,
27 tweets,
6 min read
Read on Twitter
"Tweet storm" on the topic of albuminuria lowering as a surrogate endpoint and why it's a bad idea. As requested by @S_brimble
Fair warning this isn't going to be short.
Fair warning this isn't going to be short.
As this new paper, and it's 46 page supplement, were just released this rant will mainly focus on the prior SR & MA by some of the same authors (link below) as well as a look at the albuminuria lowering therapies evaluated since that time (2015).
jasn.asnjournals.org/content/26/8/2…
jasn.asnjournals.org/content/26/8/2…
Ideally what we want from a surrogate is to be able to evaluate a novel therapeutic agent using it's effect on the surrogate (albuminuria) to accurately predict it's effect on the clinical/patient important outcome (ESRD).
In the case of CKD albuminuria lowering is attractive as it could be evaluated with significantly less patients over a significantly shorter timeline.
To accept albuminuria lowering as a surrogate what we would like to see is that a VARIETY of interventions have consistently demonstrated a reduction in albuminuria and that the magnitude of albuminuria lowering consistently correlated with the effect on the outcome of ESRD.
In other words we want to see that the surrogate of albuminuria lowering is resistant to off-target effects. That there are really only good ways to lower albuminuria and not useless or harmful ways to reduce it.
For this purpose we need clinical trial data of lots of diverse interventions showing their effect on albuminuria as well as their effect on ESRD.
*foreshadowing*
An evidence base that is derived primarily from one intervention type simply will not do.
*foreshadowing*
An evidence base that is derived primarily from one intervention type simply will not do.
Here is the primary figure from the 2015 SR/MA. 

Impressive no? Looks like in nephrology our cup runneth over with interventions to substantially decrease our patients risk of ESRD and that they tend to also lower albuminuria!
Upon closer inspection:
14/21 trials were of RAAS inhibition
7/21 non-RAAS based interventions (2 intensive BP, 2 dietary protein restriction, 2 lipid lowering, 1 glycosaminoglycans)
14/21 trials were of RAAS inhibition
7/21 non-RAAS based interventions (2 intensive BP, 2 dietary protein restriction, 2 lipid lowering, 1 glycosaminoglycans)
Of those 7 trials a grand total of 1 demonstrated renoprotection (50% decline in GFR or ESRD in most cases).
That 1 trial was of strict BP control in children with CKD.
nejm.org/doi/full/10.10…
That 1 trial was of strict BP control in children with CKD.
nejm.org/doi/full/10.10…
Here is the same figure annotated with confidence intervals of the effect on clinical outcome for some of the non-RAAS interventions.
Effect estimates quite imprecise.
Effect estimates quite imprecise.

The authors state:
"A 30% reduction in albuminuria on top of guideline-recommended care seems necessary to confer a realistically detectable renoprotective treatment effect"
"A 30% reduction in albuminuria on top of guideline-recommended care seems necessary to confer a realistically detectable renoprotective treatment effect"
Let's see what wide variety of interventions we have with that effect on albuminuria....
Looks like only one intervention (ACEI/ARB) has the necessary albuminuria lowering effect to confer detectable clinical benefit.
Looks like only one intervention (ACEI/ARB) has the necessary albuminuria lowering effect to confer detectable clinical benefit.

