The upside of defining contrast nephropathy in this way is it becomes very easy to measure the incidence of AKI. In 6 recent well done studies, the incidence runs from 1 to 11% among patients with CKD.
The studies are either retrospective reviews or from prospective studies from the recent low osmolar vs iso-osmolar contrast wars. These ended with a cease-fire but hostilities could re-ignite at any time.
The problem with these studies is they attribute all of the AKI to contrast, but surely there is a background rate of AKI? I give you Newhouse et al. who suspected that there may be some alternative causes of AKI besides contrast...🤔 ncbi.nlm.nih.gov/pubmed/18647905
If not all AKI is due to contrast, then how will we determine the rate of contrast nephropathy? This is a job for a controlled trial. 

There are no prospective randomized trials, but retrospective trials like this one by Heller, actually show a lower rate of AKI with contrast than without contrast. Wait...What?


This trend to lower risk with contrast was upheld in a meta-analysis of 13 of these retrospective trials (yeah I see that it was NS, but work with me)

Patients, that doctors see as high risk for AKI, get shifted away from IV contrast. So the “no contrast group” is enriched with high risk patients. The ideal way to deal with this is a randomized controlled trial. But there isn’t one. The next best thing is propensity scoring.
Individual patient have variable propensity for developing AKI following contrast. Patients with low GFR have higher risk. Patients with diabetes have higher risk. We can give every patient a propensity score based on that risk.

The beauty of randomization is the risk gets balanced between groups.

The problem with observational controlled trials is clever doctors keep trying to avoid contrast in their high risk patients, so that means the “No contrast” group is fortified with an additional helping of high-risk patients.
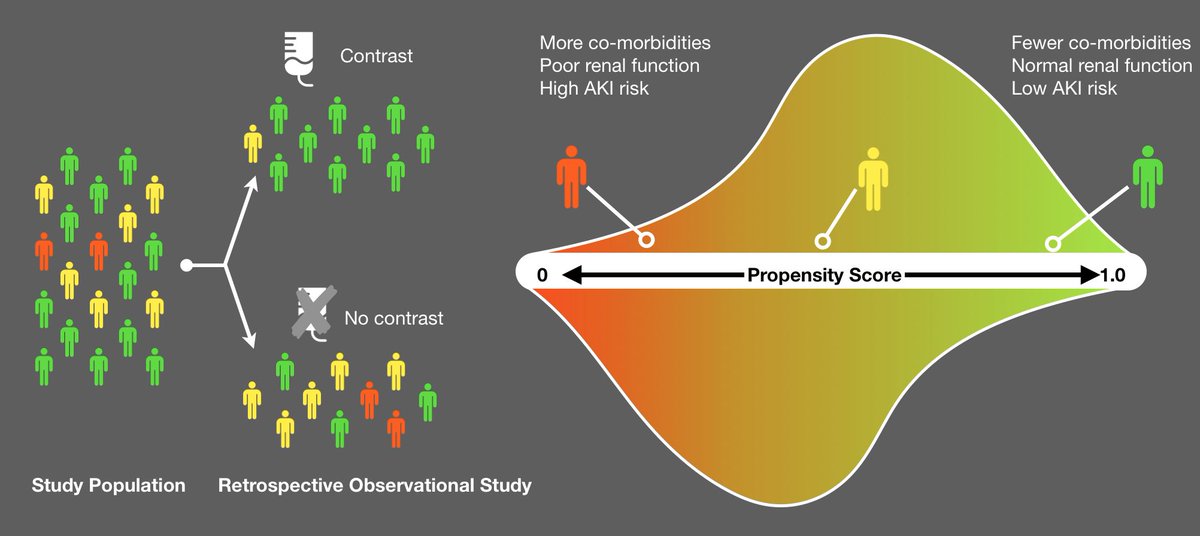
To fight this, statisticians do propensity matching where both sides get the same number of patients from every risk category.

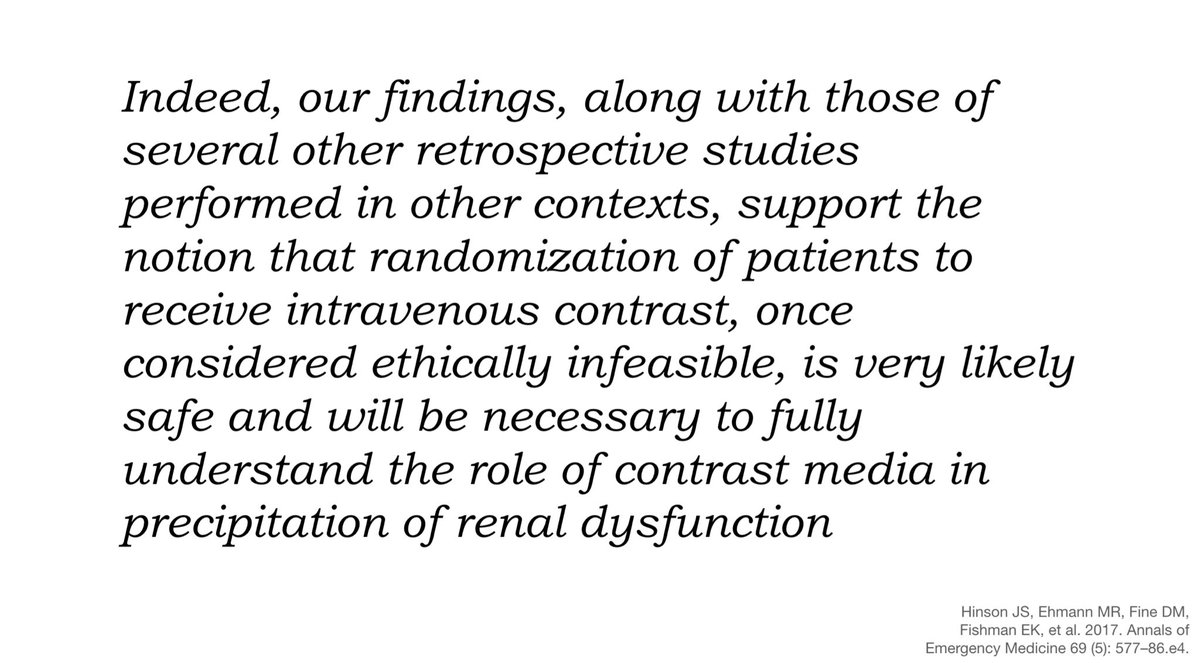
When this was done for contrast, the protective effect of contrast went away but there was no detectable excess risk of AKI from contrast. If contrast causes AKI it does so, so rarely as to be undetectable by the most sophisticated analysis available.



