,
24 tweets,
9 min read
Read on Twitter
💥How do SGLT2 Inhibitors work?
💥How does an anti-diabetic drug improve Renal & Cardiovascular outcomes?
💥To understand this let’s first review:
⚡️Renal handling of glucose
1/
@RenalFellowNtwk
#NephJC
#SGLT2
#CREDENCE
💥How does an anti-diabetic drug improve Renal & Cardiovascular outcomes?
💥To understand this let’s first review:
⚡️Renal handling of glucose
1/
@RenalFellowNtwk
#NephJC
#SGLT2
#CREDENCE
💥Renal handling of glucose:
⚡️180 g of glucose is filtered thru the glomeruli every day
(180 L x 100mg/dL)
⚡️But all the glucose is completely reabsorbed
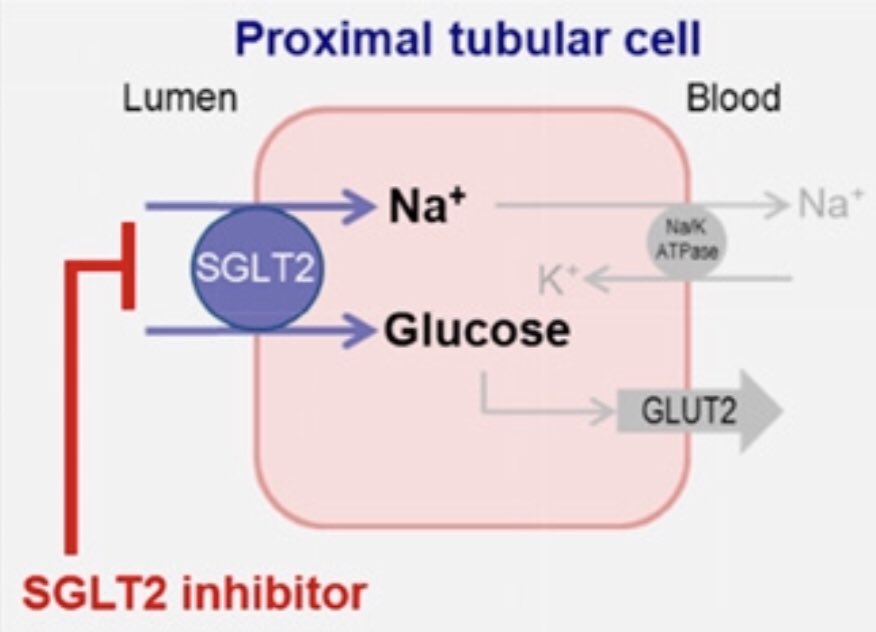
⚡️Renal reabsorption of glucose occurs thru transporters in the proximal tubule called SGLT
2/
⚡️180 g of glucose is filtered thru the glomeruli every day
(180 L x 100mg/dL)
