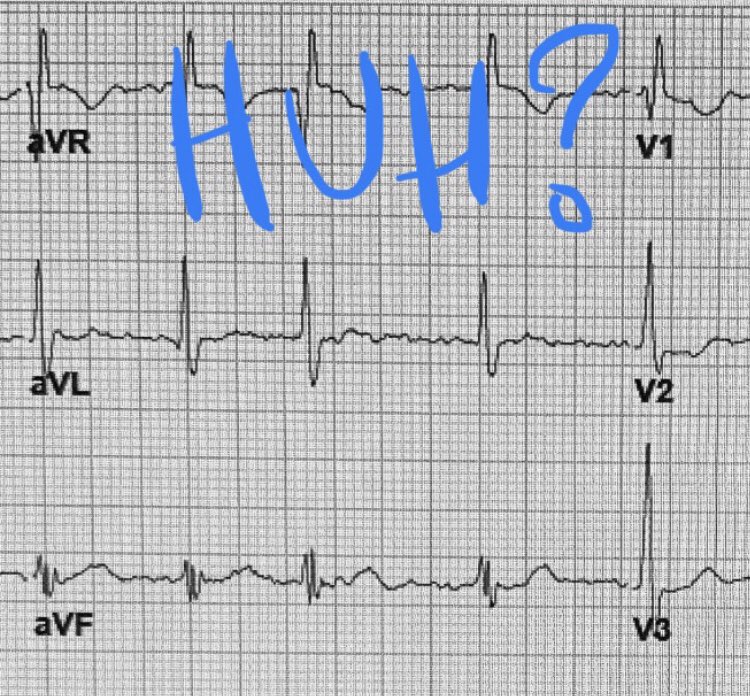
What’s up with lead aVR?
Many seem to ignore it.
Others get really excited and start saying scary things about the left main coronary.
Let’s try to demystify.
#Tweetorial 1/
Many seem to ignore it.
Others get really excited and start saying scary things about the left main coronary.
Let’s try to demystify.
#Tweetorial 1/
Directed up and to the right, aVR points opposite most of the LV and away from most leftward + downward pointing leads, like I, II, F, aVL, V5, V6.
2/
2/
Thus it can reflect processes occurring in big segments of the LV, showing the opposite/reciprocal of those electrical patterns.
aVR STE = often reflection of “everything-else” STD.
aVR STD = often reflection of “everything-else” STE.
3/
aVR STE = often reflection of “everything-else” STD.
aVR STD = often reflection of “everything-else” STE.
3/
For instance, complete LM occlusion would cause transmural injury current (ST elevation) from the anterior and lateral LV walls, and might result in an aVR with reciprocal STD.
You don’t see many ECGs like that because acute complete LM occlusion = code.
4/
You don’t see many ECGs like that because acute complete LM occlusion = code.
4/
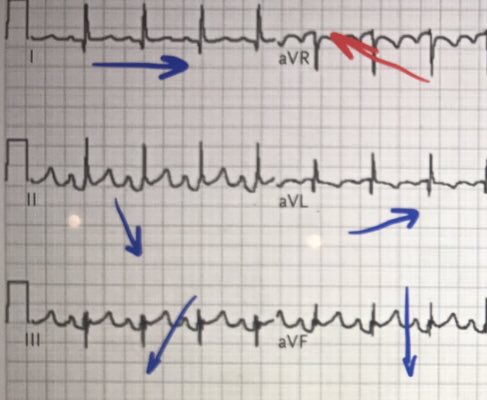
More commonly, you see something like this ECG:
Subendocardial ischemia of most of the LV ->
Injury current causing STD in anterolateral and inferior leads (except III*) ->
aVR with reciprocal STE.
5/
Subendocardial ischemia of most of the LV ->
Injury current causing STD in anterolateral and inferior leads (except III*) ->
aVR with reciprocal STE.
5/

But the CAUSE of subendocardial ischemia of LV remains a question.
- a SUB-total occlusion ACS of LM or proximal LAD could do it
- but so could non-ACS-related supply/demand mismatch e.g. hypotension, rapid arrhythmia, stress test, etc
6/
- a SUB-total occlusion ACS of LM or proximal LAD could do it
- but so could non-ACS-related supply/demand mismatch e.g. hypotension, rapid arrhythmia, stress test, etc
6/
Different scenario to demo same concept of opposite vectors:
In this ECG with pericarditis, why are there STE “everywhere” but STD in aVR? PR depressions everywhere but PR elevation in aVR.
Turn aVR upside down. It will look a lot like II, no matter what’s going on.
7/
In this ECG with pericarditis, why are there STE “everywhere” but STD in aVR? PR depressions everywhere but PR elevation in aVR.
Turn aVR upside down. It will look a lot like II, no matter what’s going on.
7/

I won’t quote test characteristics; the narrow contexts of most studies make the numbers hard to generalize. But for those interested, this review has those references.
bit.ly/2mzvWQB
8/
bit.ly/2mzvWQB
8/
Oh, the * from 5/ above...
Why is the ST segment in III often isoelectric or even elevated in diffuse subendocarial ischemia?
Rightward direction of III makes it reflect reciprocal currents from lateral wall in addition to showing the inferior wall.
9/
Why is the ST segment in III often isoelectric or even elevated in diffuse subendocarial ischemia?
Rightward direction of III makes it reflect reciprocal currents from lateral wall in addition to showing the inferior wall.
9/
And sometimes these cancel out.
Here’s another EKG with subendo ischemia of most of LV including inferior wall.
STD anterolateral leads, II, F. Big reciprocal STE in aVR. But III is isoelectric to slightly elevated.
10/
Here’s another EKG with subendo ischemia of most of LV including inferior wall.
STD anterolateral leads, II, F. Big reciprocal STE in aVR. But III is isoelectric to slightly elevated.
10/

Parting thought, with the caveat that I clearly enjoy thinking about aVR, and it CAN be a useful additional angle:
Most of the time when I see non-cardiologists focusing/relying on aVR to make a diagnosis, they’re not looking hard enough at the other leads.
11/
Most of the time when I see non-cardiologists focusing/relying on aVR to make a diagnosis, they’re not looking hard enough at the other leads.
11/