
1/
Happy Monday everyone! We have a special case for you today written by UPMC PGY2 #POCUS enthusiast @MikeTao15.
A 52 yo M with hx of EtOH/HCV cirrhosis, VTE on Eliquis, HFrEF presents w worsening abd distention and pain. He is disoriented and unable to give much history.
Happy Monday everyone! We have a special case for you today written by UPMC PGY2 #POCUS enthusiast @MikeTao15.
A 52 yo M with hx of EtOH/HCV cirrhosis, VTE on Eliquis, HFrEF presents w worsening abd distention and pain. He is disoriented and unable to give much history.
2/
Cirrhosis previously complicated by esophageal varices, hepatic encephalopathy, and ascites. No follow up since last hospital admission at outside facility ~1 year ago. Has not been taking meds.
Vitals in the ED: Temp 38.1, HR 90, BP 98/70, Pulse Ox 96% on 2L
Cirrhosis previously complicated by esophageal varices, hepatic encephalopathy, and ascites. No follow up since last hospital admission at outside facility ~1 year ago. Has not been taking meds.
Vitals in the ED: Temp 38.1, HR 90, BP 98/70, Pulse Ox 96% on 2L
3/
He is lethargic, arousable to voice and oriented to self only
+scleral icterus
Cardiac + pulmonary exams normal
Abdomen distended, diffusely tender, no rebound/guarding
2+ b/l edema to thighs
Jaundiced, scattered ecchymoses
+asterixis
He is lethargic, arousable to voice and oriented to self only
+scleral icterus
Cardiac + pulmonary exams normal
Abdomen distended, diffusely tender, no rebound/guarding
2+ b/l edema to thighs
Jaundiced, scattered ecchymoses
+asterixis
4/
Labs (unkown baseline):
Na 129, Cr 2.2, Alb 2.8, Tbili 3.2, AST/ALT 140/160, ALP 310
WBC 2.1, Hb 7.4, Plt 80, INR 2.5
Blood cultures are collected. You go find your #POCUS and prepare for a diagnostic paracentesis.
Labs (unkown baseline):
Na 129, Cr 2.2, Alb 2.8, Tbili 3.2, AST/ALT 140/160, ALP 310
WBC 2.1, Hb 7.4, Plt 80, INR 2.5
Blood cultures are collected. You go find your #POCUS and prepare for a diagnostic paracentesis.
5/
Some polls while we're looking for our ultrasound machines.
How concerned are you for SBP in this patient? (poll)
Some polls while we're looking for our ultrasound machines.
How concerned are you for SBP in this patient? (poll)
6/
Would you start empiric abx at this point? (poll)
Would you start empiric abx at this point? (poll)
7/
What would you do with volume? (poll)
What would you do with volume? (poll)

10/
Now for our images!
RUQ
Now for our images!
RUQ
11/
RUQ zoomed in
RUQ zoomed in
12/
RUQ zoomed in further
RUQ zoomed in further
13/
Left upper quadrant
Left upper quadrant
14/
Subcostal. Do not have an IVC view available unfortunately
Subcostal. Do not have an IVC view available unfortunately
15/
Suprapubic
Suprapubic
16/
How would you characterize this patients ascitic fluid? (poll)
How would you characterize this patients ascitic fluid? (poll)
17/
How concerned are you for SBP or secondary peritonitis? (poll)
How concerned are you for SBP or secondary peritonitis? (poll)
18/
What would you do with volume? (poll)
What would you do with volume? (poll)
19/
What is your overall interpretation and next steps?
Pulling in our experts!
@TimRowesays @ArgaizR @Cometin007 @rogeralver @agraviersymmes @NephroP @DRsonosRD @laxswamy @DrGalenMD @cameron_baston @kyliebaker888 @RogerAlvarezDO @MikeRoseMDMPH @cianmcdermott @easypocus
What is your overall interpretation and next steps?
Pulling in our experts!
@TimRowesays @ArgaizR @Cometin007 @rogeralver @agraviersymmes @NephroP @DRsonosRD @laxswamy @DrGalenMD @cameron_baston @kyliebaker888 @RogerAlvarezDO @MikeRoseMDMPH @cianmcdermott @easypocus
22/
Alright, all. Time to wrap up!