⚡️But all the glucose is completely reabsorbed
⚡️Renal reabsorption of glucose occurs thru transporters in the proximal tubule called SGLT
2/
💥Sodium-Glucose Co-transporters (SGLT)
⚡️There are many 👇🏽
⚡️Not all of them are located in the kidney👇🏽
3/
⚡️There are many 👇🏽
⚡️Not all of them are located in the kidney👇🏽
3/

💥SGLT2 & SGLT1 - located in the proximal tubule & are responsible for renal glucose reabsorption
⚡️SGLT2 - high capacity, low affinity, reabsorbs 90% glucose - this is where SGLT2 Inh. work👇🏽
⚡️SGLT1 - low capacity, high affinity, reabsorbs 10% glucose
4/
⚡️SGLT2 - high capacity, low affinity, reabsorbs 90% glucose - this is where SGLT2 Inh. work👇🏽
⚡️SGLT1 - low capacity, high affinity, reabsorbs 10% glucose
4/
💥Glucose is freely filtered in the glomerulus
⚡️⬆️ glucose in plasma = ⬆️ glucose in the glomerular filtrate
⚡️Renal reabsorption of glucose ⬆️ till max. reabsorptive capacity is reached (BG ~180 mg/dL), resulting in glucosuria
5/
⚡️⬆️ glucose in plasma = ⬆️ glucose in the glomerular filtrate
⚡️Renal reabsorption of glucose ⬆️ till max. reabsorptive capacity is reached (BG ~180 mg/dL), resulting in glucosuria
5/
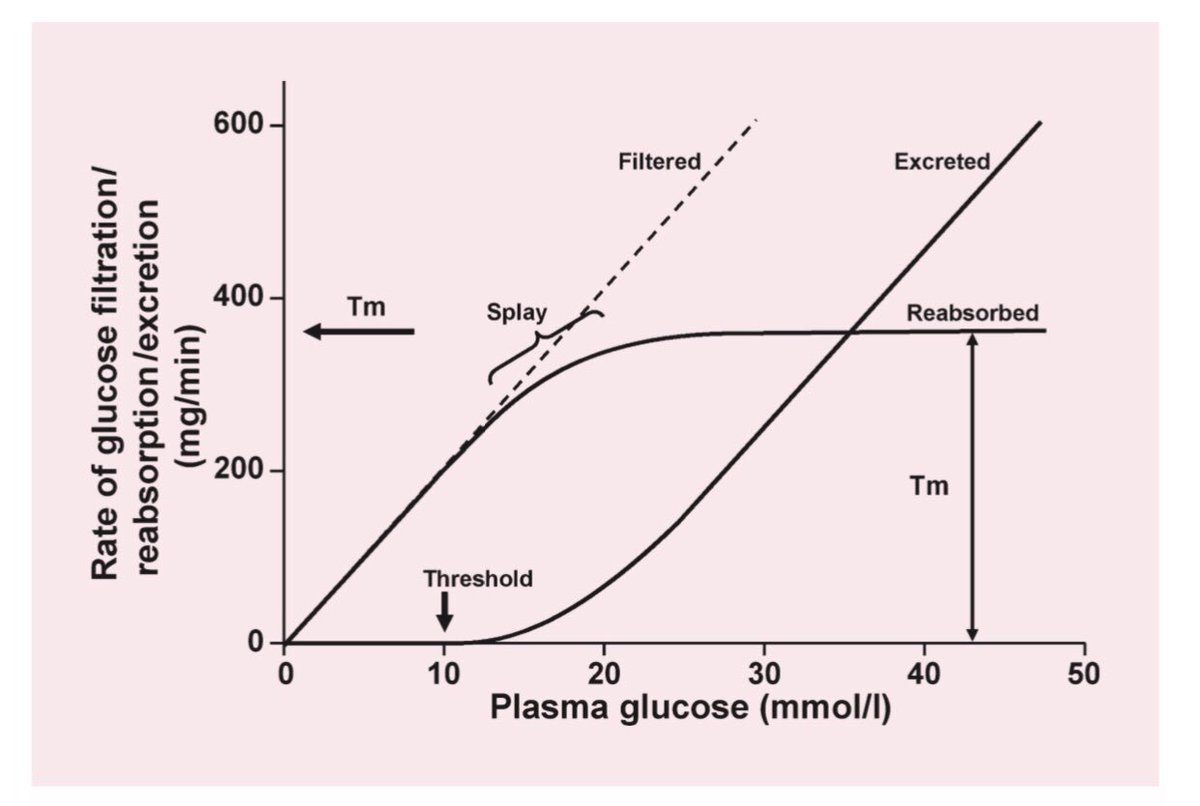
💥Renal handling of glucose is different in DM vs. Non-DM 👇🏽
⚡️Glucosuria in diabetics occurs at a much higher plasma glucose conc. as their reabsorptive capacity is ⬆️
(420 mg/min vs. 350 mg/min)
⚡️There is 4-fold up-regulation of SGLT2 expression
6/
⚡️Glucosuria in diabetics occurs at a much higher plasma glucose conc. as their reabsorptive capacity is ⬆️
(420 mg/min vs. 350 mg/min)
