A thread:
Given recent news about prosecuting people across the UK for surviving suicide attempts, it's worth considering whether and when (if ever) clinical psychologists, psychiatrists and psychiatric nurses should endorse, encourage or incite prosecution as a clinical decision
Given recent news about prosecuting people across the UK for surviving suicide attempts, it's worth considering whether and when (if ever) clinical psychologists, psychiatrists and psychiatric nurses should endorse, encourage or incite prosecution as a clinical decision
Firstly it is worth starting with the codes of ethics & conduct
Clinical psychologists: "Promote & protect the interests of service users & carers"
Psychiatrists: "Make the care of your patient your first concern"
Psychiatric nurses: "Prioritise people"
Clinical psychologists: "Promote & protect the interests of service users & carers"
Psychiatrists: "Make the care of your patient your first concern"
Psychiatric nurses: "Prioritise people"
Next, frame the question. Decisions to charge are made by police. Decisions to prosecute by the Crown Office & Procurator Fiscal Service, the Public Prosecution Service or the Crown Prosecution Service. Psychologists, psychiatrists & nurses can encourage or dissuade prosecution
Expert opinion can be powerful in guiding the actions of COPFS/PPS/CPS. Given that the primary duty of clinical psychologists, psychiatrists & psychiatric nurses is to improve wellbeing of our patients, this must be the primary framing of any question re: encouraging prosecution
So framing the question in clinical terms is something like:
Do the clinical benefits of clinical psychologists, psychiatrists & psychiatric nurses encouraging the prosecution of suicide attempt survivors outweigh the harms of doing so?
Do the clinical benefits of clinical psychologists, psychiatrists & psychiatric nurses encouraging the prosecution of suicide attempt survivors outweigh the harms of doing so?
Known harms of CPs, Drs &nurses encouraging prosecution of suicide attempt survivors include:
Death
Lifelong psychological harm
Criminal record
Loss of career
Financial loss
Family/relationship breakdown
Irretrievable loss of trust in MH staff leading to exclusion from treatment
Death
Lifelong psychological harm
Criminal record
Loss of career
Financial loss
Family/relationship breakdown
Irretrievable loss of trust in MH staff leading to exclusion from treatment
We know that all of these harms occur by listening to survivors of CPs, Drs & nurses encouraging prosecution for attempting suicide. We know less about the benefits. Are those who have benefitted from being prosecuted less likely to talk about it or less likely to exist?
I could do with some help to frame the potential benefits of CPs, Drs & nurses encouraging the prosecution of suicide attempt survivors. Perhaps there are four main categories:
Clinical/symptom outcomes
Patient experience of health services
Service use
Social/functional outcomes
Clinical/symptom outcomes
Patient experience of health services
Service use
Social/functional outcomes
I'd also be grateful if anyone can point me towards research into potential benefits of CPs, Drs & nurses encouraging prosecution for attempting suicide. I'm not familiar with the literature here & would be interested to see whether any research has found benefits (I suspect not)
So a quick dirty PubMed searches for (Suicide AND prosecution) and for ("criminal law"[MeSH Major Topic] AND "suicide"[MeSH Major Topic]) turns up three relevant papers, none of which report benefits to patients of being prosecuted for having attempted suicide
The first paper looks at people criminalised for attempting suicide in Ghana and is mostly about the characteristics of the people and the penalties they suffered - not really designed to report on benefits
This paper on criminalising suicide attempts in Abu Dhabi investigates the specific harm of making people unwilling to disclose information to mental health staff, and finds an association with being charged
This paper doesn't directly examine outcomes but surveys professionals on whether attempting suicide should remain criminalised in Ghana. The majority believe attempting suicide should not be criminalised but a minority believe there might be a deterrent effect
So as far as I can see, there is no evidence that clinical psychologists, psychiatrists or psychiatric nurses encouraging the prosecution of people for attempting suicide helps patients or improves clinical outcomes in any way.
