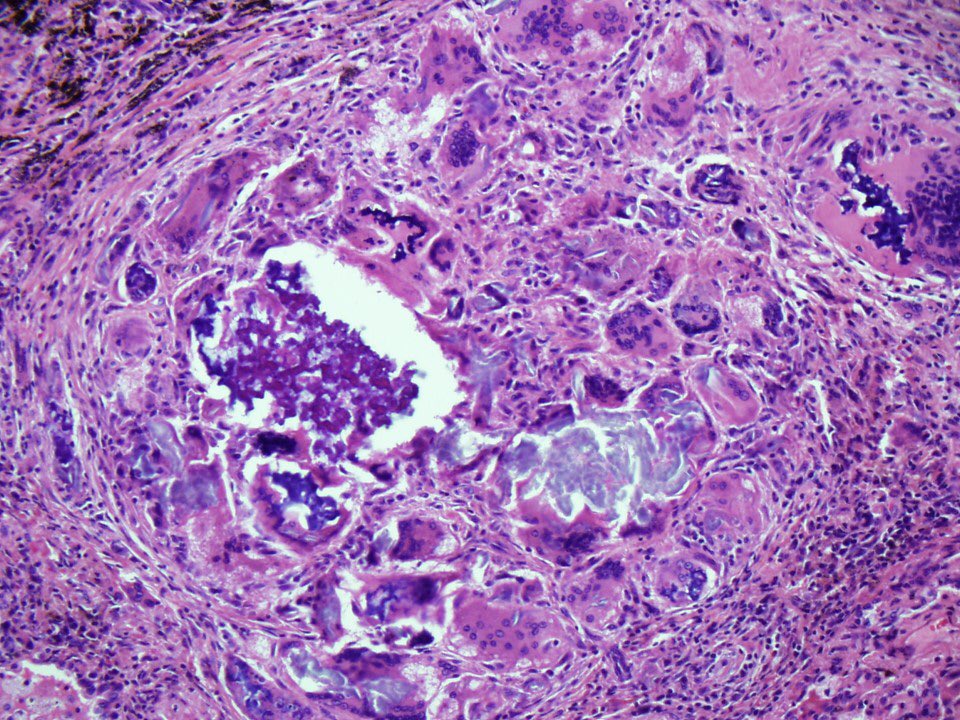
When granulomas form, they are usually small and difficult to see, at least at low mag. They are histiocytes grouped loosely into an aggregate.
When granulomas form, they are usually small and difficult to see, at least at low mag. They are histiocytes grouped loosely into an aggregate.

9/
If you want to see a video with a detailed discussion of the pathologic findings in hypersensitivity pneumonitis, check out this YouTube video I made:
#pathology #pulmpath
If you want to see a video with a detailed discussion of the pathologic findings in hypersensitivity pneumonitis, check out this YouTube video I made:
#pathology #pulmpath
10/
Eosinophils are NOT a feature of hypersensitivity pneumonitis. Most cases don’t have ANY!
Lymphocytes ✅✅✅✅
Eosinophils ❌❌❌❌
In terms of the inflammatory response, hypersensitivity pneumonitis is more like TB (type 4) than asthma (type 1)
Eosinophils are NOT a feature of hypersensitivity pneumonitis. Most cases don’t have ANY!
Lymphocytes ✅✅✅✅
Eosinophils ❌❌❌❌
In terms of the inflammatory response, hypersensitivity pneumonitis is more like TB (type 4) than asthma (type 1)
11/
Let’s summarize the textbook case of hypersensitivity pneumonitis (4-legged table):
1. Clinical: never smoker, episodic worsening
2. Exposure: pet birds, etc
3. Imaging: bilateral GGO, mosaic, air trapping
4. Path: lymphocytes in interstitium, giant cells, bronchiolitis
Let’s summarize the textbook case of hypersensitivity pneumonitis (4-legged table):
1. Clinical: never smoker, episodic worsening
2. Exposure: pet birds, etc
3. Imaging: bilateral GGO, mosaic, air trapping
4. Path: lymphocytes in interstitium, giant cells, bronchiolitis

12/
What if no exposure can be found? This scenario is actually VERY common in biopsy-proven hypersensitivity pneumonitis, probably much higher than 50%.
But if never-smoker, classic imaging and classic path, this 3-legged table can still stand.
What if no exposure can be found? This scenario is actually VERY common in biopsy-proven hypersensitivity pneumonitis, probably much higher than 50%.
But if never-smoker, classic imaging and classic path, this 3-legged table can still stand.

