,
14 tweets,
6 min read
Read on Twitter
1/
Why is the AST/ALT ratio >2 in alcoholic liver disease?
If ALT is “specific” for the liver, one might expect that any liver process would lead to a low AST/ALT ratio.
Let’s review some potential mechanistic explanations...
Why is the AST/ALT ratio >2 in alcoholic liver disease?
If ALT is “specific” for the liver, one might expect that any liver process would lead to a low AST/ALT ratio.
Let’s review some potential mechanistic explanations...
2/
The high AST/ALT ratio seen in alcoholic liver disease could result from a disproportionately high AST, a disproportionately low ALT, or a combination of both.
What's your current explanation for the elevated AST/ALT ratio in alcoholic liver disease?
The high AST/ALT ratio seen in alcoholic liver disease could result from a disproportionately high AST, a disproportionately low ALT, or a combination of both.
What's your current explanation for the elevated AST/ALT ratio in alcoholic liver disease?
3/
The answer is (probably) BOTH. Before getting into the mechanisms, some background will be useful.
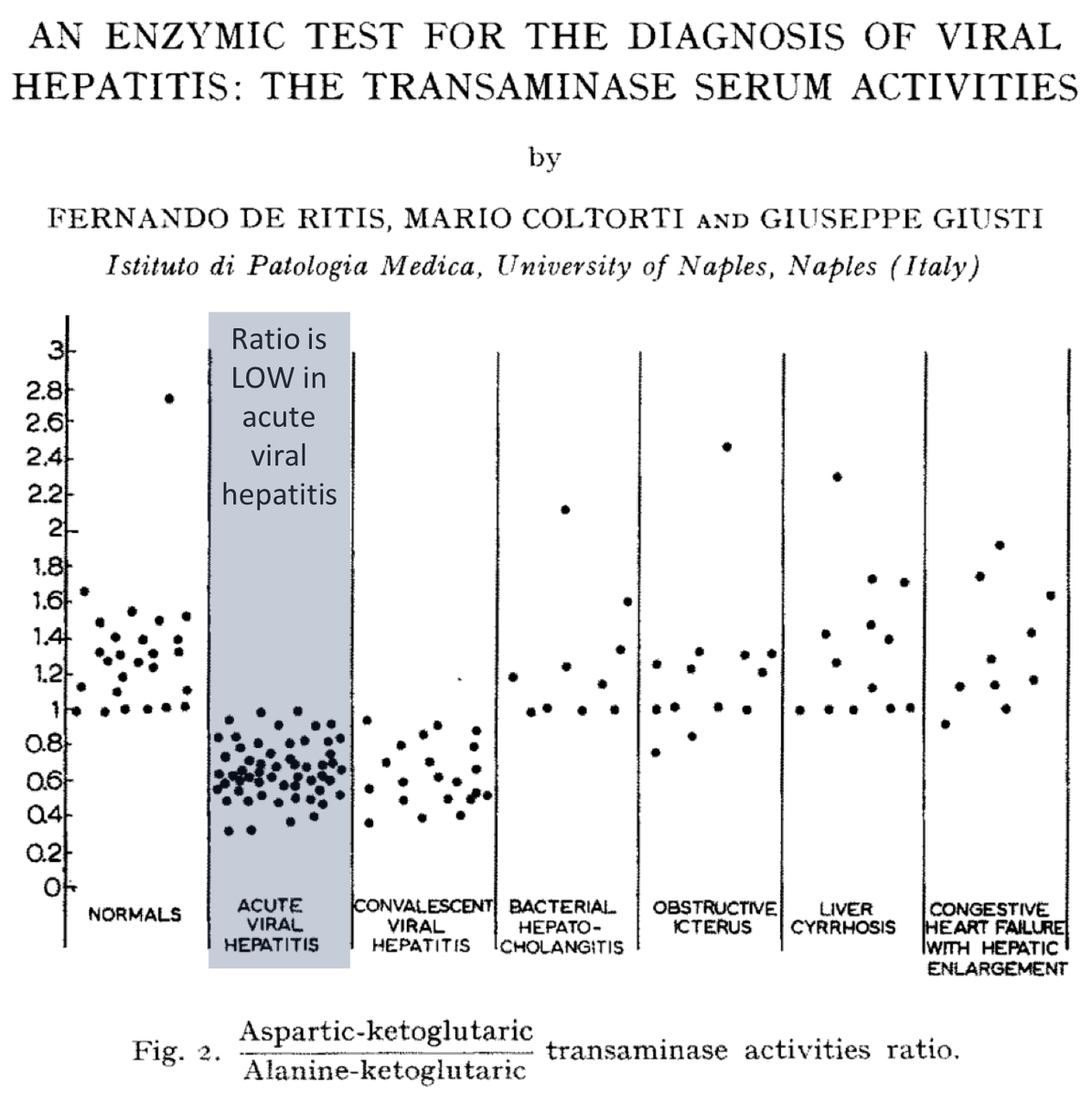
The AST/ALT ratio was first described by Fernando De Ritis in 1957. He observed that a LOW (i.e., <1) ratio was associated with acute viral hepatitis.
