,
16 tweets,
6 min read
Read on Twitter
1/
How do steroids cause an increase in the white blood cell (WBC) count (i.e., leukocytosis)?
And, how do steroids tamp down inflammation if it appears that there are more WBCs in the blood after they are administered?
Seems like a paradox in need of a thread.
How do steroids cause an increase in the white blood cell (WBC) count (i.e., leukocytosis)?
And, how do steroids tamp down inflammation if it appears that there are more WBCs in the blood after they are administered?
Seems like a paradox in need of a thread.
2/
We've known for decades that the leukocytosis observed after the administration of steroids results from an increase in the neutrophil count.
Which of the following is the largest contributor to this post-steroid leukocytosis/neutrophilia?
[BM = bone marrow]
We've known for decades that the leukocytosis observed after the administration of steroids results from an increase in the neutrophil count.
Which of the following is the largest contributor to this post-steroid leukocytosis/neutrophilia?
[BM = bone marrow]
3/
The first three mechanisms all play a role.
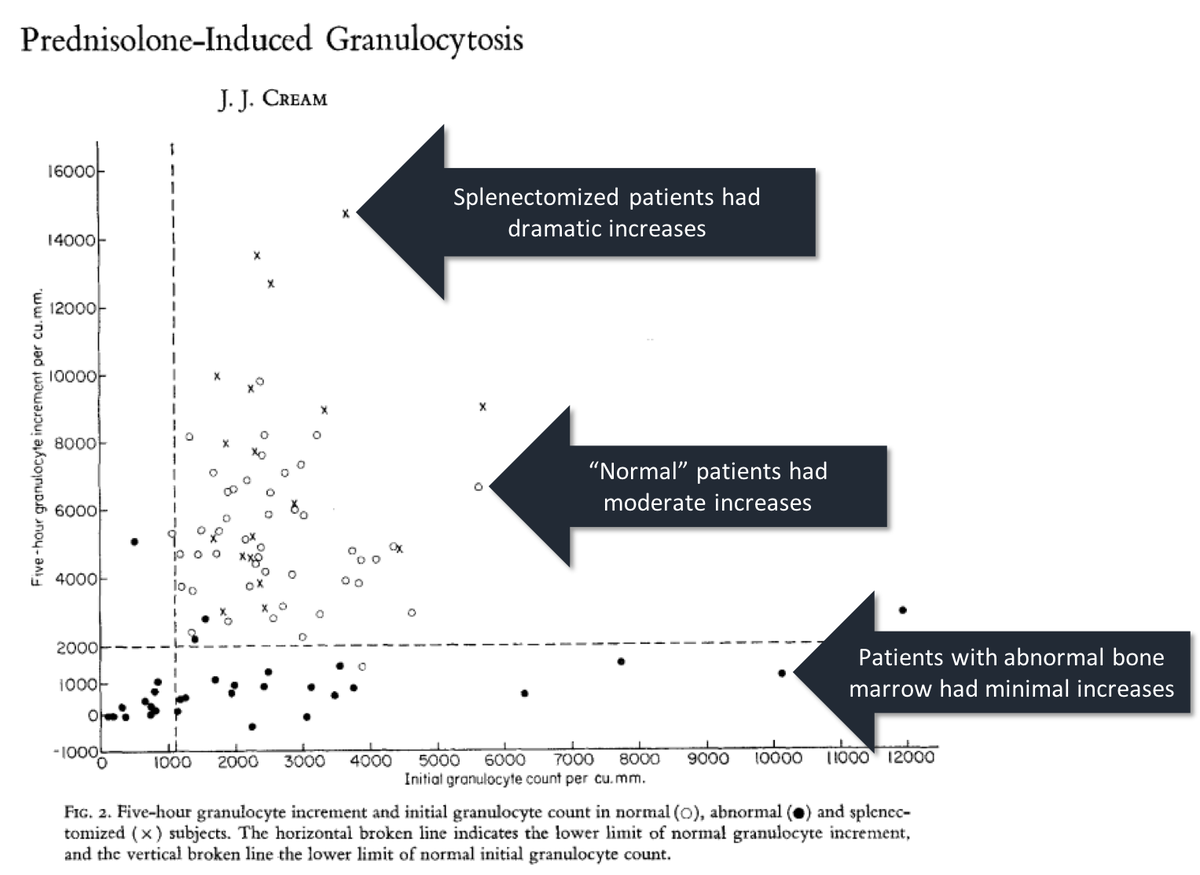
In the 1960s, many felt that an influx from the bone marrow was most responsible. One clue supporting this mechanism: patients with abnormal marrows show decreased post-steroid leukocytosis.