⚡️There is 4-fold up-regulation of SGLT2 expression
6/

💥This makes SGLT2 Inh. an attractive option to Rx DM -> it ⬇️ the threshold for glucose reabsorption causing glucosuria
Their action is:
⚡️dependent on blood glucose level
⚡️independent of insulin hence there is ⬇️ risk of hypoglycemia
7/
Their action is:
⚡️dependent on blood glucose level
⚡️independent of insulin hence there is ⬇️ risk of hypoglycemia
7/
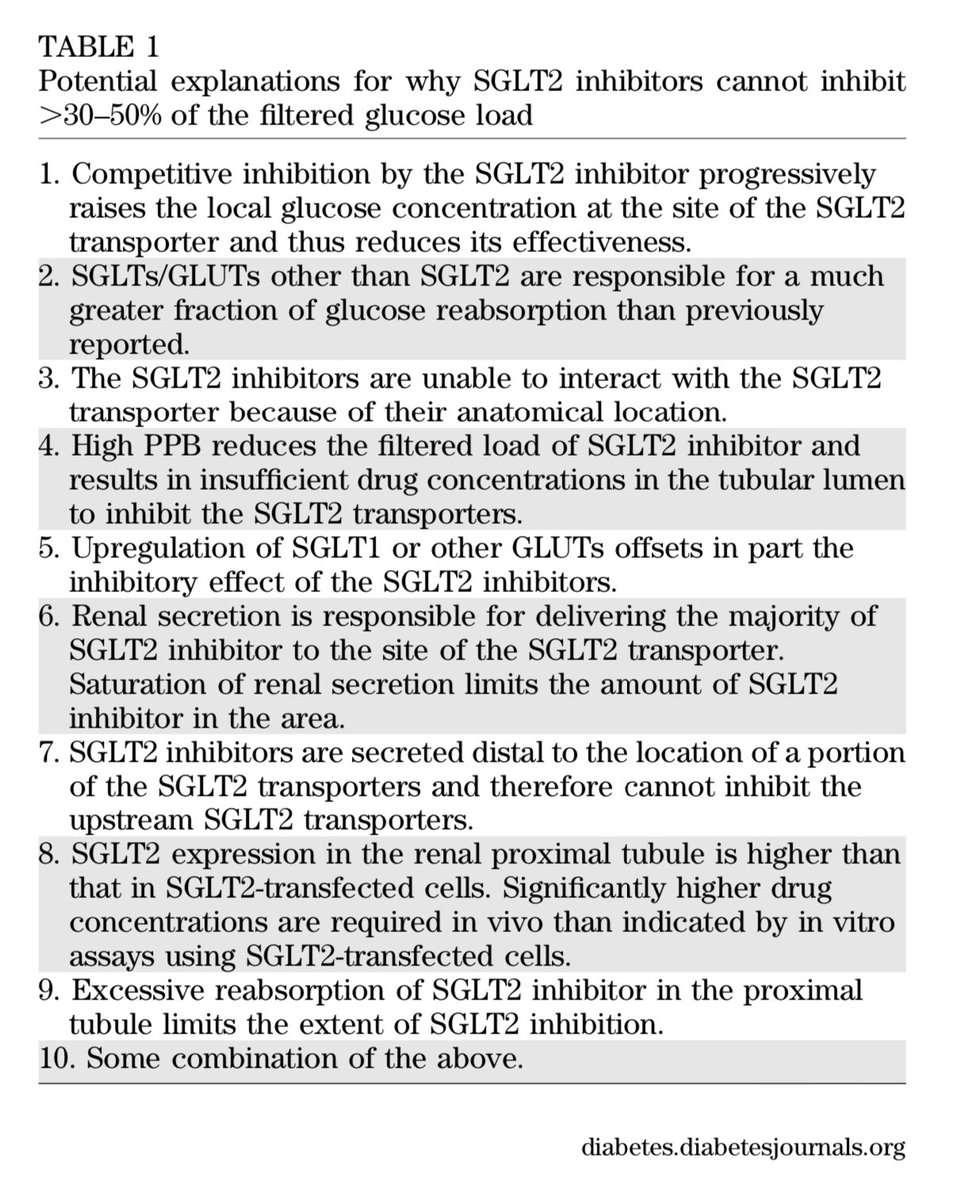
💥It is intriguing that even though SGLT2 is responsible for ~90% reabsorption of the filtered glucose load, the SGLT2 Inhibitors inhibit only 30%-50% (50-80 grams) of renal glucose reabsorption
⚡️Some potential explanations for this are 👇🏽
8/
⚡️Some potential explanations for this are 👇🏽
8/

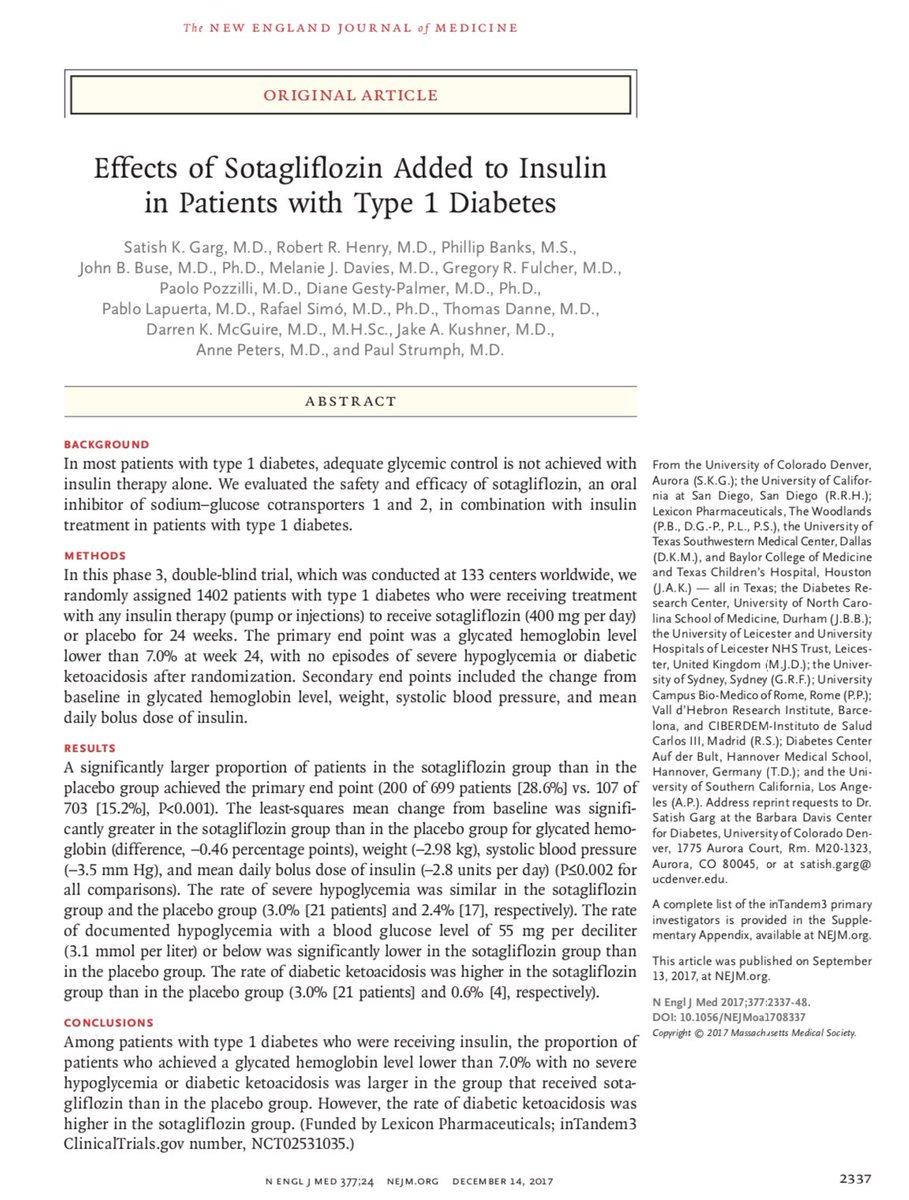
💥What about use of SGLT1 inh. for DM Rx?