ncbi.nlm.nih.gov/pubmed/13447217
The answer is (probably) BOTH. Before getting into the mechanisms, some background will be useful.
The AST/ALT ratio was first described by Fernando De Ritis in 1957. He observed that a LOW (i.e., <1) ratio was associated with acute viral hepatitis.
ncbi.nlm.nih.gov/pubmed/13447217
4/
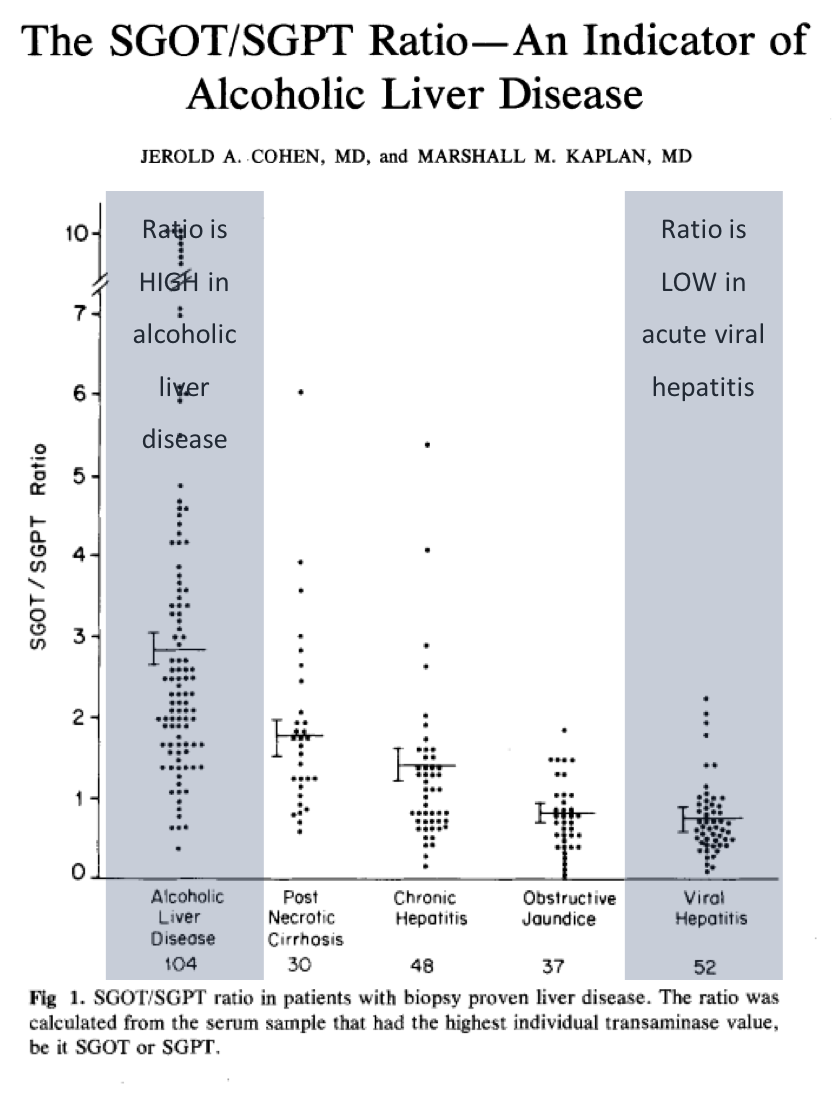
In 1979, Cohen and Kaplan examined the AST/ALT ratio and noted that it is >2 in those with alcoholic liver disease.
They also confirmed De Ritis observation of a low ratio in acute viral hepatitis.
ncbi.nlm.nih.gov/pubmed/520102
In 1979, Cohen and Kaplan examined the AST/ALT ratio and noted that it is >2 in those with alcoholic liver disease.