ncbi.nlm.nih.gov/pubmed/5681482
The first three mechanisms all play a role.
In the 1960s, many felt that an influx from the bone marrow was most responsible. One clue supporting this mechanism: patients with abnormal marrows show decreased post-steroid leukocytosis.
ncbi.nlm.nih.gov/pubmed/5681482
4/
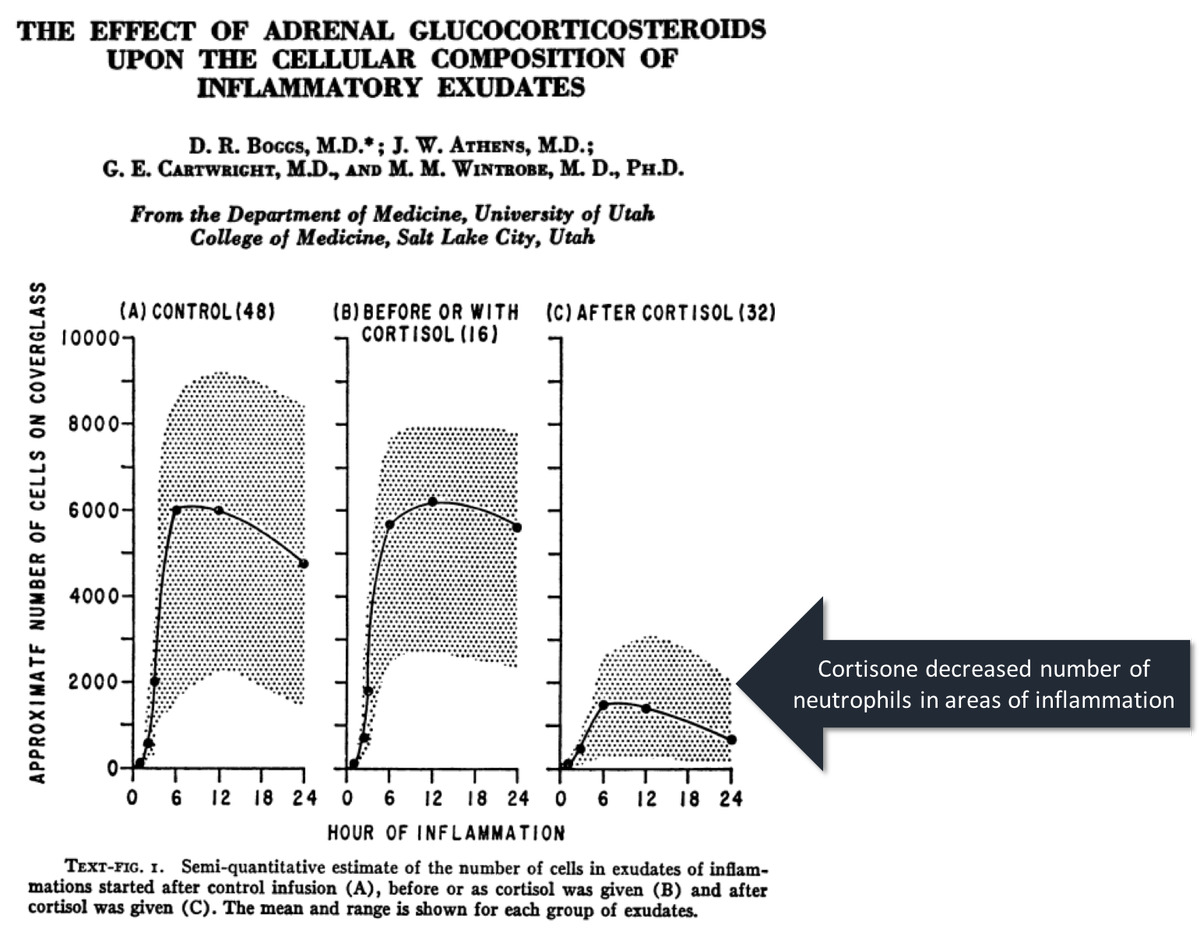
If marrow influx were the only cause, inflammation would INCREASE with steroids. (Add more neutrophils and you should increase inflammation.)
