This is INSANE and is a direct outflow of the Trump administration's choice to emphasize #Coronavirus containment rather than mitigation.
Here's how.
Here's how.
A month and a half ago, when Wuhan went up in viral flames, the administration had a choice: focus on keeping the disease out (containment); focus on preparing the US health system for its inevitable arrival (mitigation); or a balanced effort at both.
Any of these options comes with trade-offs.
As @JenniferNuzzo laid out clearly yesterday, there are a finite number of public health workers, and where the government opts to focus their attention is a major strategic choice.
As @JenniferNuzzo laid out clearly yesterday, there are a finite number of public health workers, and where the government opts to focus their attention is a major strategic choice.
More emphasis on containment (traveler screening, quarantine, etc) means less on frontline community readiness.
The administration chose to put almost all its eggs into the containment basket. And that policy choice comes through clearly in this woman's experience.
The administration chose to put almost all its eggs into the containment basket. And that policy choice comes through clearly in this woman's experience.
Breakdown 1: Failure to establish a robust enough hotline to handle high call volume, or to develop alternate widely accessible ways that people can access guidance on testing.
This should have been in the works from the moment we saw the case volumes being generated in Wuhan.
This should have been in the works from the moment we saw the case volumes being generated in Wuhan.
Breakdown 2: Failure to focus intensively on frontline readiness.
Most people will turn first to their primary care doc or an urgent care clinic if they get sick. Ensuring those facilities are informed and equipped to handle a surge in questions - didn't happen.
Most people will turn first to their primary care doc or an urgent care clinic if they get sick. Ensuring those facilities are informed and equipped to handle a surge in questions - didn't happen.
There is guidance on CDC's and state health depts' websites. But there's a big difference between posting guidance on a website, vs. actively focusing public health workers on health facility outreach.
This case suggests the website guidance isn't translating into practice.
This case suggests the website guidance isn't translating into practice.
Breakdown 3: Failure to adapt testing criteria to the real-time transmission dynamics.
CDC's testing criteria expanded last week to include potential community spread - hence the nationwide jump in case identification this week. But as this instance shows, it's still too narrow.
CDC's testing criteria expanded last week to include potential community spread - hence the nationwide jump in case identification this week. But as this instance shows, it's still too narrow.
The guidance still emphasize travel history to affected countries, even though the principal driver of the outbreak going forward will be community transmission. 

The criteria *do* now allow testing for undetected community spread - but only in especially severe cases (which this person isn't, yet).
That's a problem because 80% of cases (and thus, spreaders) don't reach this level of severity. So remain invisible.
cdc.gov/coronavirus/20…
That's a problem because 80% of cases (and thus, spreaders) don't reach this level of severity. So remain invisible.
cdc.gov/coronavirus/20…

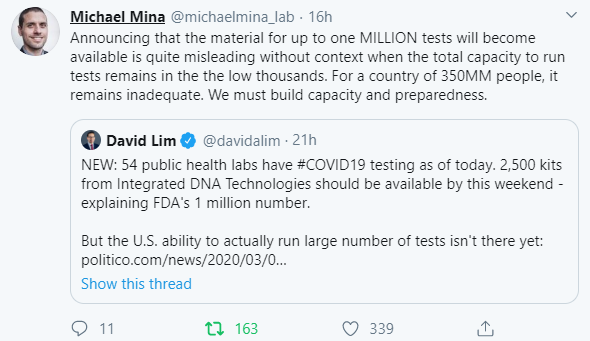
And it's only at this point that the famous shortage of test kits (now being rectified) even comes into the equation.
But there's one more breakdown: frontline hospital readiness.
As writer notes, she won't be able to get testing unless/until she ends up in the ER.
But there's one more breakdown: frontline hospital readiness.
As writer notes, she won't be able to get testing unless/until she ends up in the ER.
So ERs across the country face prospect of people showing up with severe respiratory issues but no advance knowledge of whether they could have COVID19. That puts frontline health workers at risk (like the 124 from UC-Davis who are now in self-quarantine). cnn.com/2020/02/29/hea…
And here's the thing: nothing about this chain of events is unexpected. The early situation in Wuhan gave a clear template for how this could play out elsewhere, and the strain it would put on the US health system.
That was a month and a half ago, and yet we're still unprepared.
That was a month and a half ago, and yet we're still unprepared.
And that lack of preparedness boils down to strategic decisions taken by the administration. Faced with a focus on containment, mitigation, or both/and, the administration focused almost all effort on keeping the disease out. Now clearly a strategic error.
They compounded the strategic error by assuming it was working, based on the lack of detected cases.
But that turned out to be an absence-of-evidence ≠ evidence-of-absence issue. The lack of cases reflected nothing more than the artificial narrowness of their testing criteria.
But that turned out to be an absence-of-evidence ≠ evidence-of-absence issue. The lack of cases reflected nothing more than the artificial narrowness of their testing criteria.
In sum: breakdowns in novel outbreak response are not just technical or medical - they are also strategic.
There's a clear line between high level policy choices made in the White House and a symptomatic individual potentially endangering others because she can't get tested.
There's a clear line between high level policy choices made in the White House and a symptomatic individual potentially endangering others because she can't get tested.
What needs to happen? Still much the same as the recommendations that I and others like @RebeccaKatz5 @BethCameron_DC @UNMC_DrKhan @georgetown_ghss
@_b_next @UNMCCOPH jointly issued last month:
@_b_next @UNMCCOPH jointly issued last month: