Alright #medTwitter and #medstudenttwitter, time for an Introduction to EKG #tweetorial 🙌🏽 full of GIFs, pearls & fun!
We are going to start off w/ some key principles and get all the way to the basics of a 12-lead #EKG!
1/28
We are going to start off w/ some key principles and get all the way to the basics of a 12-lead #EKG!
1/28
First— just as YOU see an EKG, the EKG “sees” the heart! Only, since it’s paper and not smart, it needs many more “eyes” than you do.
Every EKG lead is an eye (electrode) that is seeing the heart’s electricity from its own perspective.
These are the EKGs 12 eyes:
2/28
Every EKG lead is an eye (electrode) that is seeing the heart’s electricity from its own perspective.
These are the EKGs 12 eyes:
2/28

If an electrical signal from the heart is moving toward one of the leads, in the directions the arrows are pointing, it will show up as an upward i.e positive deflection on the EKG.
“So like a P-wave?” Yeah! Exactly!
But how?
3/28
“So like a P-wave?” Yeah! Exactly!
But how?
3/28
As electricity moves from the SA node to the AV node and contracts the atria, the electricity moves in a direction toward lead II and registers as a P-wave.
Now, break down the electricity moving toward lead II in its X and Y components - what ELSE does the EKG see?
4/28
Now, break down the electricity moving toward lead II in its X and Y components - what ELSE does the EKG see?
4/28

There’s an X component that is going toward lead I, so lead I will also be positive, but this X part is also going AWAY from aVR! Now what?
Away from the electrode registers as a downward i.e NEGATIVE deflection on the EKG!
So the P-wave will be negative in aVR!
5/28
Away from the electrode registers as a downward i.e NEGATIVE deflection on the EKG!
So the P-wave will be negative in aVR!
5/28
Ok, but what about V1? Well, V1 is in the Z axis, what’s the atrial contraction like in 3D space?
To V1, the SA node is slightly posterior to the AV node (remember, the right side of the heart is anterior), and the right atrium contracts before the left atrium does...WAH?!
6/28
To V1, the SA node is slightly posterior to the AV node (remember, the right side of the heart is anterior), and the right atrium contracts before the left atrium does...WAH?!
6/28

🤯, you got this! Putting it all together: the direction of the right atrium contracting first w/ electricity moving from the SA to the AV is TOWARD V1, and this is anterior to the left atrium, which then goes second, and...AWAY from V1 (left atrium is posterior!)
7/28
7/28
So....two directions, 1 lead, and no boy bands?! Yup 😎
The P-wave in V1 is biphasic! The first 1/2 of the wave registers the toward V1 right atrial electricity, the second 1/2 registers the away from V1 left atrial electricity!
Normal P-wave in lead II and V1:
8/28
The P-wave in V1 is biphasic! The first 1/2 of the wave registers the toward V1 right atrial electricity, the second 1/2 registers the away from V1 left atrial electricity!
Normal P-wave in lead II and V1:
8/28

