More info
Prior dx of kidney stones on CT (6-8 mm, unknown type), managed medically. Has intermittent L flank pain. Last 2 days - f/c/n/v/back pain.
T 38.6 HR 98 BP 154/88 SpO2 99%
UA: 1+ blood, 3+ LE, WBC TNTC
+L CVA and suprapubic tenderness
WBC 18
Cr 1.6 (baseline 1.3)
2/
Prior dx of kidney stones on CT (6-8 mm, unknown type), managed medically. Has intermittent L flank pain. Last 2 days - f/c/n/v/back pain.
T 38.6 HR 98 BP 154/88 SpO2 99%
UA: 1+ blood, 3+ LE, WBC TNTC
+L CVA and suprapubic tenderness
WBC 18
Cr 1.6 (baseline 1.3)
2/
Pt admitted with a diagnosis of acute pyelonephritis and possible kidney stones and started on ceftriaxone. Foley was placed with difficulty but has drained 200 cc in the few minutes since placement
How specifically could POCUS help here? What POCUS question(s) exactly?
3/
How specifically could POCUS help here? What POCUS question(s) exactly?
3/
Poll here:
It is 8PM. What would be your approach to imaging (if POCUS unavailable)
(we will assume radiology staff not in house overnight, but could be called in)
4/
It is 8PM. What would be your approach to imaging (if POCUS unavailable)
(we will assume radiology staff not in house overnight, but could be called in)
4/
Tagging POCUS friends/prior participants! Branching out to a renal case so please tag others who may be interested
@SonoInternist @DRsonosRD @trobertson8 @G2Disrupt @IM_POCUS @buckeye_sanjay @benjikmathews @POCUS_Society @kyliebaker888 @CaseMcQuade @MedEdPGH @HeyDrNik @kkalra_22
@SonoInternist @DRsonosRD @trobertson8 @G2Disrupt @IM_POCUS @buckeye_sanjay @benjikmathews @POCUS_Society @kyliebaker888 @CaseMcQuade @MedEdPGH @HeyDrNik @kkalra_22
Prior to images, wanted to emphasize the idea of the "POCUS question" i.e what are we asking on POCUS, and will the answer help us? Some considerations
1) Is the exam literature-based as a point-of-care study
2) How would each possible finding change mgmt
More on this later
5/
1) Is the exam literature-based as a point-of-care study
2) How would each possible finding change mgmt
5/
Going to highlight the variation in approach to imaging (when POCUS unavailable) based on the poll currently. Probably need imaging (CT) but varying opinions on urgency.
The decision was made to perform POCUS to answer a focused question and guide mgmt, images as follows
6/
The decision was made to perform POCUS to answer a focused question and guide mgmt, images as follows
6/

Left kidney (first view)
7/
7/
L kidney (second view) - "1 view is no view" after all
8/
8/
Left kidney (third view) with color flow...
9/
9/
Looking a bit more closely... (left kidney 4th view)
10/
10/
Left kidney (5th view)
11/
11/
Right Kidney (fanning across in long axis)
12/
12/
Right kidney (fanning across in short axis)
13/
13/
Bladder (transverse)
14/
14/
Bladder (longitudinal)
15/
15/
Interpretations on those images?
How does this affect management (in the practical setting)?
What role does POCUS play in the case?
Limitations? Feedback on how to improve image quality?
16/
How does this affect management (in the practical setting)?
What role does POCUS play in the case?
Limitations? Feedback on how to improve image quality?
16/
Case wrap-up here:
POCUS interpretation:
L kidney: Mild to mod left hydro (absence of color flow helps confirm). Distended L ureter w possible stone at PUJ.
R kidney: no hydro seen
Bladder: foley in decompressed bladder. Small stones in bladder.
see annotated images here
17/
POCUS interpretation:
L kidney: Mild to mod left hydro (absence of color flow helps confirm). Distended L ureter w possible stone at PUJ.