But studies clearly show that the number of neutrophils in areas of inflammation DECREASE with steroids.
ncbi.nlm.nih.gov/pubmed/14155024
If marrow influx were the only cause, inflammation would INCREASE with steroids. (Add more neutrophils and you should increase inflammation.)
But studies clearly show that the number of neutrophils in areas of inflammation DECREASE with steroids.
ncbi.nlm.nih.gov/pubmed/14155024
5/
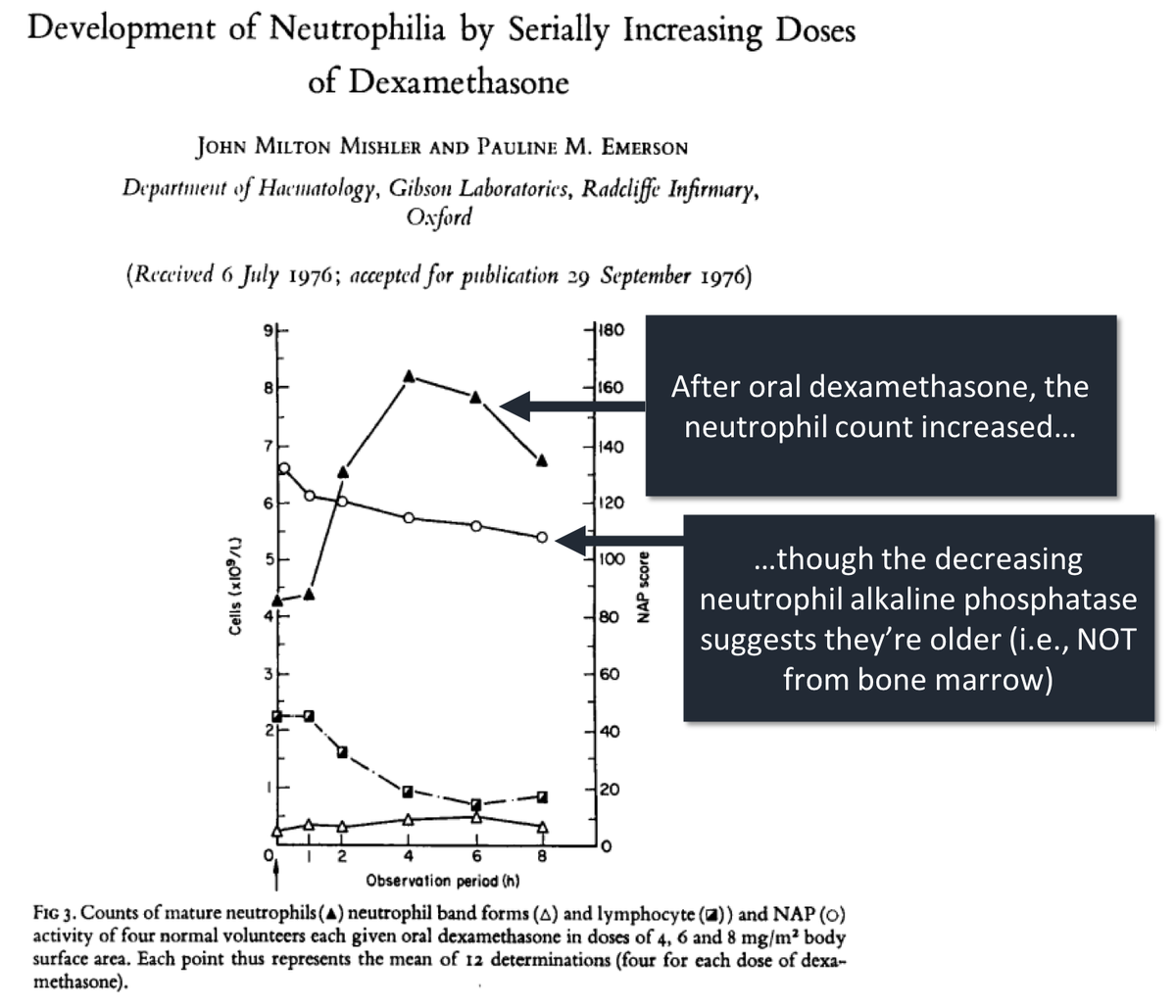
Another clue that increased bone marrow production isn't the predominant mechanism: the neutrophils seen after steroids are "old".