Absolutely none
Absolutely none
There is another harm which we know has resulted from clinical psychologists, psychiatrists and psychiatric nurses encouraging the prosecution of suicide attempt survivors:
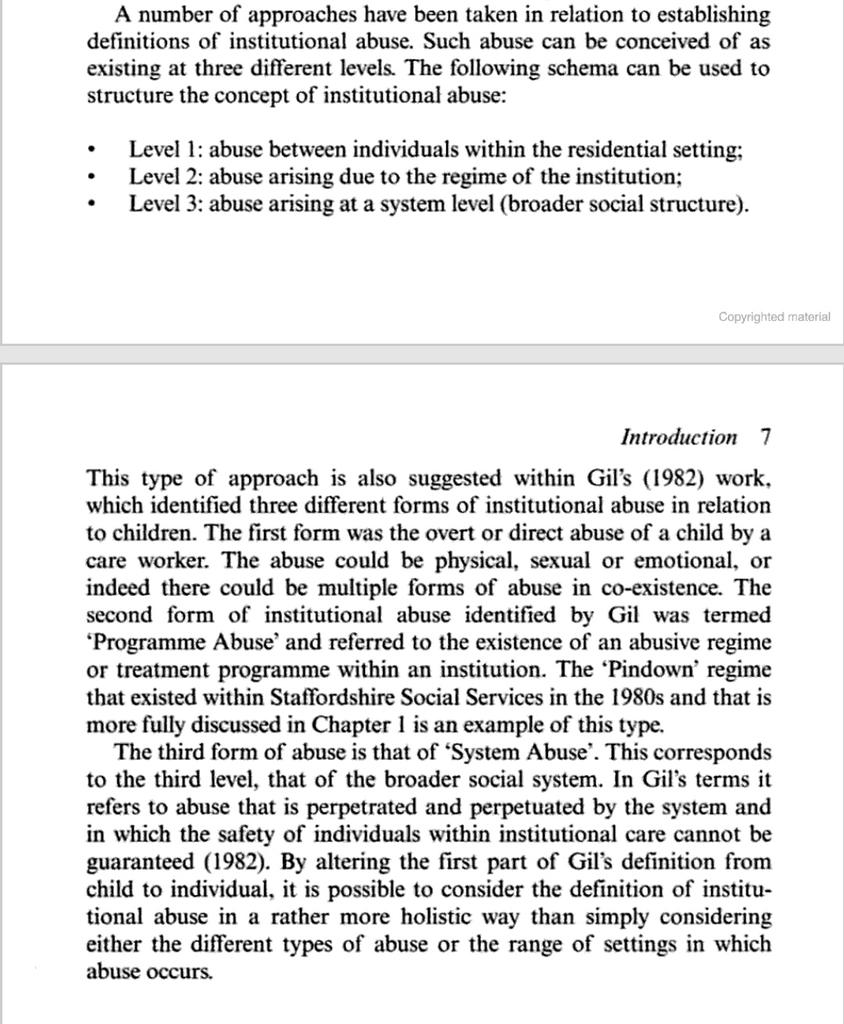
Level 3 institutional abuse
Level 3 institutional abuse
Institutional abuse can be conceptualised at three levels:
Level 1 - direct abuse of patients by individual staff (verbal/emotional/physical/sexual etc)
Level 2 - abusive regimes (enabling level 1 abuse / deliberate & vexatious exclusion etc)
Level 1 - direct abuse of patients by individual staff (verbal/emotional/physical/sexual etc)
Level 2 - abusive regimes (enabling level 1 abuse / deliberate & vexatious exclusion etc)
Level 3 institutional abuse is 'System abuse' - when the broader societal structures designed to safeguard vulnerable people fail to detect & stop abuse, and instead perpetrate & perpetuate further abuse
If a person attempts suicide as a consequence either of abusive acts, or of deliberate & vexatious exclusion leading to a failure to treat a mental illness, then prosecuting that person is 'System Abuse' - a failure of police & safeguarding services to detect & stop that abuse
So if there are no known clinical benefits of CPs, Drs & nurses encouraging prosecution for attempting suicide, and countless known harms, what of /theoretical/ benefits? Could prosecution improve clinical outcomes & wellbeing? I am struggling to envisage a mechanism here
If one were to argue that enforcing treatment for mental illnesses by means of prosecution leads to improved symptom reduction & wellbeing, one would need to demonstrate this, and demonstrate that prosecution is superior to non-criminal compulsory treatment under MHCTA/MHA/MHO
A crucial clinical outcome measure in psychiatry is service user experience - indeed my subspecialty it is arguably the most important outcome. Is there a /theoretical/ mechanism whereby a CP, Dr or nurse encouraging prosecution for attempting suicide improves patient experience?
