
,
25 tweets,
9 min read
Read on Twitter
💥Tutorial on ‘Dialysis Adequacy’
⚡️Is Urea a good solute to assess Adequacy ?
⚡️Is Kt/V urea a good Adequacy test?
⚡️Should ‘time on dialysis’ be an independent measure of Adequacy?
⚡️Should ‘UF rate’ be a measure of Adequacy?
@RenalFellowNtwk
#NephPearls
⚡️Is Urea a good solute to assess Adequacy ?
⚡️Is Kt/V urea a good Adequacy test?
⚡️Should ‘time on dialysis’ be an independent measure of Adequacy?
⚡️Should ‘UF rate’ be a measure of Adequacy?
@RenalFellowNtwk
#NephPearls
Urea is not the perfect uremic solute to assess dialysis adequacy, in fact it is far from perfect👇🏽 



Kt/V urea is a measure of the dialysis dose
‘K’ is the dialyzer clearance, ‘T’ is the time on dialysis and ‘V’ is the volume of distribution of urea (which = Total Body Water)
Familiarize yourself with spKt/V, eKt/V and stdKt/V 👇🏽
‘K’ is the dialyzer clearance, ‘T’ is the time on dialysis and ‘V’ is the volume of distribution of urea (which = Total Body Water)
Familiarize yourself with spKt/V, eKt/V and stdKt/V 👇🏽

In PD, Kt/V is ‘measured’ as you collect the dialysate, whereas in HD
Kt/V is ‘estimated’ using a mathematical formula 👇🏽 - why is that?
Well, because it is impractical to collect the dialysate in HD patients
Kt/V is ‘estimated’ using a mathematical formula 👇🏽 - why is that?
Well, because it is impractical to collect the dialysate in HD patients

Kt/V urea has a number of limitations including the fact that the urea kinetics are different from the kinetics of other uremic solutes such as the middle molecules (B2-microglubulin). See 👇🏽

Uremic toxins are classified as small molecules,middle molecules and protein-bound solutes. Small molecules are easily removed by diffusion, middle molecules are removed by convection & protein bound solutes are not removed by either diffusion or convention

Middle molecules are better removed by the native kidneys so try your best to preserve the Residual Renal Function! A few things about the Middle Molecules 👇🏽

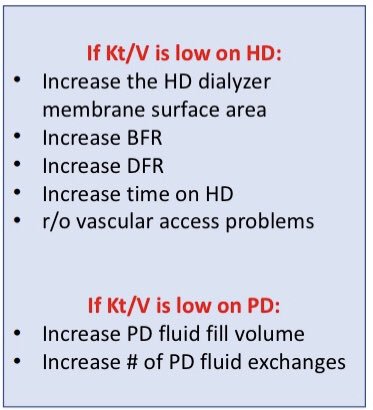
If your patient’s Kt/V does not meet the KDOQI recommended target then what can you do to improve the Kt/V in HD and PD patients 👇🏽
Always take patient’s residual renal function into account
Always take patient’s residual renal function into account
Before we discuss the KDOQI recommended target for Kt/V, we should be familiar with these pivotal RCTs 👇🏽

NCDS Study was published in NEJM in 1981 - it showed that high BUN was associated with higher rate of hospitalization compared to low BUN. And that the dialysis time did not impact hospitalization or mortality👇🏽
This started the trend of short HD treatments..
This started the trend of short HD treatments..


So, if BUN was used to assess dialysis adequacy in the NCDS Study, where did Kt/V urea come from?
Well, it came from the secondary analysis of the NCDS data that resulted in the concept of Kt/V. This analysis showed that Kt/V of <0.9 was bad 👇🏽
Well, it came from the secondary analysis of the NCDS data that resulted in the concept of Kt/V. This analysis showed that Kt/V of <0.9 was bad 👇🏽

In 2002, another important study - the HEMO Study was published in NEJM - 21 years after the NCDS Trial 👇🏽
The HEMO study compared standard dose vs. high dose hemodialysis, and low flux vs. high flux hemodialysis
The HEMO study compared standard dose vs. high dose hemodialysis, and low flux vs. high flux hemodialysis