This conclusion is based on decreased neutrophil alkaline phosphatase (NAP) level after steroids administration.
ncbi.nlm.nih.gov/pubmed/871436
Another clue that increased bone marrow production isn't the predominant mechanism: the neutrophils seen after steroids are "old".
This conclusion is based on decreased neutrophil alkaline phosphatase (NAP) level after steroids administration.
ncbi.nlm.nih.gov/pubmed/871436
6/
More recent data suggests the following contributions to post-steroid leukocytosis:
*mobilization from marginated pool - 61%
*delayed apoptosis - 29%
*increased bone marrow production - 10%
ncbi.nlm.nih.gov/pubmed/9826319
More recent data suggests the following contributions to post-steroid leukocytosis:
*mobilization from marginated pool - 61%
*delayed apoptosis - 29%
*increased bone marrow production - 10%
ncbi.nlm.nih.gov/pubmed/9826319
7/
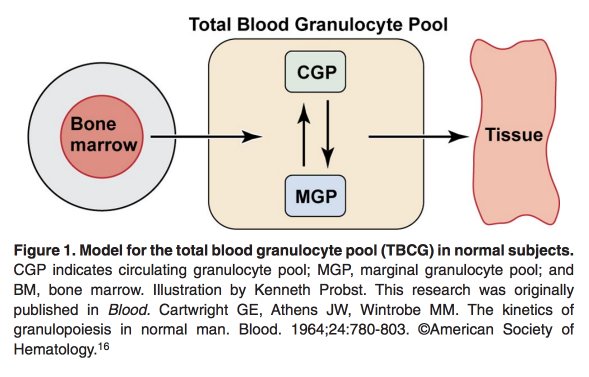
More than half of the leukocytosis results from "demargination". To understand this mechanism, recall that there are two pools of neutrophils within the circulation:
*circulating
*marginated
ncbi.nlm.nih.gov/pubmed/18684880