Now you got it!
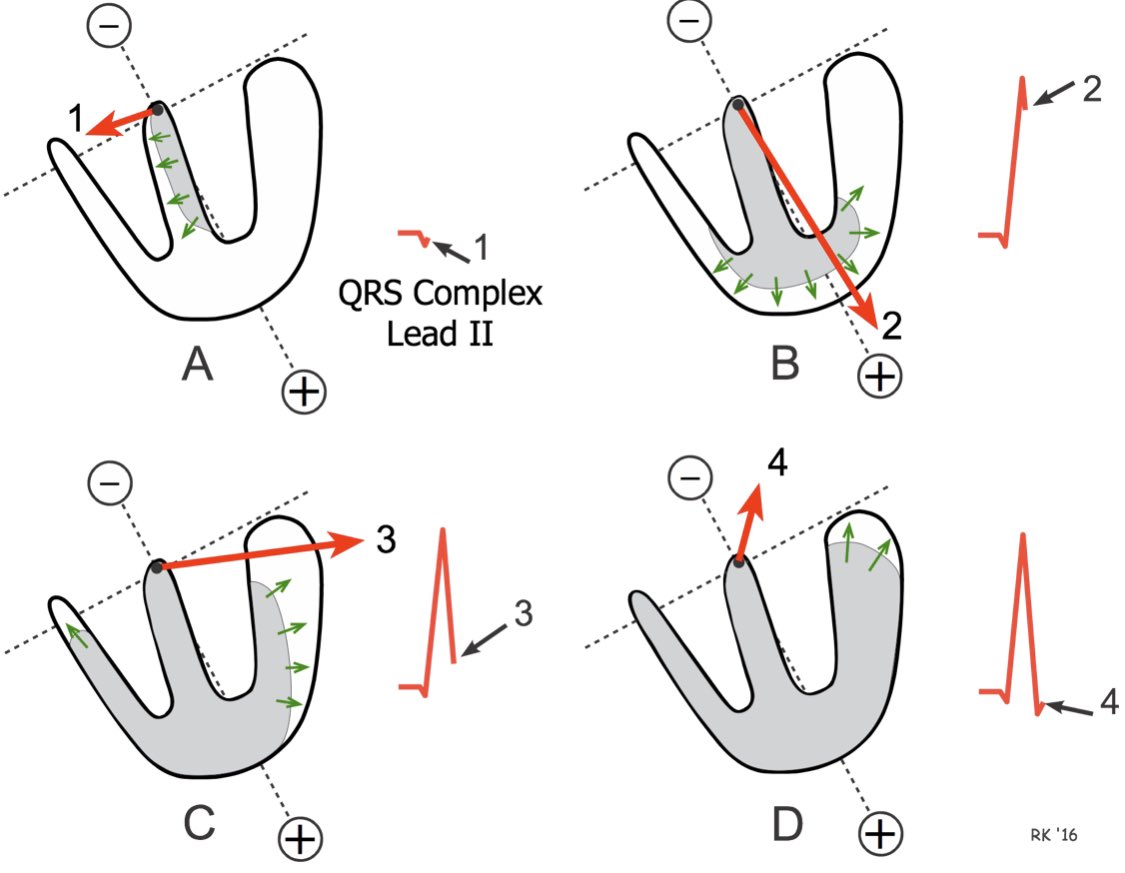
For the ventricles, below image from cvphysiology.com is 🔥.
- image is from lead II’s perspective
- red top arrow is the overall direction of electricity
- why L to R electricity of the septum? The L bundle of His is faster!
9/28
For the ventricles, below image from cvphysiology.com is 🔥.
- image is from lead II’s perspective
- red top arrow is the overall direction of electricity
- why L to R electricity of the septum? The L bundle of His is faster!
9/28
Now, the atria and ventricles have contracted ie DEpolarized (DEpol) and they gave us the P-wave and the QRS complexes, so what is the T-wave and why is it...positive?
The T-wave represents REpolarization (REpol) or “resetting” of the cardiac myocytes!
10/28
The T-wave represents REpolarization (REpol) or “resetting” of the cardiac myocytes!
10/28
The normal cardiac myocyte is negative and rests at approximately -90 mV (important later). When the myocytes DEpol, they become positive, and this positive wave spreads toward positive electrodes causing positive deflections, what happens when they REpol?
11/28
11/28
The myocytes become negative again! And this NEGATIVE wave of electricity goes AWAY from the positive electrodes because REpol happens basically in reverse of DEpol.
The LAST myocytes to DEpol are the FIRST to REpol!
Why?
12/28
The LAST myocytes to DEpol are the FIRST to REpol!
Why?
12/28
The myocytes closest to the subendocardium are bigger and thicker and take longer to depolarize! The ones closest to the epicardium depolarize VERY quickly and IMMEDIATELY begin REpolarizing.
The REpol wave is from the epicardium toward the myocardium, out to in!
13/28
The REpol wave is from the epicardium toward the myocardium, out to in!
13/28