R kidney: no hydro seen
Bladder: foley in decompressed bladder. Small stones in bladder.
see annotated images here
17/




These POCUS findings, in this clinical setting, led to a dx of obstructive urolithiasis with infection. CT A/P was performed, which confirmed ureter dilation and mild-mod left hydronephrosis. Interestingly, no stones were seen on CT. Urine cx grew E. coli (pan-sensitive)
18/
18/
Urology was consulted and performed cystoscopy/ureteroscopy, which did reveal a stone in the mid-distal ureter. The stone was extracted and noted to be ~1 cm calcium oxalate stone. Infection subsequently resolved with abx treatment.
19/
19/
Key points
1) When to obtain imaging in a pt with acute pyelo?
2) How do we grade hydronephrosis on POCUS?
3) How sens and spec is POCUS for hydronephrosis?
4) Is POCUS useful to r/o stone?
5) How do we integrate POCUS findings to affect dx in mgmt in this case?
20/
1) When to obtain imaging in a pt with acute pyelo?
2) How do we grade hydronephrosis on POCUS?
3) How sens and spec is POCUS for hydronephrosis?
4) Is POCUS useful to r/o stone?
5) How do we integrate POCUS findings to affect dx in mgmt in this case?
20/
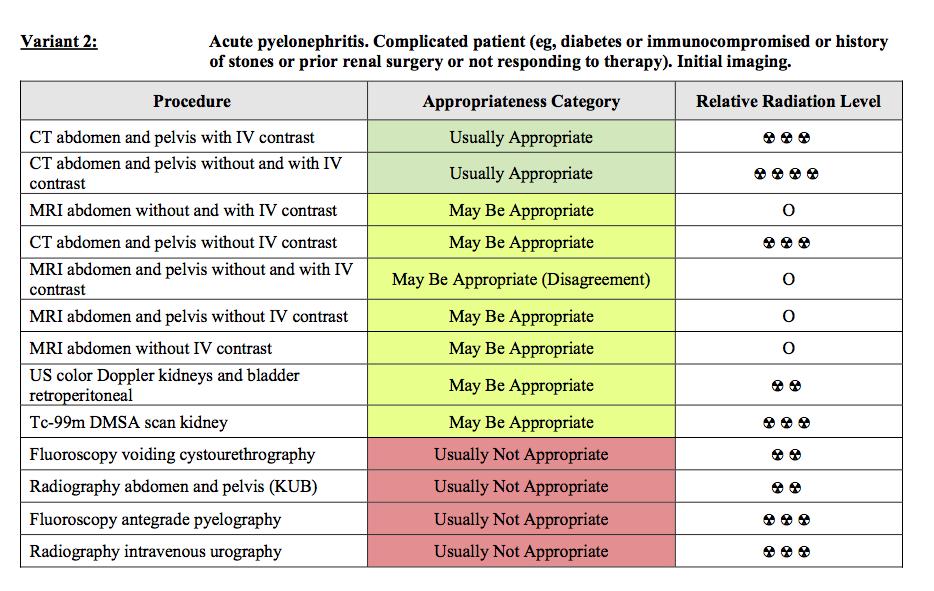
1) In general, imaging indicated if no response to therapy (>48-72 hrs) or complicating factor present ex: history of stone disease, immunocompromised (see tables from ACR appropriateness criteria)
21/
21/


3)
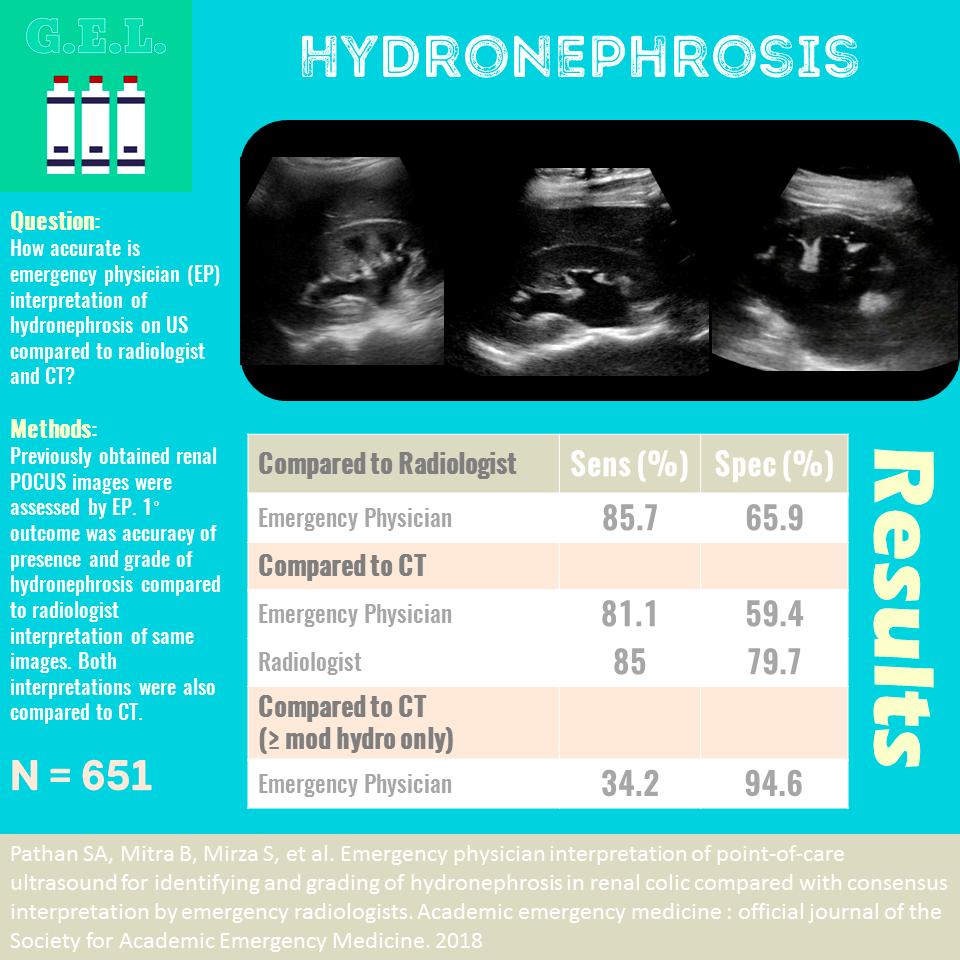
POCUS for hydronephrosis performed by IM residents had sens of >90% and spec of > 90% (ncbi.nlm.nih.gov/pubmed/24154905). Another study in the ED found sens 86% for any hydronephrosis and 66% spec (95% spec for moderate or greater hydronephrosis) - see image from ultrasound GEL
23/