13/
Let’s examine the imaging, since that’s the leg that clinicians rely so heavily on.
Remember, we are talking about “subacute” hypersensitivity pneumonitis, the least controversial form. Here an expert radiologist describes the “head cheese sign”
Let’s examine the imaging, since that’s the leg that clinicians rely so heavily on.
Remember, we are talking about “subacute” hypersensitivity pneumonitis, the least controversial form. Here an expert radiologist describes the “head cheese sign”
14/
By the way, head cheese isn’t cheese at all...you know, the kind that comes from dairy/milk.
Head cheese is a potpourri of meat, or “meat jelly” (image from Wikimedia commons)
I guess pathologists are not the only ones who like food analogies. 😰🤢
By the way, head cheese isn’t cheese at all...you know, the kind that comes from dairy/milk.
Head cheese is a potpourri of meat, or “meat jelly” (image from Wikimedia commons)
I guess pathologists are not the only ones who like food analogies. 😰🤢

15/
Agreement goes out the window when it comes to “chronic hypersensitivity pneumonitis”, an entity in which fibrosis allegedly develops and progresses to an appearance very similar to UIP/IPF. Most of these cases behave very badly (like UIP).
So what makes them HP? Read on..
Agreement goes out the window when it comes to “chronic hypersensitivity pneumonitis”, an entity in which fibrosis allegedly develops and progresses to an appearance very similar to UIP/IPF. Most of these cases behave very badly (like UIP).
So what makes them HP? Read on..
16/
Often, this diagnosis is based heavily on “air trapping” on HRCT. This is truly a one legged table, resting solely on imaging. Can air trapping occur in UIP/IPF?
Answer: Yes!
This study by Sverzellati et al is a must-read:
pubs.rsna.org/doi/full/10.11…
Often, this diagnosis is based heavily on “air trapping” on HRCT. This is truly a one legged table, resting solely on imaging. Can air trapping occur in UIP/IPF?
Answer: Yes!
This study by Sverzellati et al is a must-read:
pubs.rsna.org/doi/full/10.11…
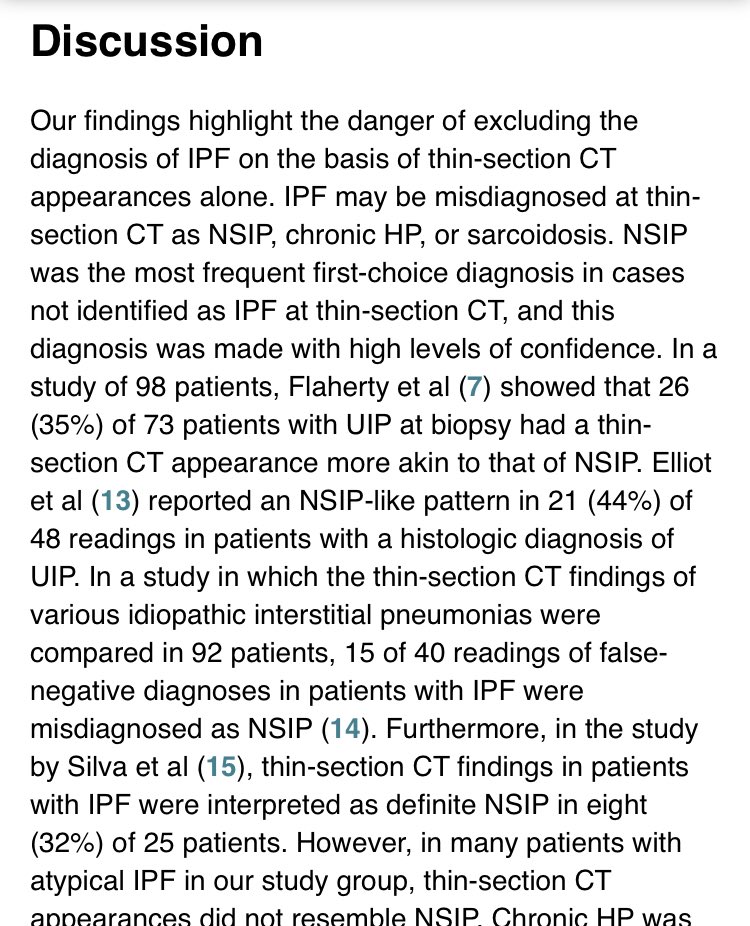
17/
The Sverzellati study is shocking, but only if you believe that air trapping on HRCT is specific for hypersensitivity pneumonitis. The study provides examples of CT scans from biopsy-proven IPF that were read as hypersensitivity with high degree of confidence.
The Sverzellati study is shocking, but only if you believe that air trapping on HRCT is specific for hypersensitivity pneumonitis. The study provides examples of CT scans from biopsy-proven IPF that were read as hypersensitivity with high degree of confidence.
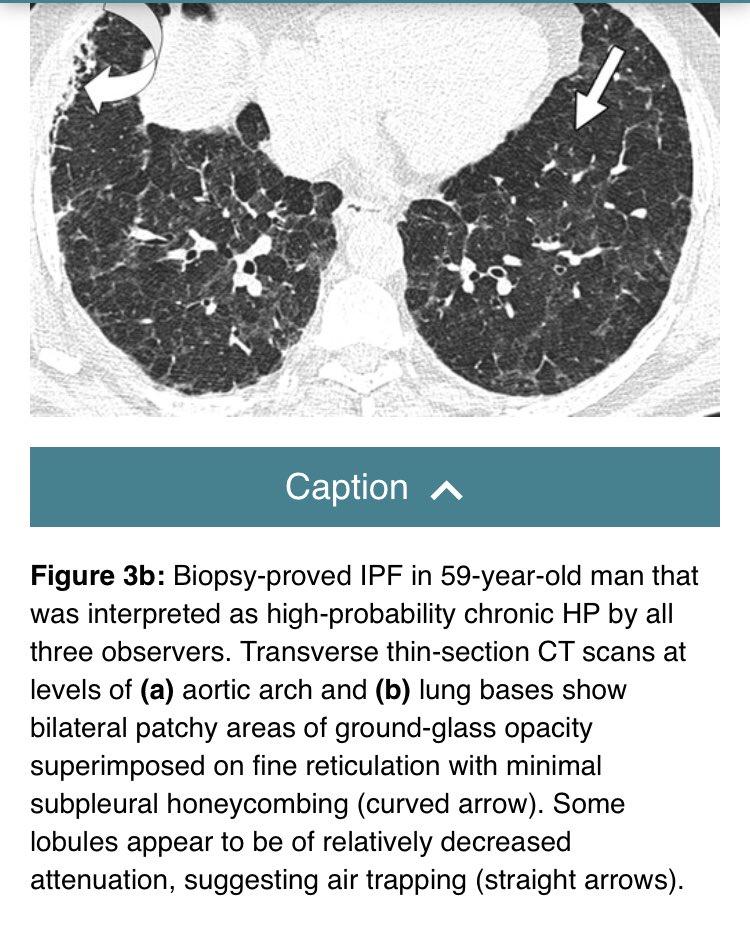