⚡️SGLT1 is predominantly expressed in the intestine & ❌ this ⬇️ glucose absorption from the gut -> improving glycemic control
⚡️Sotagliflozin (SGLT2/1 Inh.) & GSK-1614235 (SGLT1 Inh.) have been tested👇🏽
9/
⚡️SGLT1 is predominantly expressed in the intestine & ❌ this ⬇️ glucose absorption from the gut -> improving glycemic control
⚡️Sotagliflozin (SGLT2/1 Inh.) & GSK-1614235 (SGLT1 Inh.) have been tested👇🏽
9/

💥Let’s get back to SGLT2 Inhibitors:
⚡️Are they Anti-diabetic agents?
⚡️Are they diuretics?
⚡️Do they cause weight loss?
⚡️Are they Anti-HTN agents?
⚡️Do they lower intra-glomerular pressure?
10/
⚡️Are they Anti-diabetic agents?
⚡️Are they diuretics?
⚡️Do they cause weight loss?
⚡️Are they Anti-HTN agents?
⚡️Do they lower intra-glomerular pressure?
10/
💥SGLT2 Inhibitors - are they anti-diabetic agents? ✅
⚡️In most trials, the HbAIC was 0.4% - 0.8% ⬇️ in the SGLT2 Inh. group vs. placebo
11/
⚡️In most trials, the HbAIC was 0.4% - 0.8% ⬇️ in the SGLT2 Inh. group vs. placebo
11/

💥Given the mechanism of it’s action it is not surprising that the glucose lowering effect of SGLT2 Inhibitors declines at lower GFR 👇🏽
12/
12/

💥SGLT2 Inhibitors also ⬆️ fat oxidation & ketogenesis, and ⬇️ carbohydrate utilization
13/
13/
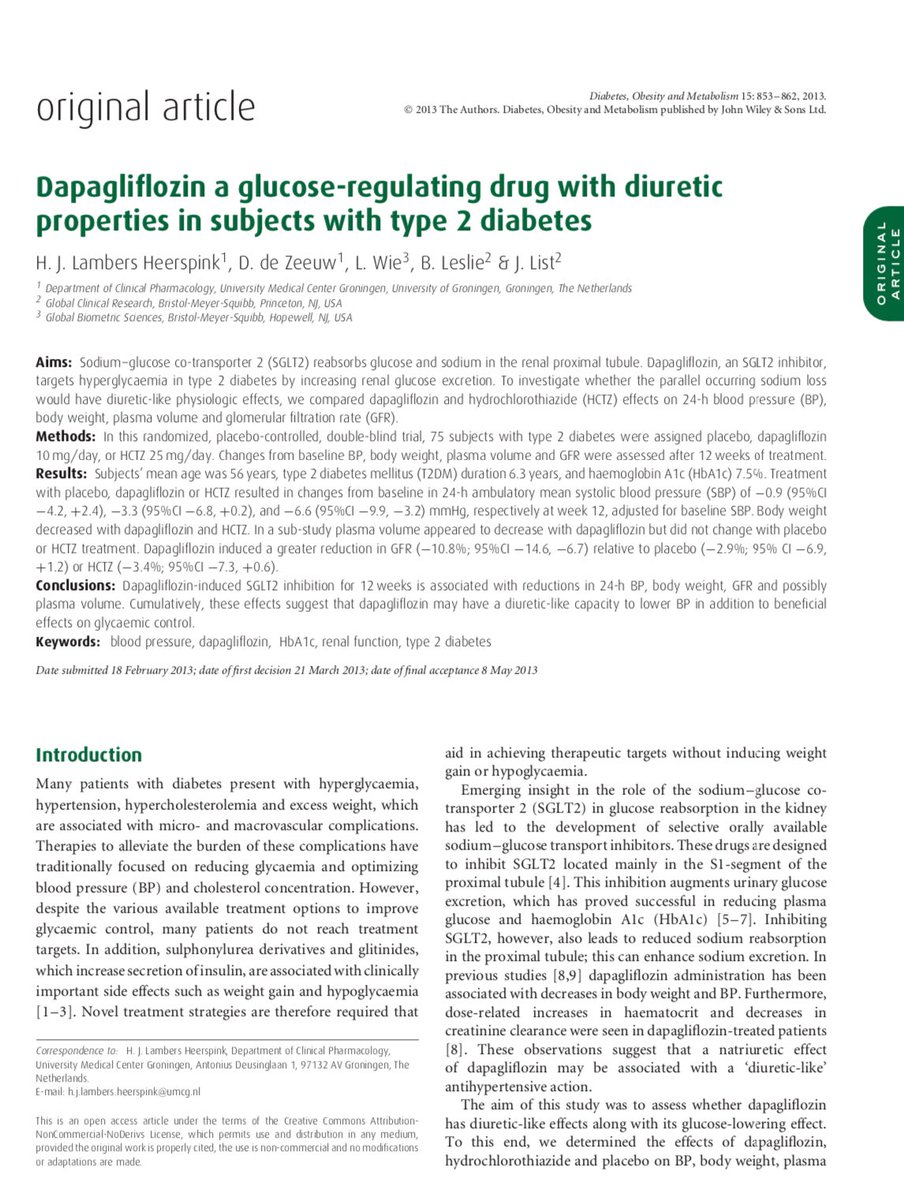
💥SGLT2 Inhibitors - Are they diuretics? ✅
⚡️ Sodium-glucose co-transporter blockage causes glucosuria -> osmotic diuresis -> ⬆️ urine output
⚡️This is supported by ⬇️ plasma volume & ⬆️ hematocrit
⚡️There is natriuresis but this effect is transient
14/
⚡️ Sodium-glucose co-transporter blockage causes glucosuria -> osmotic diuresis -> ⬆️ urine output