POCUS for hydronephrosis performed by IM residents had sens of >90% and spec of > 90% (ncbi.nlm.nih.gov/pubmed/24154905). Another study in the ED found sens 86% for any hydronephrosis and 66% spec (95% spec for moderate or greater hydronephrosis) - see image from ultrasound GEL
23/
4/ Is POCUS useful for ruling out a stone? No. Review of ED POCUS for nephrolithiasis: sens ~70%, spec ~75% (journalfeed.org/article-a-day/…). However negative POCUS scans have been assoc with low rates of stone-related adverse events (0.4%) in ED patients nejm.org/doi/full/10.10…
24/
24/
5/ The most important point - Integration of POCUS findings in a case like this
Here is a proposed algorithm for this case, or perhaps for other similar cases. We welcome any comments on this.
25/
Here is a proposed algorithm for this case, or perhaps for other similar cases. We welcome any comments on this.
25/


Main conclusions:
- Remember to be clear on what exactly you are asking on POCUS, and how possible findings will impact your approach in the practical setting
-In this case presence or absence of hydronephrosis was most critical, and guided urgency of imaging and mgmt
26/
- Remember to be clear on what exactly you are asking on POCUS, and how possible findings will impact your approach in the practical setting
-In this case presence or absence of hydronephrosis was most critical, and guided urgency of imaging and mgmt
26/
We didn’t delve much into other possible findings: ex: emphysematous cystitis/pyelonephritis, fat stranding, etc… but we appreciate the comments on those and welcome all input.
27/
27/
Retagging POCUS friends for any and all thoughts on this... @SonoInternist @DRsonosRD @trobertson8 @G2Disrupt @IM_POCUS @buckeye_sanjay @benjikmathews @POCUS_Society @kyliebaker888 @CaseMcQuade @MedEdPGH @HeyDrNik @kkalra_22