The Friends & Family Test is a crude measure of patient experience but I can't imagine anyone endorsing it: "Would you recommend that any of your friends or family go through your experience of being prosecuted after attempting suicide?" Answering "Yes" doesn't seem plausible
Service use is often cited as a clinical outcome but I would caution against its use as a primary outcome. There is no clear relationship between service use and wellbeing or symptom reduction, which should be primary outcomes
It is indeed plausible that encouraging prosecution for attempting suicide may reduce service use without improving wellbeing by deterring help-seeking. The opposite is equally plausible: losing trust in treatment leading to an increased frequency of psychiatric emergencies
Any CP, Dr or nurse asserting that encouraging prosecution of suicide attempt survivors is beneficial in reducing service use would need to demonstrate:
1 This is true, in at least a robust observational study
2 It is not occurring at the expense of wellbeing or clinical symptoms
1 This is true, in at least a robust observational study
2 It is not occurring at the expense of wellbeing or clinical symptoms
So the last outcome area that could be examined for clinical benefits of clinical psychologists, psychiatrists and psychiatric nurses encouraging the prosecution of their patients who attempt suicide is social/functional outcomes:
Employment
Housing
Relationships
Raising children
Employment
Housing
Relationships
Raising children
Does the encouragement of prosecution for attempting suicide lead to increased employment rates?
Does the encouragement of prosecution for attempting suicide improve security of housing?
Does the encouragement of prosecution for attempting suicide keep families together?
Does the encouragement of prosecution for attempting suicide improve security of housing?
Does the encouragement of prosecution for attempting suicide keep families together?
Once again, a theoretical improvement in social/functional status seems implausible as a potential benefit of CPs, Drs & nurses encouraging prosecution of people in relation to feeling suicidal or attempting suicide
A digression: it's been pointed out l that the act of suicide itself is no longer an offence under UK law. It was never an offence in Scotland, was decriminalised in England & Wales in 1961, & in 1966 in Northern Ireland, so strictly speaking people aren't charged with 'Suicide'
I should also emphasise that I am NOT discussing whether or not the police & COPFS/PPS/CPS should charge people with offences related to being suicidal where there is no danger to others, but specifically whether mental health staff should encourage or support such actions
Disclosing thoughts of suicide, attempting suicide & associated acts with no danger to others can be seen as "Breach of the Peace" - here are the definitions for England/Wales/Northern Ireland & for Scotland
en.m.wikipedia.org/wiki/Breach_of…
en.m.wikipedia.org/wiki/Breach_of…
This means that if a person discloses suicidal thoughts to a police officer, or if MH staff disclose info about their patient to a police officer, and that info "causes alarm" to the police officer, technically a breach of the peace has occurred and can be charged & prosecuted
So to summarise the clinical benefits and harms of clinical psychologists, psychiatrists and psychiatric nurses encouraging police to charge people with offences relating to being suicidal:
There is no reported clinical benefit
There are substantial known & demonstrable harms
There is no reported clinical benefit
There are substantial known & demonstrable harms
Known harms of CPs/Drs/nurses encouraging prosecution for offences related to being suicidal:
Death
Lifelong psychological harm
Criminal record
Loss of career
Financial loss
Family/relationship breakdown
Irretrievable loss of trust in MH staff leading to exclusion from treatment
Death
Lifelong psychological harm
Criminal record
Loss of career
Financial loss
Family/relationship breakdown
Irretrievable loss of trust in MH staff leading to exclusion from treatment
Further harms include:
And
...and also level 3 institutional abuse, or system abuse
So should clinical psychologists, psychiatrists and psychiatric nurses promote an intervention which carries risk of serious harm or even death?