⚡️This is supported by ⬇️ plasma volume & ⬆️ hematocrit
⚡️There is natriuresis but this effect is transient
14/

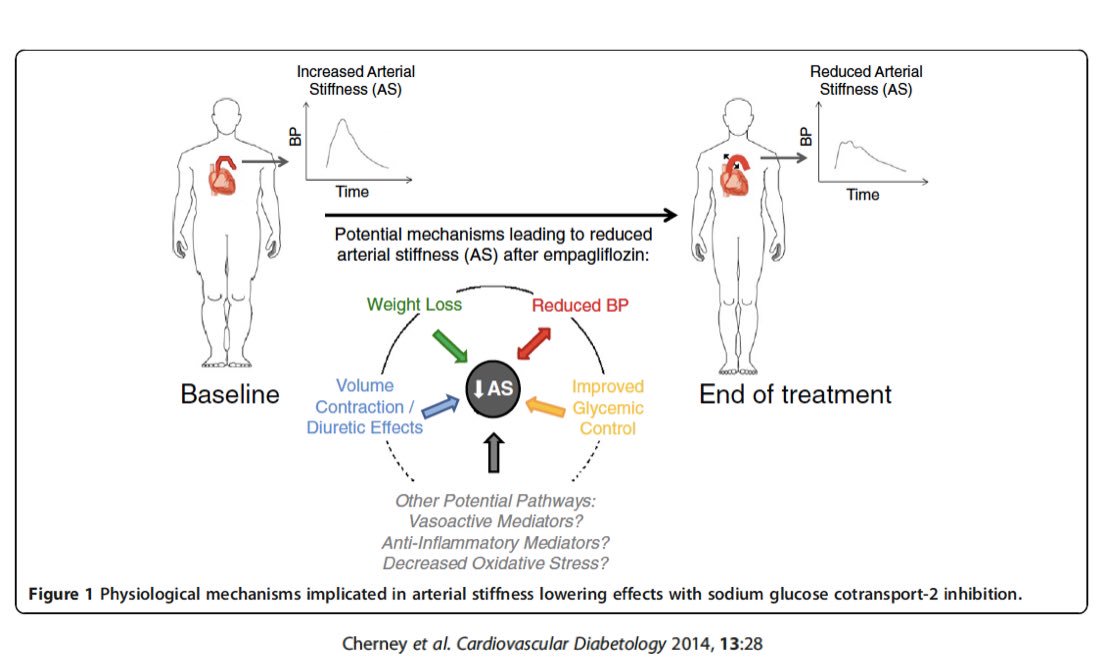
💥SGL2 Inhibitors ⬇️ arterial stiffness ⚡️⬇️ SNS activation
⚡️Do not cause reflex tachycardia despite hemodynamic changes
15/
⚡️Do not cause reflex tachycardia despite hemodynamic changes
15/
SGLT2 Inh. - Do they cause weight loss? ✅ ~2 kg over ~6 months
⚡️Wt. loss seen earlier with it’s use is likely due to osmotic diuresis
⚡️Wt. loss seen later is likely from ⬇️ in body fat due to calories lost due to glucosuria (~300 kcal/d)
16/
⚡️Wt. loss seen earlier with it’s use is likely due to osmotic diuresis
⚡️Wt. loss seen later is likely from ⬇️ in body fat due to calories lost due to glucosuria (~300 kcal/d)
16/
SGLT2 Inh. - Are they anti-HTN agents? ✅
⚡️⬇️ systolic BP by 3-4 mm & diastolic BP by 1-2 mm
⚡️Due to diuretic effect, wt. loss, ⬇️ arterial stiffness ⬇️ SNS activation
⚡️👆🏽 may explain why the anti-HTN effect persists even at lower GFR
17/
⚡️⬇️ systolic BP by 3-4 mm & diastolic BP by 1-2 mm
⚡️Due to diuretic effect, wt. loss, ⬇️ arterial stiffness ⬇️ SNS activation
⚡️👆🏽 may explain why the anti-HTN effect persists even at lower GFR
17/
💥SGLT2 Inh. - impacts renal hemodynamics? Likely ✅
⚡️SGLT2 blockade -> ⬆️ Na delivery to macula densa -> activates tubuloglomerular feedback-> ⬆️ afferent arterial tone -> ⬇️ intra-glom pressure
⚡️👆🏽 likely improves albuminuria & slows CKD progression
18/
⚡️SGLT2 blockade -> ⬆️ Na delivery to macula densa -> activates tubuloglomerular feedback-> ⬆️ afferent arterial tone -> ⬇️ intra-glom pressure