#POCUS interpretation:
Diffuse complex free intraabdominal fluid in the right + left upper quadrants + pericolic gutter with visible fibrin stranding, plankton sign, and hematocrit sign
Simple right renal cyst, no hydronephrosis
Alright, all. Time to wrap up!
#POCUS interpretation:
Diffuse complex free intraabdominal fluid in the right + left upper quadrants + pericolic gutter with visible fibrin stranding, plankton sign, and hematocrit sign
Simple right renal cyst, no hydronephrosis
23/
The bladder is decompressed with Foley catheter seen
Tachycardia with regular rhythm is noted on subxiphoid view without any significant pericardial effusion. LV and RV function is difficult to assess based on these images, but grossly appears preserved
The bladder is decompressed with Foley catheter seen
Tachycardia with regular rhythm is noted on subxiphoid view without any significant pericardial effusion. LV and RV function is difficult to assess based on these images, but grossly appears preserved
24/
The patient was had progressive tachycardia to the 120s - 130s. Repeat CBC w downtrending Hgb to 6.2. Mental status worsened, transferred to the ICU and intubated for airway protection. He was resuscitated with pRBCs, plts, and FFP. General surgery consulted.
The patient was had progressive tachycardia to the 120s - 130s. Repeat CBC w downtrending Hgb to 6.2. Mental status worsened, transferred to the ICU and intubated for airway protection. He was resuscitated with pRBCs, plts, and FFP. General surgery consulted.
25/
Pt went to OR for ex lap and bloody ascitic fluid was found but no source of bleeding identified. Bleeding resolved with resuscitation and after a prolonged hospital course pt eventually recovered and was discharged.
Final Diagnosis: Hemoperitoneum, etiology unclear.
Pt went to OR for ex lap and bloody ascitic fluid was found but no source of bleeding identified. Bleeding resolved with resuscitation and after a prolonged hospital course pt eventually recovered and was discharged.
Final Diagnosis: Hemoperitoneum, etiology unclear.
26/
Thought-Provoking Questions from this case:
1) What are features on POCUS that would distinguish complex vs simple ascitic fluid?
2) What are ultrasonographic findings of complex fluid? Is there literature behind this?
3) What was the role of POCUS in this case?
Thought-Provoking Questions from this case:
1) What are features on POCUS that would distinguish complex vs simple ascitic fluid?
2) What are ultrasonographic findings of complex fluid? Is there literature behind this?
3) What was the role of POCUS in this case?
27/
1) Simple vx. complex ascitic fluid
Broadly, ascitic fluid can be characterized as transudative - typically homogenously anechoic - or exudative - can be anechoic or complex. Complex fluid may present with debris, internal septations, and loculated collections.
1) Simple vx. complex ascitic fluid
Broadly, ascitic fluid can be characterized as transudative - typically homogenously anechoic - or exudative - can be anechoic or complex. Complex fluid may present with debris, internal septations, and loculated collections.
28/
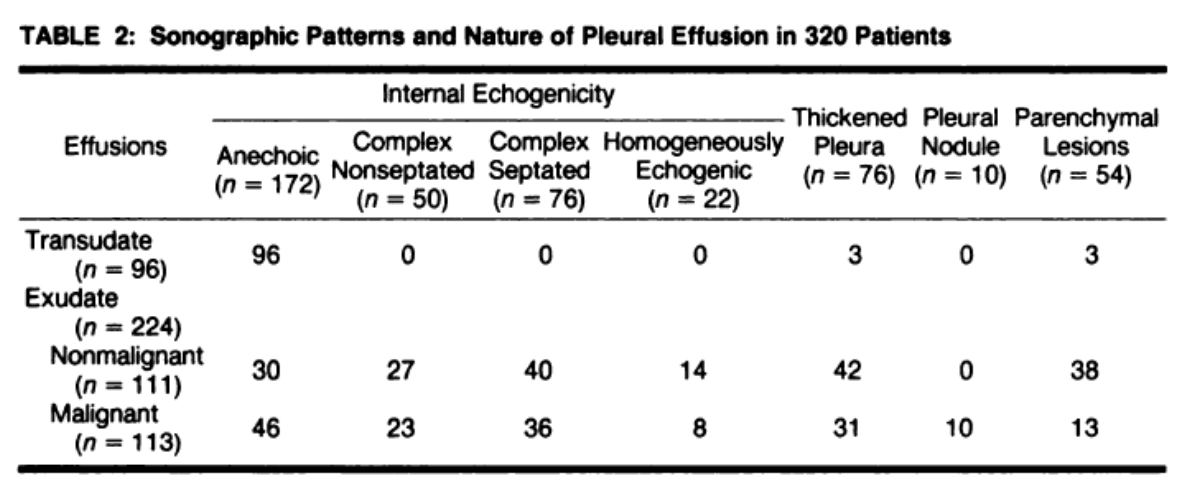
To our knowledge, most studies on complex vs simple fluid, like @cameron_baston said, are older and on pleural fluid, such as ajronline.org/doi/pdf/10.221…, + conclude that complex effusions are almost always exudates whereas simple effusions can be transudate OR exudate.