Should we not require even one other intervention to demonstrate this surrogate - clinical outcome relationship to accept the surrogate?
Even one other intervention that had a large enough effect on the surrogate to show benefit?
One intervention does not validate a surrogate.
Even one other intervention that had a large enough effect on the surrogate to show benefit?
One intervention does not validate a surrogate.
In summary:
This is the relationship one intervention (ACEI/ARB) has between albuminuria lowering and ESRD ergo ALL interventions must have this same relationship!
I don't buy it.
This is the relationship one intervention (ACEI/ARB) has between albuminuria lowering and ESRD ergo ALL interventions must have this same relationship!
I don't buy it.
Since that time we have trials of the most potent albuminuria lowering agents to date, the endothelin receptor antagonists (ERA).
40-50% lowering of albuminuria! These must have improved clinical outcomes given their impressive effect on this great surrogate!
40-50% lowering of albuminuria! These must have improved clinical outcomes given their impressive effect on this great surrogate!
First up avosentan, an unselective ERA, in overt diabetic nephropathy.
The ASCEND trial:
jasn.asnjournals.org/content/21/3/5…
Over 40% albuminuria lowering! Stopped early due to increased fluid overload/CHF.
There is no surrogate for harm.
The ASCEND trial:
jasn.asnjournals.org/content/21/3/5…
Over 40% albuminuria lowering! Stopped early due to increased fluid overload/CHF.
There is no surrogate for harm.
Next up atrasentan. Atrasentan is a selective ERA chosen to hopefully avoid the side-effects of avosentan.
The study of diabetic nephropathy with atrasentan (SONAR) trial. This trial employed an interesting enrichment design selecting patients with the greatest albuminuria lowering (>30% reduction aka responders).
ncbi.nlm.nih.gov/pubmed/29405626
ncbi.nlm.nih.gov/pubmed/29405626
SONAR was billed to "further define whether albuminuria is a valid surrogate"
Over 3600 patients. Average eGFR ~40. Average UACR ~800 mg/g.
~50% albuminuria lowering in the nearly 2700 responders.
ncbi.nlm.nih.gov/pubmed/29604160
Over 3600 patients. Average eGFR ~40. Average UACR ~800 mg/g.
~50% albuminuria lowering in the nearly 2700 responders.
ncbi.nlm.nih.gov/pubmed/29604160
Results? Stopped ~4 months before the end of a nearly 5 year trial reportedly due to a lower than expected event rate.
news.abbvie.com/news/media-sta…
Full results expected to be published later this year.
news.abbvie.com/news/media-sta…
Full results expected to be published later this year.
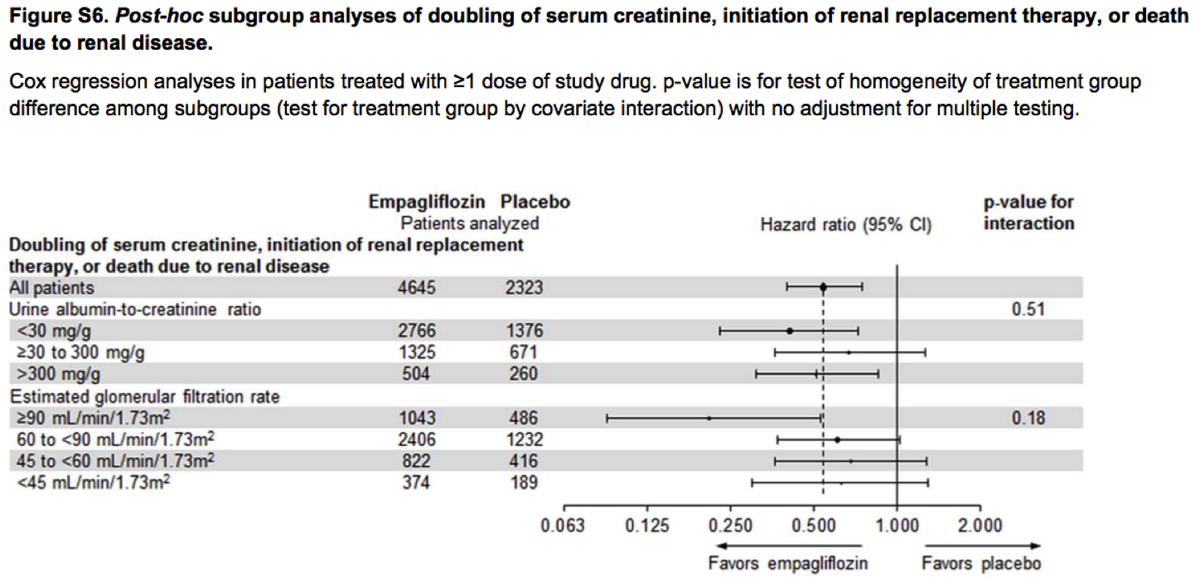
SGLT2 inhibitors show renoprotective benefit and ~20% albuminuria lowering
nejm.org/doi/full/10.10…
thelancet.com/journals/landi…
Renoprotective effect was in no way modified by albuminuria status. Albuminuria lowering was completely irrelevant to the clinical benefit.
nejm.org/doi/full/10.10…
thelancet.com/journals/landi…
Renoprotective effect was in no way modified by albuminuria status. Albuminuria lowering was completely irrelevant to the clinical benefit.
TL;DR
We do not have the intervention diversity necessary to accept albuminuria lowering as a surrogate outcome.
We have examples of interventions that lower proteinuria that can cause harm including dual RAAS blockade (ONTARGET, VA NEPHRON-D) as well as avosentan,....
We do not have the intervention diversity necessary to accept albuminuria lowering as a surrogate outcome.
We have examples of interventions that lower proteinuria that can cause harm including dual RAAS blockade (ONTARGET, VA NEPHRON-D) as well as avosentan,....
...interventions for which albuminuria lowering is irrelevant to clinical benefit (SGLT2 inhibitor trial info to date), and the intervention that lowers albuminuria to the greatest extent that has not demonstrated clinical benefit (SONAR trial).
But surely we can give provisional approval on the basis of albuminuria lowering with a commitment to post-approval studies?
Not exactly a track record of success there
ncbi.nlm.nih.gov/pubmed/28810023
ncbi.nlm.nih.gov/pubmed/28810023