Here are the results of the poll I did yesterday. 1,105 votes. Probably not the best sample size but a rough idea what the people think about our healthcare.
Any thoughts before I continue?
I myself would have probably voted "depends on condition" too.
Any thoughts before I continue?
I myself would have probably voted "depends on condition" too.
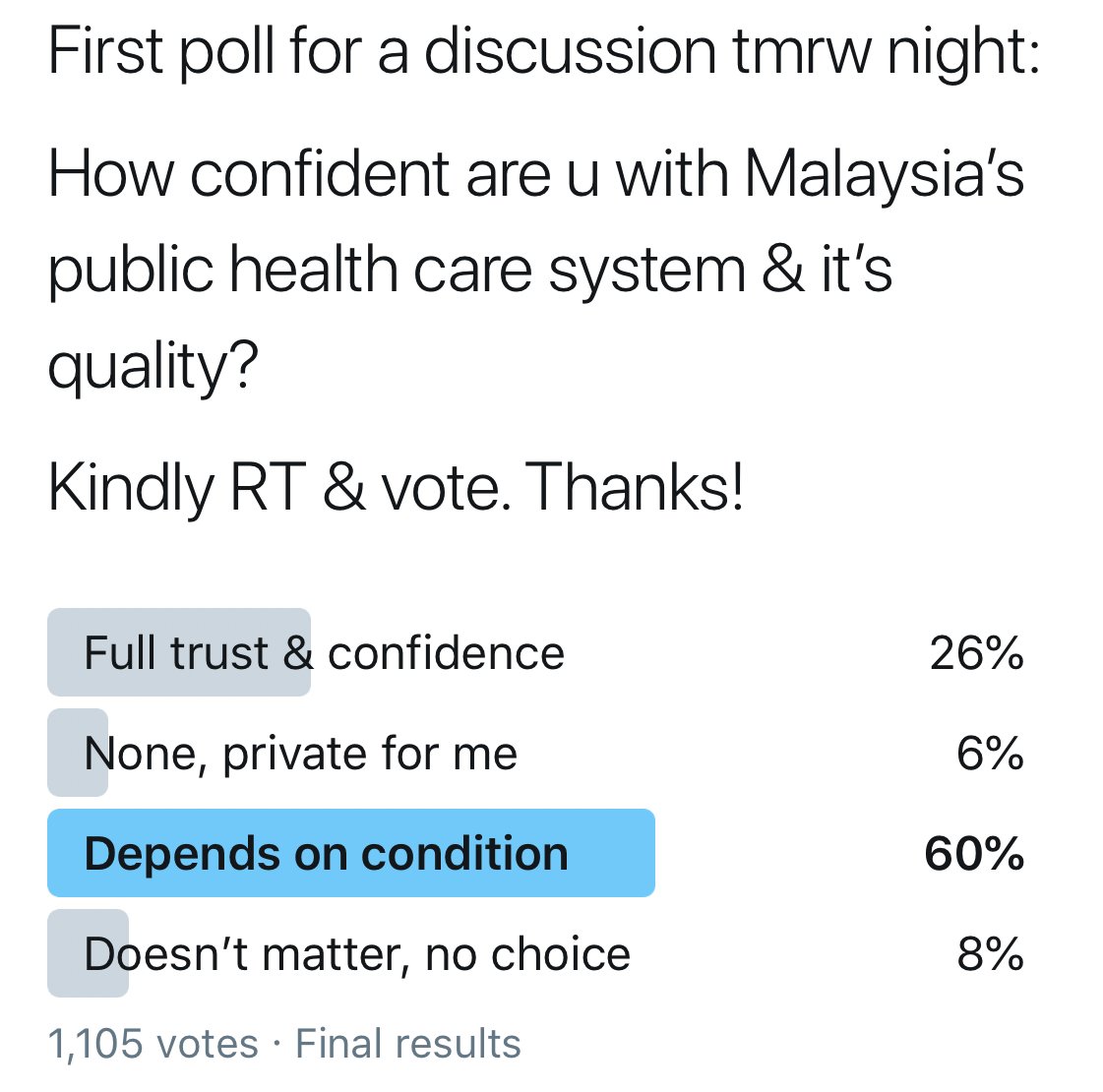
Obviously there is no 'correct' answer here, many factors play into how one feel about any healthcare service, be it public or private.