In the conclusion of Hinson’s propensity scored analysis, the authors wrote (annemergmed.com/article/S0196-…)
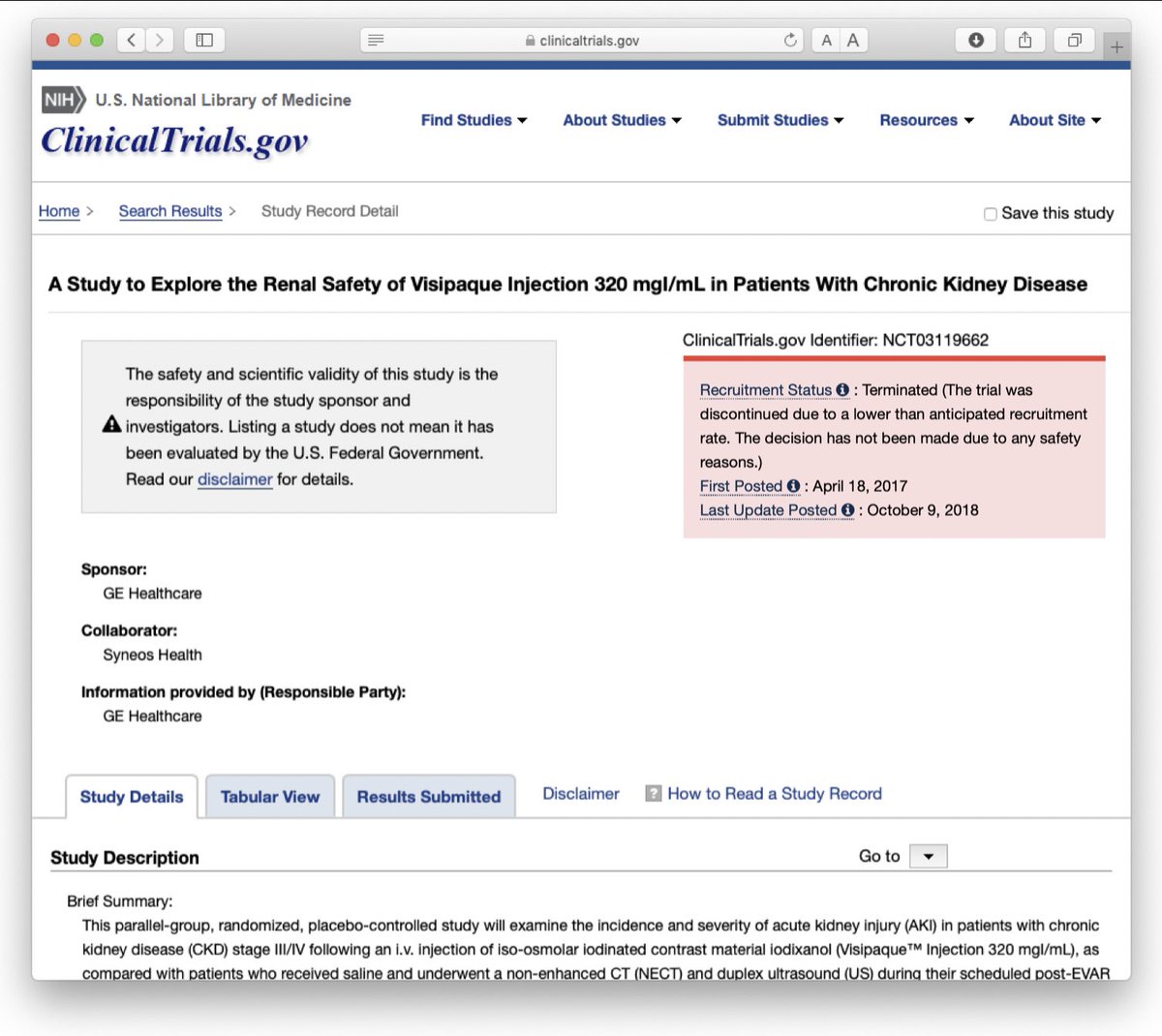
GE saw this and started a protocol to randomize patients. The indication was monitoring endovascular repair of abdominal aortic aneurysms. Patients with aortic stents go for yearly imaging, either CT w/o contrast + U/S or contrast CT. There is equipoise in imaging modality choice
The protocol can be seen at clinicaltrials.gov NCT03119662 but it was abandoned due to insufficient recruitment. It turns out that even though contrast researchers have equipoise, the wider physician community does not.
So without a randomized clinical trial this is what we are left with. The highest quality epidemiology studies are unable to detect any increase in AKI, so those bumps in creatinine following contrast are almost certainly run of the mill AKI and not contrast induced AKI.