18/
If it walks like a 🦆 and quacks like a 🦆 it’s a 🦆, right?
The chronic HP camp says no. It looks like UIP and behaves like UIP. No exposure. Smokers. Elderly men. But air trapping makes it HP.
I don’t buy this argument. I think most of these are UIP/IPF.
If it walks like a 🦆 and quacks like a 🦆 it’s a 🦆, right?
The chronic HP camp says no. It looks like UIP and behaves like UIP. No exposure. Smokers. Elderly men. But air trapping makes it HP.
I don’t buy this argument. I think most of these are UIP/IPF.
19/
I’m willing to buy chronic HP if the patient is a bird fancier and/or pathology is classic for HP in non fibrotic areas of the lung
But UIP doesn’t become HP just because of:
🔴 a few granulomas
🔴 chronic inflammation
🔴 “airway centered fibrosis”
🔴 air trapping
I’m willing to buy chronic HP if the patient is a bird fancier and/or pathology is classic for HP in non fibrotic areas of the lung
But UIP doesn’t become HP just because of:
🔴 a few granulomas
🔴 chronic inflammation
🔴 “airway centered fibrosis”
🔴 air trapping
20/
Optimal Rx of hypersensitivity pneumonitis: identify the source of exposure and get the patient away from it.
The next time you see a dyspneic never smoker with bilateral GGO and the head cheese sign on HRCT, ask them if they have pet birds.
🔴 End of #Tweetorial 🔴
Optimal Rx of hypersensitivity pneumonitis: identify the source of exposure and get the patient away from it.
The next time you see a dyspneic never smoker with bilateral GGO and the head cheese sign on HRCT, ask them if they have pet birds.
🔴 End of #Tweetorial 🔴