But in our setting, 'depends on condition' is quite sensible but in reality, Twitterjaya is not the whole of Malaysia, and probably 'doesnt matter, no choice' is the most accurate, in a sense.
M'sia practice universal health care system. The term 'subsidised by the govt' is a bit of a misnomer, IMHO.
'Subsidised by govt' denote that the govt is paying an entity, like a private corporation to supply healthcare.
But it's not. Services r given by govt, paid by taxes.
'Subsidised by govt' denote that the govt is paying an entity, like a private corporation to supply healthcare.
But it's not. Services r given by govt, paid by taxes.
But I'm not here to shoot out numbers like GDP spending, patient doctor ratio or bed numbers, I think there r smarter ppl who can give u that info, or u can Google.
I prefer to tell it as it is, from my experience as a healthcare worker.
I prefer to tell it as it is, from my experience as a healthcare worker.
Like any OCD doctor, I like to list out things. So I'll cerita along 3 phases of my career.
1. In the Emergency Dept in a tertiary hospital
2. Primary healthcare in rural area
3. Nephrology as a subspeciality, also in a tertiary hospital
1. In the Emergency Dept in a tertiary hospital
2. Primary healthcare in rural area
3. Nephrology as a subspeciality, also in a tertiary hospital
The Emergency Dept (ED) is probably the most chaotic part of the hospital (apart from the canteen 😂)
I spend the last 4 months as a HO there & couple of months as a junior MO before getting posted out.
I spend the last 4 months as a HO there & couple of months as a junior MO before getting posted out.
The ED is like the sorting hat of a hospital, u come in with a health complain, the doctors will divide u two ways.
1. How critical are u?
2. What speciality your complain belong to, if needed for further treatment (not all complains need to be forwarded, some r treated in ED)
1. How critical are u?
2. What speciality your complain belong to, if needed for further treatment (not all complains need to be forwarded, some r treated in ED)
& the ED is open 24/7, so there is no downtime or rest period, it just functions non stop at max capacity, all year round.
The ED received patients walking in w a complain or by ambulance. So the patient load is tremendous.
The ED received patients walking in w a complain or by ambulance. So the patient load is tremendous.
Anyway I am rambling.
ED patients come in by the hundreds per day, from minor illnesses to major ones.
Doctors & resources r often stretched at the ED. When there are influx of patients, they get 'stuck' at ED before getting a bed up in the wards. We call this access block.
ED patients come in by the hundreds per day, from minor illnesses to major ones.
Doctors & resources r often stretched at the ED. When there are influx of patients, they get 'stuck' at ED before getting a bed up in the wards. We call this access block.
That is why we see EDs being filled up with no where to go because beds are not empty in the wards, simply because there isnt enough of it.
This, obviously is not safe for patients. ED is not a ward & there is very little close monitoring done, unlike the wards.
This, obviously is not safe for patients. ED is not a ward & there is very little close monitoring done, unlike the wards.
How do we overcome access blocks? Increasing no. of beds is the simplest way, but in reality, it's not just adding beds. More beds = more resources needed, more doctors, nurses, equipment, medication.
But this is not happening.
But this is not happening.
So in reality, patient load increases because private health care costs r getting higher.
Resources at govt hospitals r getting stretched, while private hospitals still look kinda cool, no issues (if u can afford that is)
This is 1 reason why ppl think private might be better.
Resources at govt hospitals r getting stretched, while private hospitals still look kinda cool, no issues (if u can afford that is)
This is 1 reason why ppl think private might be better.
Next is my time in primary healthcare in the rural area, I spent 1 year in N9.
My clinic is small, only a team of 2 doctors (myself included), 2 MAs & nurses. We run emergency/outpatient services, a non communicable disease (NCD) unit & a mother child clinic (MCH)
My clinic is small, only a team of 2 doctors (myself included), 2 MAs & nurses. We run emergency/outpatient services, a non communicable disease (NCD) unit & a mother child clinic (MCH)
Our equipment & meds are truly basic, anything we cant handle, we need to stabilise & send to a hospital, about 1/2 hour away.