More than half of the leukocytosis results from "demargination". To understand this mechanism, recall that there are two pools of neutrophils within the circulation:
*circulating
*marginated
ncbi.nlm.nih.gov/pubmed/18684880
8/
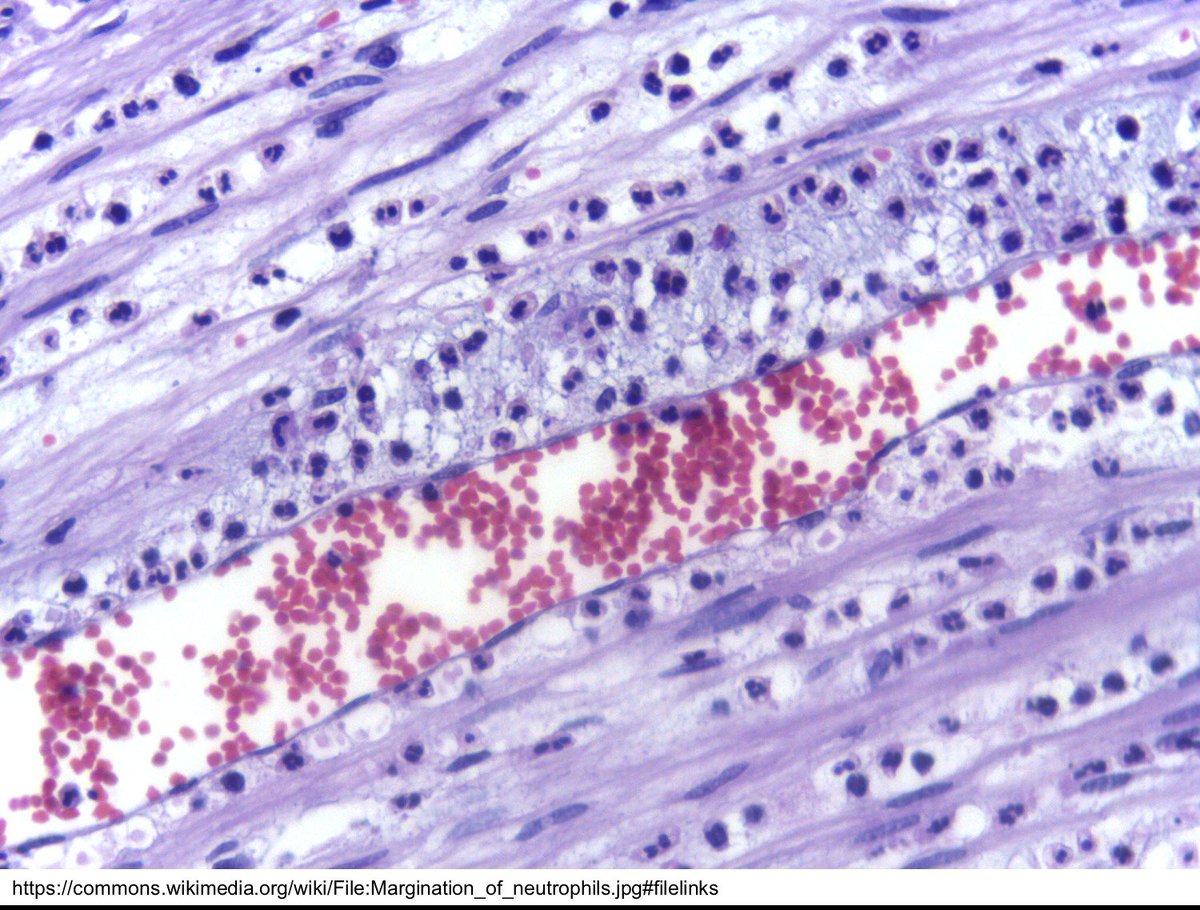
The marginated pool includes neutrophils that adhere to the endothelium of capillaries and postcapillary venules.
Areas rich in marginated neutrophils include the lungs, liver, and spleen.
The marginated pool includes neutrophils that adhere to the endothelium of capillaries and postcapillary venules.
Areas rich in marginated neutrophils include the lungs, liver, and spleen.
9/
It's important to realize that when we order a white blood cell count, we do NOT "see" the marginated neutrophils on the report. We only see the circulating neutrophils.
So, a question: What fraction of neutrophils are circulating (C) versus marginated (M)?
It's important to realize that when we order a white blood cell count, we do NOT "see" the marginated neutrophils on the report. We only see the circulating neutrophils.
So, a question: What fraction of neutrophils are circulating (C) versus marginated (M)?