So what did the HEMO Study show?
⚡️No difference in survival between standard dose vs high dose HD
(spKt/V 1.3 vs. spKt/V 1.7)
⚡️No difference in survival between low flux vs. high flux HD
👇🏽
⚡️No difference in survival between standard dose vs high dose HD
(spKt/V 1.3 vs. spKt/V 1.7)
⚡️No difference in survival between low flux vs. high flux HD
👇🏽


Even though the HEMO study did not show an overall survival benefit between standard dose vs. high dose HD, there were differences in sub-group analysis
⚡️Among women, high dose HD was associated with 19% lower mortality compared to standard dose HD
⚡️Among women, high dose HD was associated with 19% lower mortality compared to standard dose HD

Possible explanation for this - women tend to have lower ‘Volume’ to ‘Body Surface Area’ (BSA) ratio compared to men. And remember ‘V’ is the denominator in the Kt/V calculation, so it is possible that using ‘V’ rather than ‘BSA’ in women overestimates Kt/V

Another possible explanation for better survival among women in the high dose group is probably the ‘time on dialysis’. In the HEMO Study, women in the standard dose group dialyzed for only 180 minutes compared to the men who dialyzed for 200 minutes

Time on Dialysis can be a surrogate marker for the following:
⚡️Total solute removal
⚡️Rate of fluid removal
⚡️Middle Molecule Clearance
⚡️Phosphorus removal
⚡️Total solute removal
⚡️Rate of fluid removal
⚡️Middle Molecule Clearance
⚡️Phosphorus removal
So, should time on HD be an independent measure of Dialysis Adequacy regardless of Kt/V?