So, from the perspective of our electrode:
- with DEpolarization, positive charges were coming toward it and it registers positive on the EKG
- with REpolarization, negative charges are going AWAY from it, which means our electrode feels positive still!
14/28
- with DEpolarization, positive charges were coming toward it and it registers positive on the EKG
- with REpolarization, negative charges are going AWAY from it, which means our electrode feels positive still!
14/28
Thus, our T-wave, which represents REpolarization (of the ventricles - the atrial repolarization was happening during ventricular DEpol and the atrial REpol wave got lost in that mess because the ventricles > atria) is positive too since the negative wave is going AWAY!
15/28
15/28
ALRIGHT, GO YOU! GIVE YOURSELF A HIGH FIVE, A HUG, AND A SNACK! Now comes the fun stuff!
#celebrate #littleVictories #growthMindset
What do det ischemia do doe?
16/28
#celebrate #littleVictories #growthMindset
What do det ischemia do doe?
16/28
Ischemia is hypoxia because of clot or supply-demand mismatch.
Not enough O2 messes with our bodies ability to make ATP.
In the heart, and elsewhere, not enough ATP makes the Na-K-ATPase less functional.
Remember how the cardiac myocyte rests at -90 mV?
17/28
Not enough O2 messes with our bodies ability to make ATP.
In the heart, and elsewhere, not enough ATP makes the Na-K-ATPase less functional.
Remember how the cardiac myocyte rests at -90 mV?
17/28
Well, resting potential of -90mV happens because of Na-K-ATPases!
Normally, they funnel 3 Na+ OUT of the cell and 2 K+ INTO the cell for a net negative of 1 since 3+ go out and 2+ come in. Cumulatively, the cell is left at a negative -90mV!
18/28
Normally, they funnel 3 Na+ OUT of the cell and 2 K+ INTO the cell for a net negative of 1 since 3+ go out and 2+ come in. Cumulatively, the cell is left at a negative -90mV!
18/28
When there is ischemia, there is hypoxia, the Na-K-ATPase CANNOT maintain the -90mV and so the region of ischemia sits more positive...at say -60mV i.e MORE DEpol than the surrounding non-ischemic myocytes!
This = less remaining cell to DEpol, so faster time to REpol!
19/28
This = less remaining cell to DEpol, so faster time to REpol!
19/28
Remember how our REpol wave went from out to in in a healthy heart because the subendocardial cells were plumper?
With subendocardial ischemia, these cells DEpol FASTER now and at about the same speed as the epicardial cells. So, they switch to REpol faster too!
20/28
With subendocardial ischemia, these cells DEpol FASTER now and at about the same speed as the epicardial cells. So, they switch to REpol faster too!
20/28
This means the DEpol AND the REpol waves go from in to out from subendocardium to epicardium!
The REpol wave is NEGATIVE and negative toward the (+) electrode = a negative EKG deflection!
This is why the REpol wave (the T-wave) is inverted in subendocardial ischemia!
21/28
The REpol wave is NEGATIVE and negative toward the (+) electrode = a negative EKG deflection!
This is why the REpol wave (the T-wave) is inverted in subendocardial ischemia!
21/28
Note: the EKG sees “waves” of electricity - when there aren’t any waves, like in the ST segament, the EKG is at its baseline.
So - what about ST depressions and elevations?
Remember: the ischemic portion of the heart is DEpol already and permanent ischemia = forever DEpol.
So - what about ST depressions and elevations?
Remember: the ischemic portion of the heart is DEpol already and permanent ischemia = forever DEpol.
With permanent subendocardial ischemia (non-transmural) - the EKG is “seeing” the DEpol bits already, these are (+) and so the EKG notes a little bit of positivity when the heart is actually just resting (since it’s only the ischemic bits that are DEpol).
23/28
23/28
Then - after the healthy cells join and DEpol ALSO, the EKG isn’t seeing ANY waves, so draws the ST segament at baseline! This baseline is LOWER than earlier because it was seeing the perpetually DEpol ischemic bits!
24/28
24/28