10/
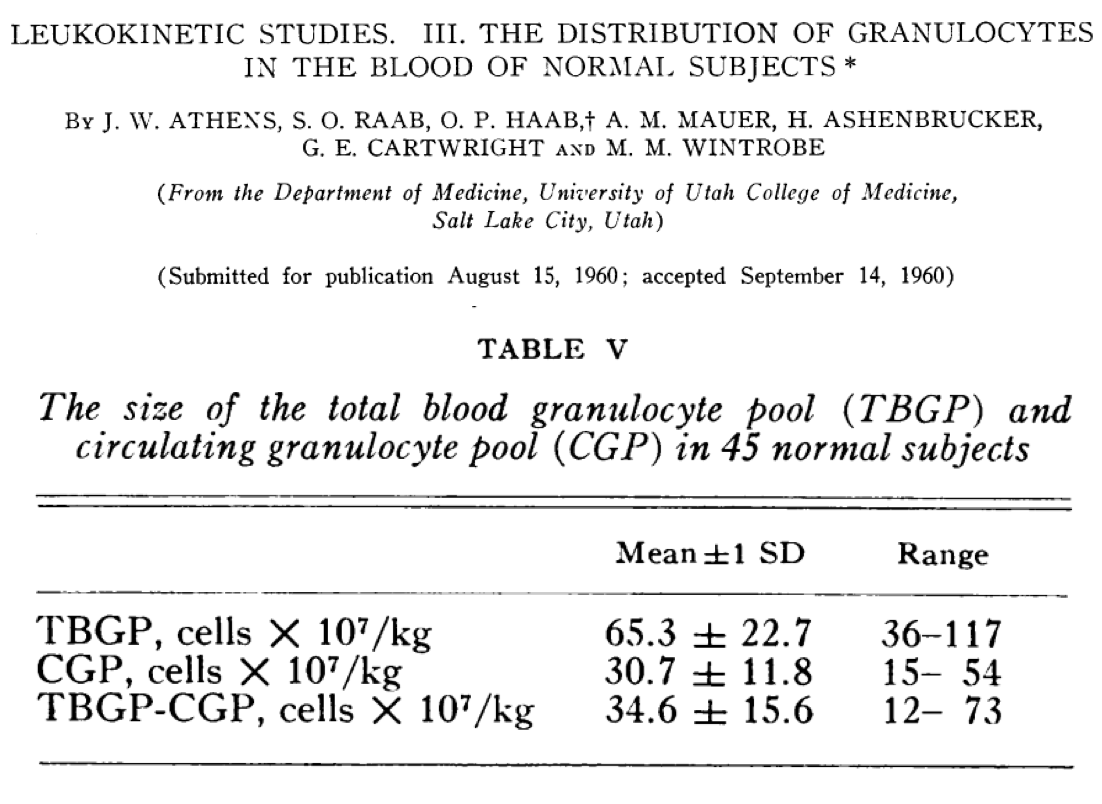
Approximately HALF of the neutrophils in the "circulation" aren't circulating (i.e., they're marginated)! This was demonstrated in 1961 in a study using radiolabeled neutrophils.
ncbi.nlm.nih.gov/pubmed/13684959
Approximately HALF of the neutrophils in the "circulation" aren't circulating (i.e., they're marginated)! This was demonstrated in 1961 in a study using radiolabeled neutrophils.
ncbi.nlm.nih.gov/pubmed/13684959
11/
So, there certainly is a large pool of marginated neutrophils ready to contribute to post-steroid leukocytosis.
But, what do steroids "do" that moves neutrophils from the marginated pool to the circulating pool?
So, there certainly is a large pool of marginated neutrophils ready to contribute to post-steroid leukocytosis.
But, what do steroids "do" that moves neutrophils from the marginated pool to the circulating pool?