⚡️Yes
-KDOQI recommends a minimum of 3hrs/session for 3x/wk HD
-European Practice Guidelines recommends at least 4 hrs HD/session
-Of course, one has to consider the RRF
⚡️Yes
-KDOQI recommends a minimum of 3hrs/session for 3x/wk HD
-European Practice Guidelines recommends at least 4 hrs HD/session
-Of course, one has to consider the RRF
What about the Ultrafiltration rate?
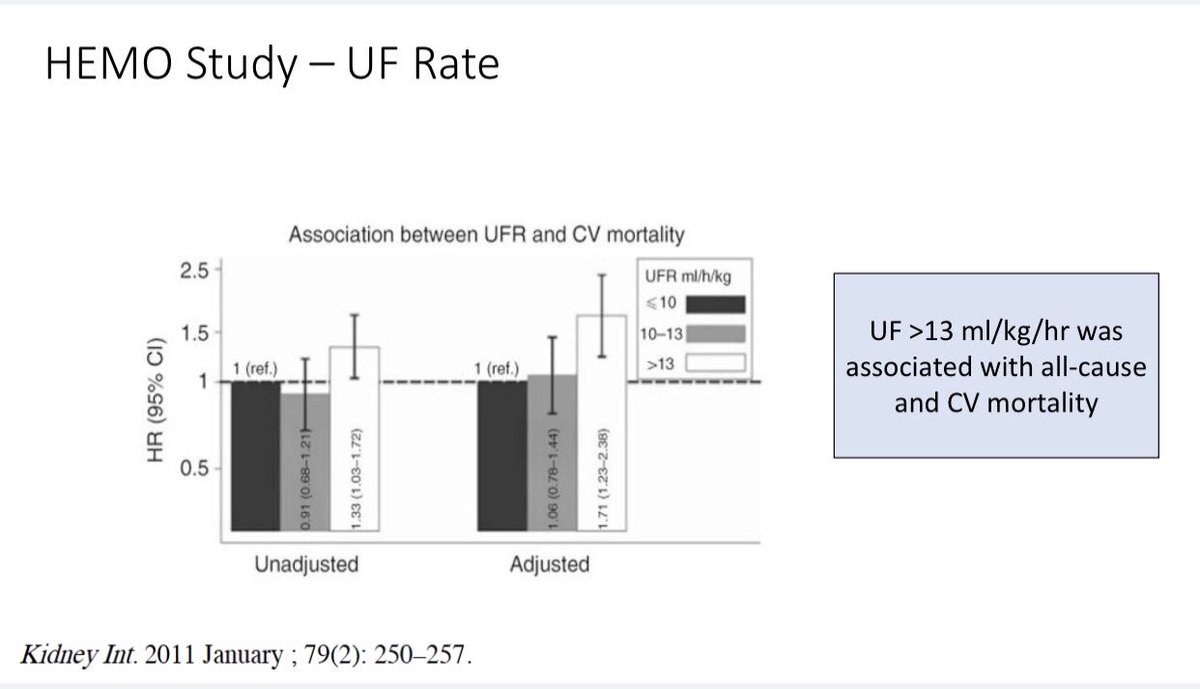
Analysis of the HEMO Study showed that UF rate >13 mls/kg/hr is associated with higher mortality 👇🏽
Other studies have shown similar results
Analysis of the HEMO Study showed that UF rate >13 mls/kg/hr is associated with higher mortality 👇🏽
Other studies have shown similar results
High UF rate is associated with higher incidence of intra-dialytic hypotension which has been shown to cause Myocardial Stunning and Cerebral Stunning. So, low systolic BP during HD is bad for the ♥️ and the 🧠
We also know that frequent hemodialysis (FHD) is associated with lower UF rates which in turn is associated with less intra-dialytic hypotension and results in less ♥️ stunning
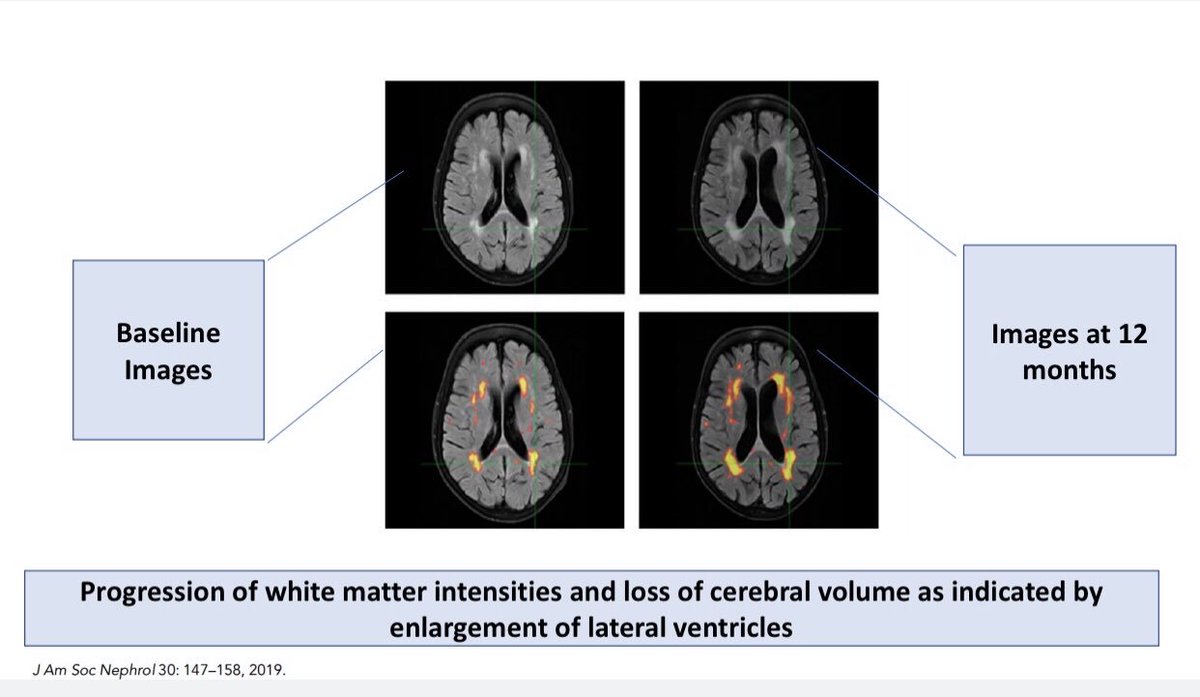
Let’s look at a recent study which showed occurrence of cerebral stunning in HD patients
Just like myocardial stunning, 🧠 stunning was associated with high UF rates
BTW, this was also associated w/ cerebral white matter changes & cognitive impairment 🥺
Just like myocardial stunning, 🧠 stunning was associated with high UF rates
BTW, this was also associated w/ cerebral white matter changes & cognitive impairment 🥺