In health care this is done all the time: aortic aneurysm repair, cancer surgery, many drug treatments etc.
In health care this is done all the time: aortic aneurysm repair, cancer surgery, many drug treatments etc.
So health care involves tough decisions and interventions which might risk death or save life. When a midwife or obstetrician makes decisions about cesarean, induction etc. she is doing so with knowledge of the risks & benefits of each course of action from research
Can this apply here? Given the primary duty of clinical psychologists, psychiatrists and psychiatric nurses is the welfare of patients, is encouraging prosecution of our patients for offences associated with suicide consistent with our ethics & standards?
If there were overwhelming evidence of benefit for the majority of people who are prosecuted for offences related to being suicidal, then CPs, Drs & nurses would be justified in encouraging this as an intervention
...provided the benefits greatly outweigh the harms. If hundreds of people benefited from being prosecuted for every death, every missed case of institutional abuse, every degradation, every ruined career, every lifelong trauma, could we justify encouraging this? Perhaps we could
Is there any evidence of benefit from CPs, Drs & nurses encouraging prosecution for offences related to being suicidal?
No
Is there evidence of harm?
Yes
Do we know the rate of harm?
No
Can we justify this intervention on the grounds of benefits outweighing harms?
No.
No
Is there evidence of harm?
Yes
Do we know the rate of harm?
No
Can we justify this intervention on the grounds of benefits outweighing harms?
No.
Are there any other considerations here? How about criminal culpability?
This is a matter for the police & courts. As a CP, Dr or nurse, if you opine on culpability you are outside the bounds of both your competence & ethics, thereby jeopardising your professional registration
This is a matter for the police & courts. As a CP, Dr or nurse, if you opine on culpability you are outside the bounds of both your competence & ethics, thereby jeopardising your professional registration
How about 'enforcing boundaries'?
Unless you can demonstrate:
1 A robust theoretical framework
2 Evidence of benefits which vastly outweigh the harms
...this amounts to nothing more than pseudopsychoanalytic theorising & again you are jeopardising your professional registration
Unless you can demonstrate:
1 A robust theoretical framework
2 Evidence of benefits which vastly outweigh the harms
...this amounts to nothing more than pseudopsychoanalytic theorising & again you are jeopardising your professional registration
How about 'people need to take responsibility / face the consequences of their actions'?
This is squarely outside the ethics & standards frameworks of the HCPC, NMC & GMC. It is very close to moral judgement & advocating punishment- not the professional role of a CP, Dr or nurse
This is squarely outside the ethics & standards frameworks of the HCPC, NMC & GMC. It is very close to moral judgement & advocating punishment- not the professional role of a CP, Dr or nurse
How about 'prosecuting a person is the only way to get them a service'?
We have already established that prosecution has no benefits & substantial harms. If commissioners or MH staff are excluding a person from help, it is those people who should be prosecuted, not their patient
We have already established that prosecution has no benefits & substantial harms. If commissioners or MH staff are excluding a person from help, it is those people who should be prosecuted, not their patient
So back to the original question:
when (if ever) is it clinically justified for clinical psychologists, psychiatrists and psychiatric nurses to endorse, encourage or incite prosecution for offences associated with attempting suicide or being suicidal?
when (if ever) is it clinically justified for clinical psychologists, psychiatrists and psychiatric nurses to endorse, encourage or incite prosecution for offences associated with attempting suicide or being suicidal?
Given that there is no evidence of clinical benefit from prosecution
Given that the harms are substantial, permanent or even fatal
Given that other considerations are outside the ethics &duties of clinical psychologists, psychiatrists & psychiatric nurses
The answer is "Never"
Given that the harms are substantial, permanent or even fatal
Given that other considerations are outside the ethics &duties of clinical psychologists, psychiatrists & psychiatric nurses
The answer is "Never"
This thread has become a bit of an epic! I've been busy with fun things this morning but might come back to one more question: what are the duties of CPs, Drs & nurses if their patient might be charged with breach of the peace or similar for being suicidal