To our knowledge, most studies on complex vs simple fluid, like @cameron_baston said, are older and on pleural fluid, such as ajronline.org/doi/pdf/10.221…, + conclude that complex effusions are almost always exudates whereas simple effusions can be transudate OR exudate.
29/
An article by Rudralingam et al - ncbi.nlm.nih.gov/pmc/articles/P… - presents a nice case series describing different types of ascites and comes to a similar conclusion - complex fluid may be useful to help rule IN an exudative process.
An article by Rudralingam et al - ncbi.nlm.nih.gov/pmc/articles/P… - presents a nice case series describing different types of ascites and comes to a similar conclusion - complex fluid may be useful to help rule IN an exudative process.
30/
2) So, what are the #POCUS findings of complex fluid?
The “plankton sign” and “hematocrit sign” are two sonographic findings that have been reported.
Plankton sign reveals echogenic cellular debris that swirl as a result of respiratory motion and vascular pulsations.
2) So, what are the #POCUS findings of complex fluid?
The “plankton sign” and “hematocrit sign” are two sonographic findings that have been reported.
Plankton sign reveals echogenic cellular debris that swirl as a result of respiratory motion and vascular pulsations.
31/
And the Hematocrit sign forms due to layering of denser, echogenic materials as a result of gravity with these materials collecting at the most dependent locations.
And the Hematocrit sign forms due to layering of denser, echogenic materials as a result of gravity with these materials collecting at the most dependent locations.

32/
3) So how did #POCUS help in this case?
Without much data to support this beyond what we have described above (please post studies or thoughts if you have them!), we think of complex fluid as useful for ruling IN a more complex process
3) So how did #POCUS help in this case?
Without much data to support this beyond what we have described above (please post studies or thoughts if you have them!), we think of complex fluid as useful for ruling IN a more complex process
33/
That is, the presence of hematocrit sign, septations, or fibrin stranding significantly increases our suspicion for an alternate process like SBP or hemoperitoneum, but the absence of these signs wouldn’t rule this out, as we all know how tricky it can be to diagnose SBP.
That is, the presence of hematocrit sign, septations, or fibrin stranding significantly increases our suspicion for an alternate process like SBP or hemoperitoneum, but the absence of these signs wouldn’t rule this out, as we all know how tricky it can be to diagnose SBP.
34/
In this case, POCUS increased the urgency for surgical consultation and helped triage the patient more quickly than we may have without POCUS. Likely he would have received abx regardless. We will pull in this algorithm we created from a prior case:
In this case, POCUS increased the urgency for surgical consultation and helped triage the patient more quickly than we may have without POCUS. Likely he would have received abx regardless. We will pull in this algorithm we created from a prior case:

35/
Thanks all for your wise thoughts and insights as always!
Pulling back in our participants.
@cameron_baston @TimRowesays @ThinkingCC @ssrasm
@NephroP @jtanguay11 @jminardi21 @ScottBiggersta1 @buckeye_sanjay
Please pull in anyone we missed.
Happy #POCUS-ing
Thanks all for your wise thoughts and insights as always!
Pulling back in our participants.
@cameron_baston @TimRowesays @ThinkingCC @ssrasm
@NephroP @jtanguay11 @jminardi21 @ScottBiggersta1 @buckeye_sanjay
Please pull in anyone we missed.
Happy #POCUS-ing















