What are physician-led ACOs doing differently than Health System ACOs? [thread]
CMS released the 2017 MSSP results. While there will be thoughtful analyses of these results, I wanted to examine the multi-year trends in ACO performance. I also sought to understand the difference in performance between health system-led ACOs and physician-led ACOs. (1/n)
This analyses had three principal findings: first, by the fourth performance year, physician-led ACOs, whether due to performance improvements or attrition, lose less money than do health system-led ACOs; (2/n)
Second, among top-performing ACOs, physician-led ACOs do a better job than do health system-led ACOs of managing key utilization measures, including Part B costs, IPPS admissions, and SNF admissions; and (3/n)
And third, while ACOs are controlling the rates of hospital and SNF admissions, the costs of the unavoidable admissions appear to be rising. To-date, controlling SNF costs is largely a function of controlling IPPS admissions. More can be done to improve this performance. (4/n)
METHODS: I used the "Public Use Files" for the five MSSP performance years. ACOs began participating in MSSP at different points over the previous five years. So for each ACO I categorized the performance in that year based on the # of years that ACO had been in MSSP. (5/n)
For instance, the 2015 performance of a "Class of 2013" ACO and the 2017 performance of a "Class of 2015" ACO" would both be categorized as "T3," or the third performance year. (6/n)
I wanted to examine how ACOs were managing utilization. I compared an ACO’s performance for a utilization measure for a given year against performance for that same measure during the first year of the ACO's participation. (7/n)
I could not complete this calculation for ACOs with only one year of performance. I therefore excluded these ACOs from all analyses. (8/n)
Health system-led ACOs have different incentive structures than those of physician-led ACOs. To identify a health system-led ACO, I examined the Public Reporting webpage of an ACO to determine the "Primary Contact" and ACO Governing Board structure. (9/n)
If either the ACO "Primary Contact" or a Voting Member of the ACO Governing Board was affiliated with a health system, I categorized the ACO as a "Health System-led ACO." If neither of these conditions were met, I categorized the ACO as a "Physician-led ACO." (10/n)
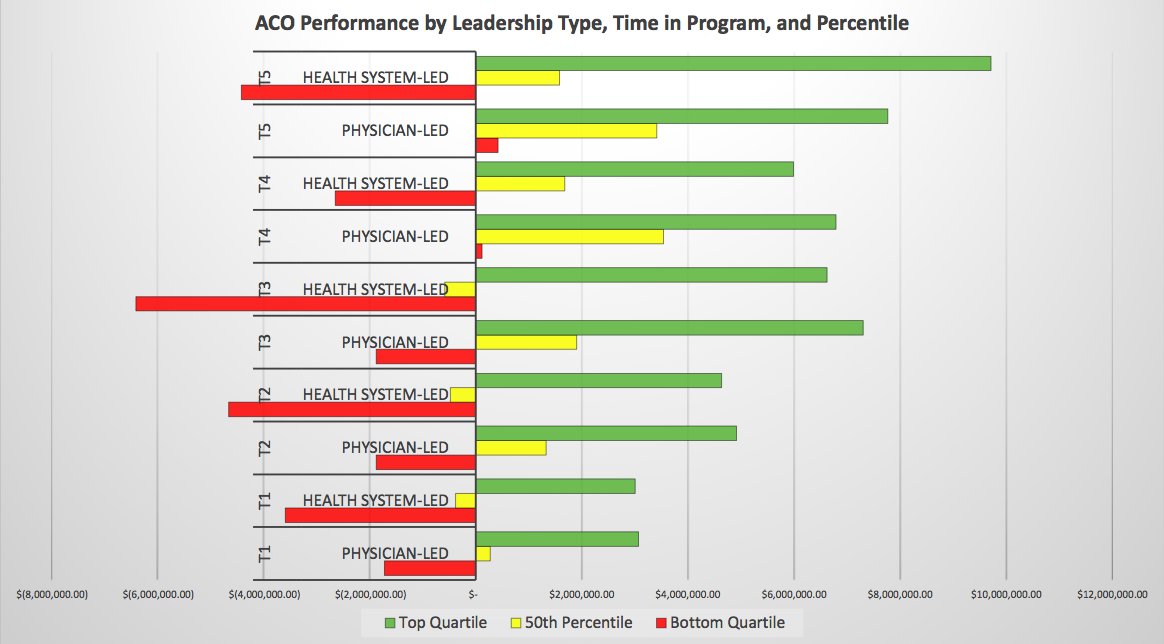
The median and average performance of ACOs belied the variability for both the health system-led and physician-led ACO categories. I therefore examined the top and bottom quartile performance within the health system ACO category. (11/n)
RESULTS: On every measure, physician-led ACOs are outperforming health system-led ACOs. With regard to health system ACOs, it appears that by the fourth performance year the average and median savings are in excess of $1.5 million. (12/n) 

But this is misleading; ACO performance is variable. By the fourth PY year, health system ACOs in the bottom quartile are still generating losses >$2.0 million. By contrast, physician-led ACOs in the the bottom quartile do not generate losses after the third PY. (13/n)
I sought to understand the difference among three categories of ACOs:
(1) Bottom quartile of health system ACOs (light blue);
(2) Top quartile of health system ACOs (dark blue); and
(3) Top quartile of physician-led ACOs (orange).
(14/n)
(1) Bottom quartile of health system ACOs (light blue);
(2) Top quartile of health system ACOs (dark blue); and
(3) Top quartile of physician-led ACOs (orange).
(14/n)
ACO population size is not a determinant of savings, either for health system ACOs or for physician-led ACOs. (15/n)

On the utilization measure aggregating physician services, imaging, and physician-administered drugs, top quartile physician-led ACOs are outperforming all types of health system ACOs. (16/n)

Top quartile physician-led ACOs are also outperforming all types of health system ACOs on measures of hospital admissions and costs. But reductions in IPPS adm. are not tightly correlated with IPPS costs. (17/n)

Top quartile ACOs in both categories are reducing hospital admissions. But health system ACOs saw an increase in per-capita costs, suggesting that the unavoidable admissions are more costly (and complex) than the prevented ones. (18/n)

The health system-led and physician-led ACO performance on SNF measures tells a story that is similar to that for ACO performance on hospital measures. While top quartile ACOs reduced per-capita SNF admissions, health system ACOs saw an increase in per-capita costs (19/n).

How are top quartile ACOs keeping SNF costs and admissions down? By reducing hospital admissions and costs, which reduces SNF costs, especially for health system ACOs. Without the predicate 3-day hospital stay, patients are not eligible for SNF admissions. (20/n)

DISCUSSION: it remains to be seen how ACOs are managing the patients that do experience acute exacerbations. I suspect this is why physician-led ACOs are not reducing per-capita hospital and SNF costs as quickly as they are reducing hospital admissions. (21/n)
And it is likely why even top-performing health system ACOs are still experiencing increases in hospital and SNF costs. (22/22)