⚡️👆🏽 likely improves albuminuria & slows CKD progression
18/

💥Is the positive impact on CV & Renal outcomes explained by it’s anti-glycemic effect
⚡️Likely not - as the reduction in A1C is modest & other diabetic drugs w/ similar A1C affect have not shown similar Renal & CV outcomes (exception: GLP-1RA)
19/
⚡️Likely not - as the reduction in A1C is modest & other diabetic drugs w/ similar A1C affect have not shown similar Renal & CV outcomes (exception: GLP-1RA)
19/
💥 Benefits of SGLT2 Inh. r not explained by any of these individually: glucose ⬇️, BP ⬇️, diuretic, wt. loss, ⬇️ intra-glomerular pressure,
⬇️ arterial stiffness
⚡️But perhaps it’s the combination of all these that produce the Renal & CV benefits👇🏽
20/
⬇️ arterial stiffness
⚡️But perhaps it’s the combination of all these that produce the Renal & CV benefits👇🏽
20/

💥SGLT2 Inh. - adverse effects:
⚡️Genital infections
⚡️DKA
⚡️Volume depletion/AKI
⚡️? Amputations (not seen in the #CREDENCE Trial)
21/
⚡️Genital infections
⚡️DKA
⚡️Volume depletion/AKI
⚡️? Amputations (not seen in the #CREDENCE Trial)
21/
💥SGLT2 Inh. are currently approved for:
⚡️Rx of T2DM - add on to metformin if A1C ⬆️
⚡️ T2DM + CV disease
⚡️FDA currently does not approve it’s use at GFR <45 ml’s/min but..
22/
⚡️Rx of T2DM - add on to metformin if A1C ⬆️
⚡️ T2DM + CV disease
⚡️FDA currently does not approve it’s use at GFR <45 ml’s/min but..
22/
...the recently published #CREDENCE Trial has shown than SGLT2 Inhibitors ⬇️ risk of CKD progression & ⬇️ CV events even at low GFR (down to 30 mls/min)
23/
23/