Small place but we still see about 50-80 patients in the morning (NCD) and noons we keep for MCH appointments, like scans, antenatal booking
Small place but we still see about 50-80 patients in the morning (NCD) and noons we keep for MCH appointments, like scans, antenatal booking
Every month, we travel in to 1 orang asal kampung, called Langkap. We have a small hut there, but it's basically a mobile clinic. Even more basic.
Luckily I didnt have any emergencies there though, now that I think about it. 😅
Luckily I didnt have any emergencies there though, now that I think about it. 😅
Short break; best part of working in rural areas is that u will never go hungry. My nurses seem to have food magically appear everyday, during Raya is the best.
Also, patients like to give u food. 1 makcik wanted to give me live chicken. 😂
Also, patients like to give u food. 1 makcik wanted to give me live chicken. 😂
Patients r the cutest too. 1 makcik ask me for ubat kutu, I asked how many of the kids have kutu.
She tells me it is for her cat. 🤦🏻♂️
She tells me it is for her cat. 🤦🏻♂️
Anyway, off tangent already. I'm like an old man who cant stop talking.
Primary healthcare in rural areas offer access no private healthcare can. It is still far from being 100% accessible, but the work we do make a difference in many rural communities.
Primary healthcare in rural areas offer access no private healthcare can. It is still far from being 100% accessible, but the work we do make a difference in many rural communities.
Next is Nephrology, or kidney subspecialty.
Kidney disease as u might know, is exponentially increasing by the day. Dialysis patient are increasing & what else but costs also going up.
Kidney disease as u might know, is exponentially increasing by the day. Dialysis patient are increasing & what else but costs also going up.
Nephro is divided to few other units but generally each clinic day we also see about 100+ patients, in addition, we need to see emergency patients, prepare patients for surgery or procedures.
Nephro is unique in a sense most of our patients r long term with us.
Nephro is unique in a sense most of our patients r long term with us.
Not counting the emergency & critical patients, we have many chronic/long term patients.
This just means no. of patient r always increasing. Again, resources r stretched when only patient load increases but not budget.
This just means no. of patient r always increasing. Again, resources r stretched when only patient load increases but not budget.
Private care for nephro is available but as it is a highly specialised unit, it is not cheap.
Dialysis costs about RM2000++ per month, per patient. Not many can afford to pay that, for years.
Dialysis costs about RM2000++ per month, per patient. Not many can afford to pay that, for years.
So we have many financial available to tap into, e.g JPA, Zakat, Baitumal, NGOs, etc.
But like I say, no. of patient going up, money is stagnant. There is basically no where to go.
But like I say, no. of patient going up, money is stagnant. There is basically no where to go.
Ok, that was a bit morbid. But I think that's the harsh reality of our healthcare.
The delivery is maxed out. Quality, mostly excellent because of our healthcare workers, but this system is not sustainable.
It will tip over one day if we do not manage it well.
The delivery is maxed out. Quality, mostly excellent because of our healthcare workers, but this system is not sustainable.
It will tip over one day if we do not manage it well.
With the arrival of the new Health Minister, I think many in the fraternity is hopeful (but still got some skeptics lah 😜) for a true reform of our system, from work culture to procurement system to budget.
There is much work to be done, for the healthcare workers, the system & most importantly, the wellbeing of patients.
I think I will choose to be hopeful. The work KKM does is exemplary, I'm proud to be part of it once. They are working miracles over there.
I think I will choose to be hopeful. The work KKM does is exemplary, I'm proud to be part of it once. They are working miracles over there.
Crap, rambling again. Ok I will end this.
Point is, the system is too fractured to say whether private or public is better. And for many like I said, they have no choice. I think we owe it to this segment of ppl to make it better.
Sekian, rambling saya malam ini.
Point is, the system is too fractured to say whether private or public is better. And for many like I said, they have no choice. I think we owe it to this segment of ppl to make it better.
Sekian, rambling saya malam ini.
As usual, I will take any questions, except kaunter pertanyaan sini sakit sana sakit type of questions 😜
Unroll @threadreaderapp