What about Peritoneal Dialysis and Dialysis Adequacy?
2 important studies to be familiar with are:
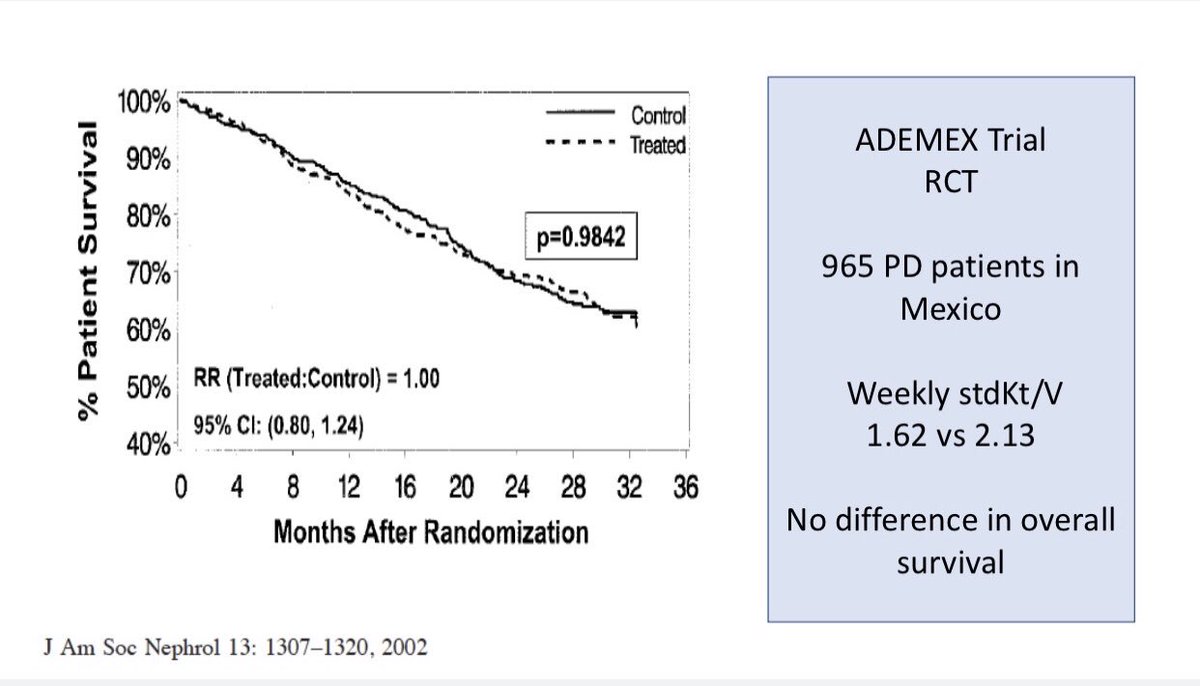
⚡️The ADEMEX Trial
⚡️The Hong Kong PD Trial
Results 👇🏽
2 important studies to be familiar with are:
⚡️The ADEMEX Trial
⚡️The Hong Kong PD Trial
Results 👇🏽

Before we summarize the KDOQI recommendations for Dialysis Adequacy let’s review the concept of standardized Kt/V which allows for comparison of Adequacy
b/w different dialysis modalities and is based on weekly dosing. Take a look at this illustration 👇🏽
b/w different dialysis modalities and is based on weekly dosing. Take a look at this illustration 👇🏽

So here are the current KDOQI recommendations for Dialysis Adequacy:
⚡️Target minimum spKt/V urea > 1.2 and target 1.4 or > for 3x/week HD
⚡️Target weekly Kt/V of > 1.7 for PD
⚡️Target Kt/V for FHD is opinion-based to meet the weekly standard
Kt/V of 2.0
⚡️Target minimum spKt/V urea > 1.2 and target 1.4 or > for 3x/week HD
⚡️Target weekly Kt/V of > 1.7 for PD
⚡️Target Kt/V for FHD is opinion-based to meet the weekly standard
Kt/V of 2.0