For transmural ischemia - ALL the tissue is dead and the dead tissue that is DEpol at rest is sending waves AWAY from the electrode which makes the initial EKG draw NEGATIVE.
Everything DEpol = back to baseline.
Then negative again - causing an ST elevation!
25/28
Everything DEpol = back to baseline.
Then negative again - causing an ST elevation!
25/28

So, to summarize:
- positive DEpol waves toward an (+) electrode cause POSITIVE deflections on an EKG
- negative REpol waves toward a (+) electrode cause NEGATIVE deflections on an EKG
- non-permanent subendocardial ischemia causes t-wave inversions because REpol wave flips
- positive DEpol waves toward an (+) electrode cause POSITIVE deflections on an EKG
- negative REpol waves toward a (+) electrode cause NEGATIVE deflections on an EKG
- non-permanent subendocardial ischemia causes t-wave inversions because REpol wave flips
- permanent subendo ischemia causes ST depressions because of permanently DEpol tissue
- transmural ischemia flips the DEpol wave and causes ST elevations
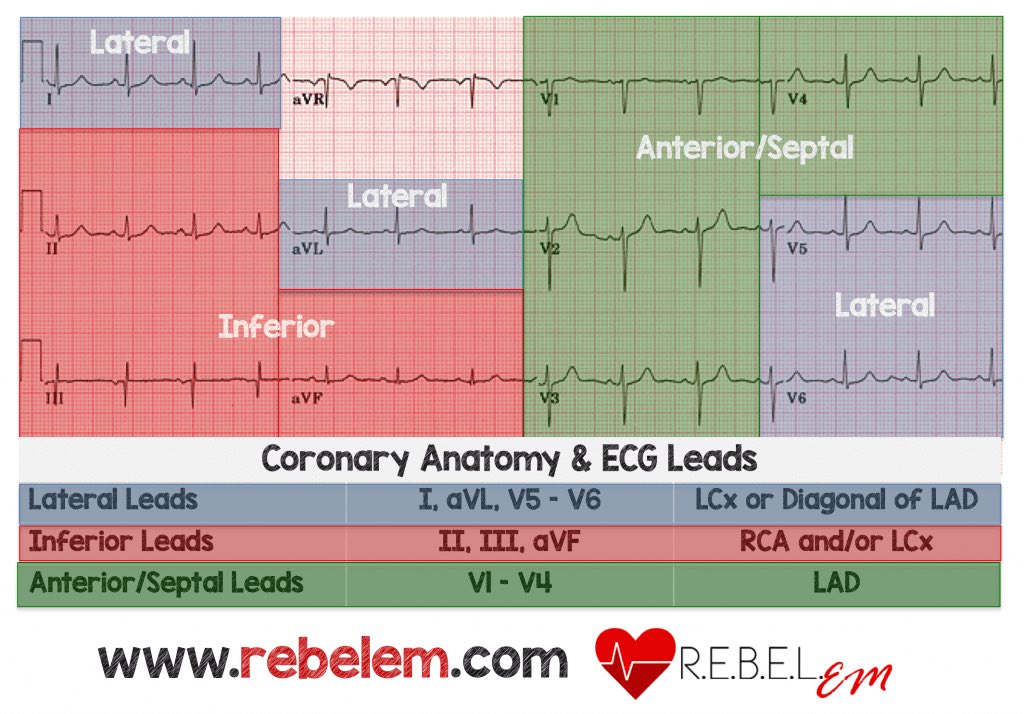
Armed w/ this understanding, you can now find the culprit lesions! It’s ALL just the leads!
27/28
- transmural ischemia flips the DEpol wave and causes ST elevations
Armed w/ this understanding, you can now find the culprit lesions! It’s ALL just the leads!
27/28
If the inferior leads have depression/elevation - there’s an issue w/ the tissue the inferior leads are “seeing” and likely the vasculature that supplies that region!
Here’s a summation of such by @srrezaie:
- just think through the “eyes” of the EKG and you’ll too will see 🤓
Here’s a summation of such by @srrezaie:
- just think through the “eyes” of the EKG and you’ll too will see 🤓