12/
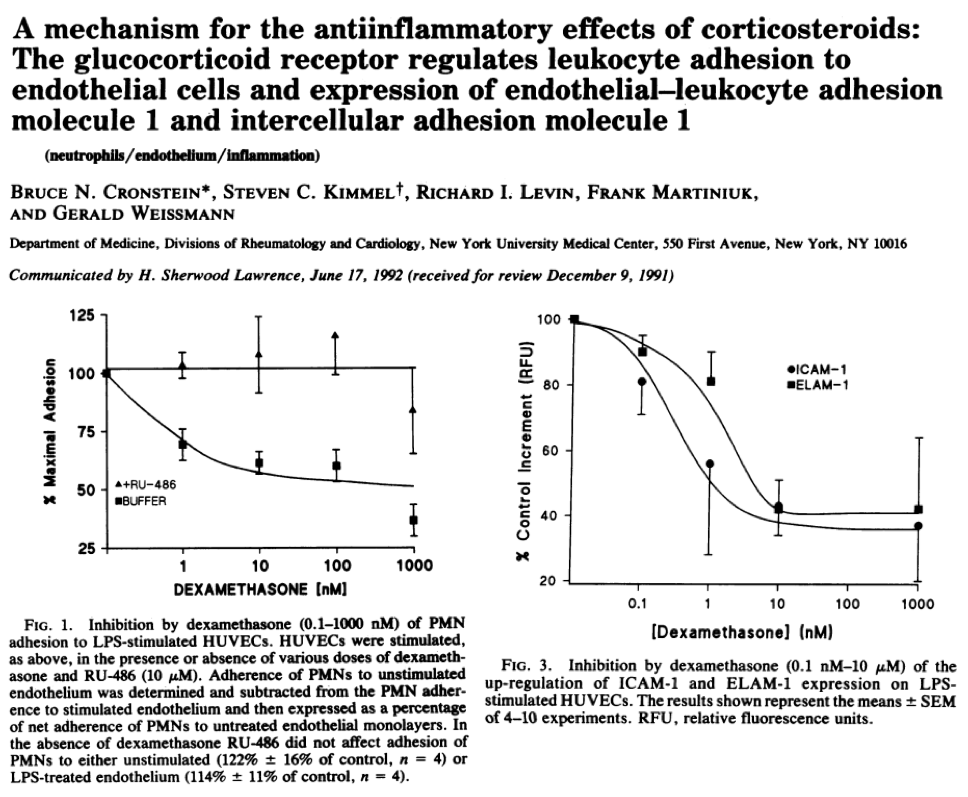
In 1992, Cronstein showed that steroids inhibit ICAM-1 and ELAM-1 expression. Without these adhesion molecules neutrophils:
*don't leave the vascular space ➡️ decreased inflammation
*do move from marginated pool to circulating pool ➡️ leukocytosis!
ncbi.nlm.nih.gov/pubmed/1279685
In 1992, Cronstein showed that steroids inhibit ICAM-1 and ELAM-1 expression. Without these adhesion molecules neutrophils:
*don't leave the vascular space ➡️ decreased inflammation
*do move from marginated pool to circulating pool ➡️ leukocytosis!
ncbi.nlm.nih.gov/pubmed/1279685
13/
Based on the above, which of the following might also cause leukocytosis via demargination (i.e., movement from the marginated pool to the circulating pool)?
Based on the above, which of the following might also cause leukocytosis via demargination (i.e., movement from the marginated pool to the circulating pool)?
14/
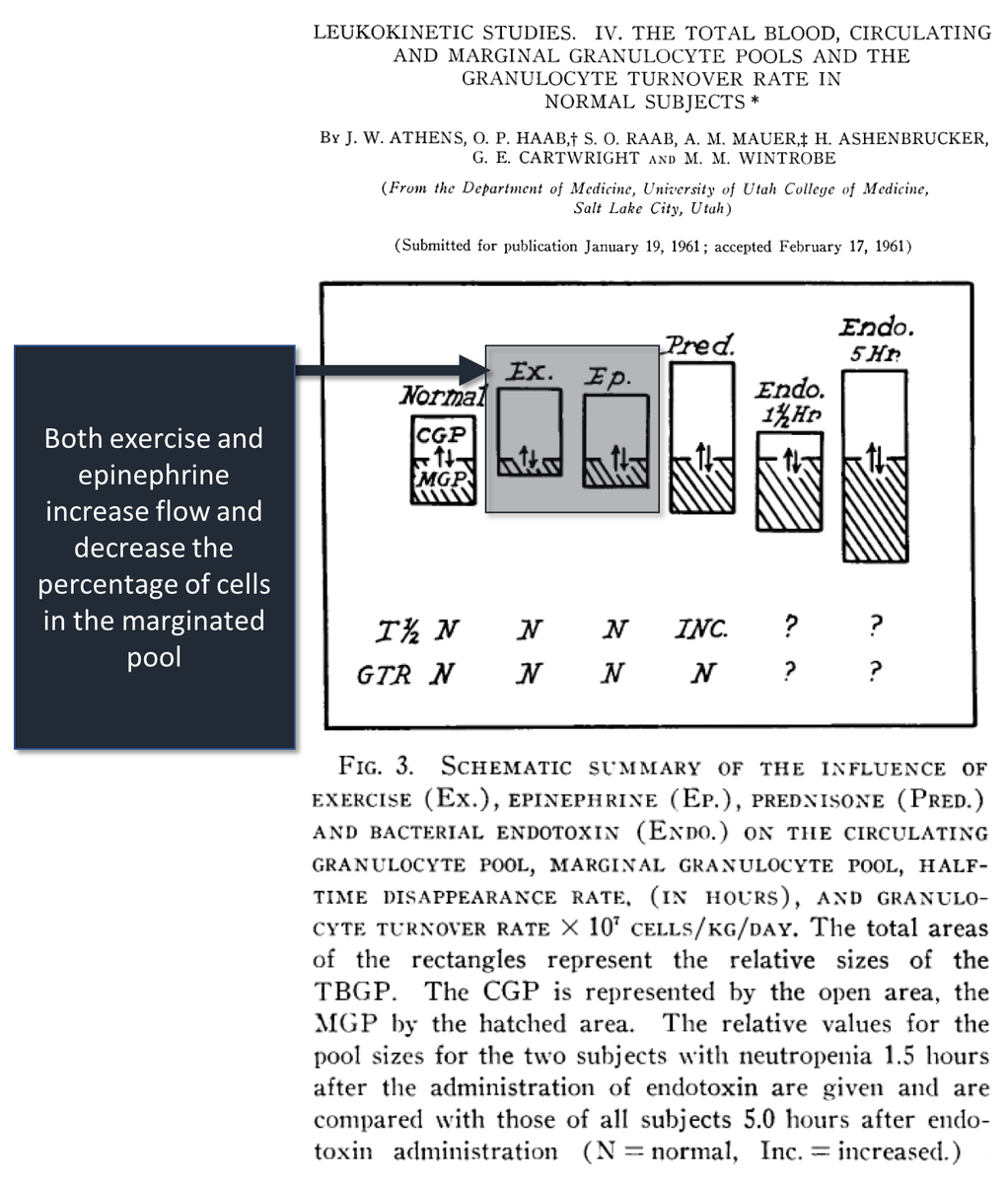
Neutrophils need slower velocities to adhere. Things that increase blood flow are likely to cause fewer neutrophils to adhere/marginate.
Exercise and epinephrine have repeatedly been shown to cause demargination and leukocytosis.
ncbi.nlm.nih.gov/pubmed/13684959
Neutrophils need slower velocities to adhere. Things that increase blood flow are likely to cause fewer neutrophils to adhere/marginate.
Exercise and epinephrine have repeatedly been shown to cause demargination and leukocytosis.
ncbi.nlm.nih.gov/pubmed/13684959
15/
Before summarizing, I'll re-ask the original question: Which of the following is the largest contributor to post-steroid leukocytosis/neutrophilia?
[BM = bone marrow]
Before summarizing, I'll re-ask the original question: Which of the following is the largest contributor to post-steroid leukocytosis/neutrophilia?
[BM = bone marrow]
16/
In summary:
⭐️approximately 50% of neutrophils in the circulation are marginated
⭐️demargination is likely the largest contributor to post-steroid leukocytosis
⭐️demargination also contributes to steroids' anti-inflammatory effects (i.e., neutrophils don't move into tissue)
In summary:
⭐️approximately 50% of neutrophils in the circulation are marginated
⭐️demargination is likely the largest contributor to post-steroid leukocytosis
⭐️demargination also contributes to steroids' anti-inflammatory effects (i.e., neutrophils don't move into tissue)