They also confirmed De Ritis observation of a low ratio in acute viral hepatitis.
ncbi.nlm.nih.gov/pubmed/520102
5/
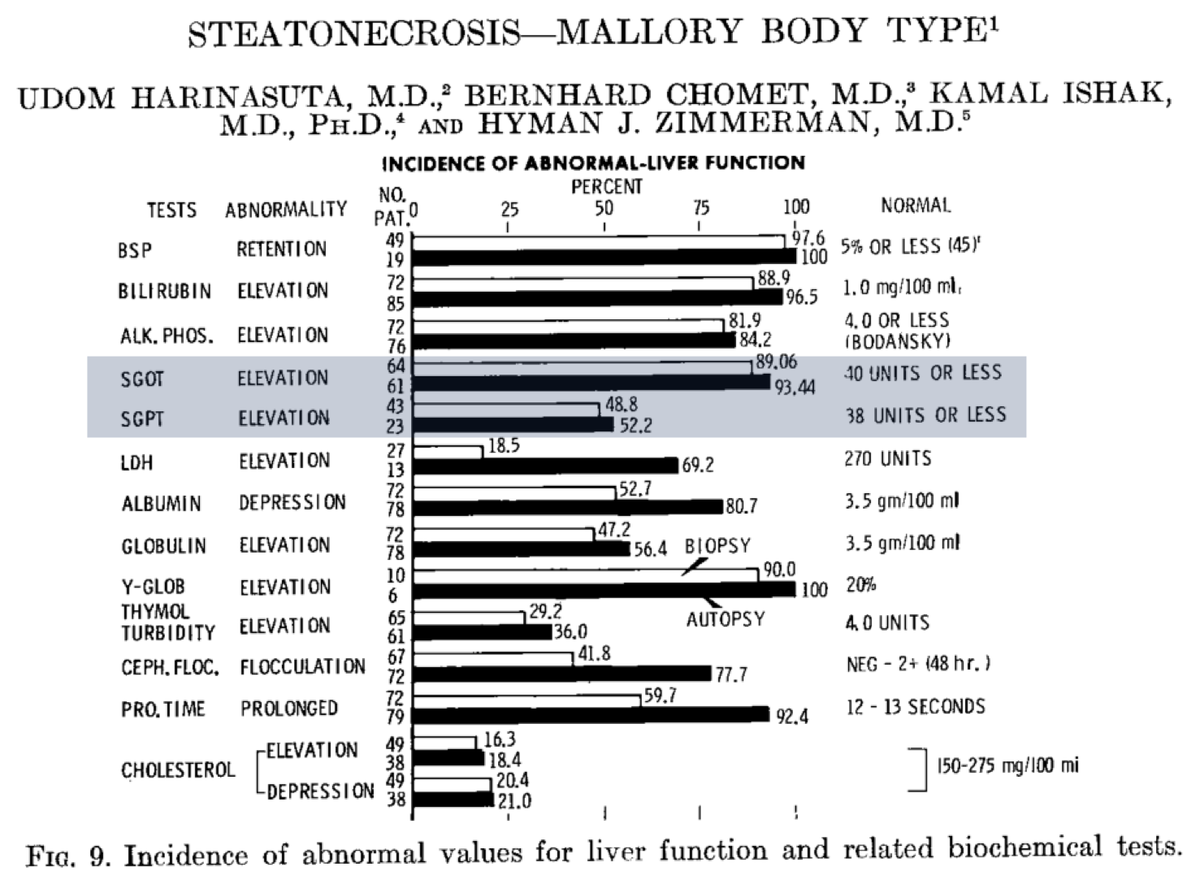
A final piece of history helps explain one of the reasons the AST/ALT ratio is >2 in alcoholic liver disease.
In 1967, Harinasuta reported that the absolute value of AST is high in alcoholic liver disease, without a matching elevation of ALT.
ncbi.nlm.nih.gov/pubmed/5338701
A final piece of history helps explain one of the reasons the AST/ALT ratio is >2 in alcoholic liver disease.
In 1967, Harinasuta reported that the absolute value of AST is high in alcoholic liver disease, without a matching elevation of ALT.
ncbi.nlm.nih.gov/pubmed/5338701
6/
This is mechanism 1: excess (high) AST.
But what is it about alcohol-mediated injury that leads to a rise in AST?
This is mechanism 1: excess (high) AST.
But what is it about alcohol-mediated injury that leads to a rise in AST?
7/
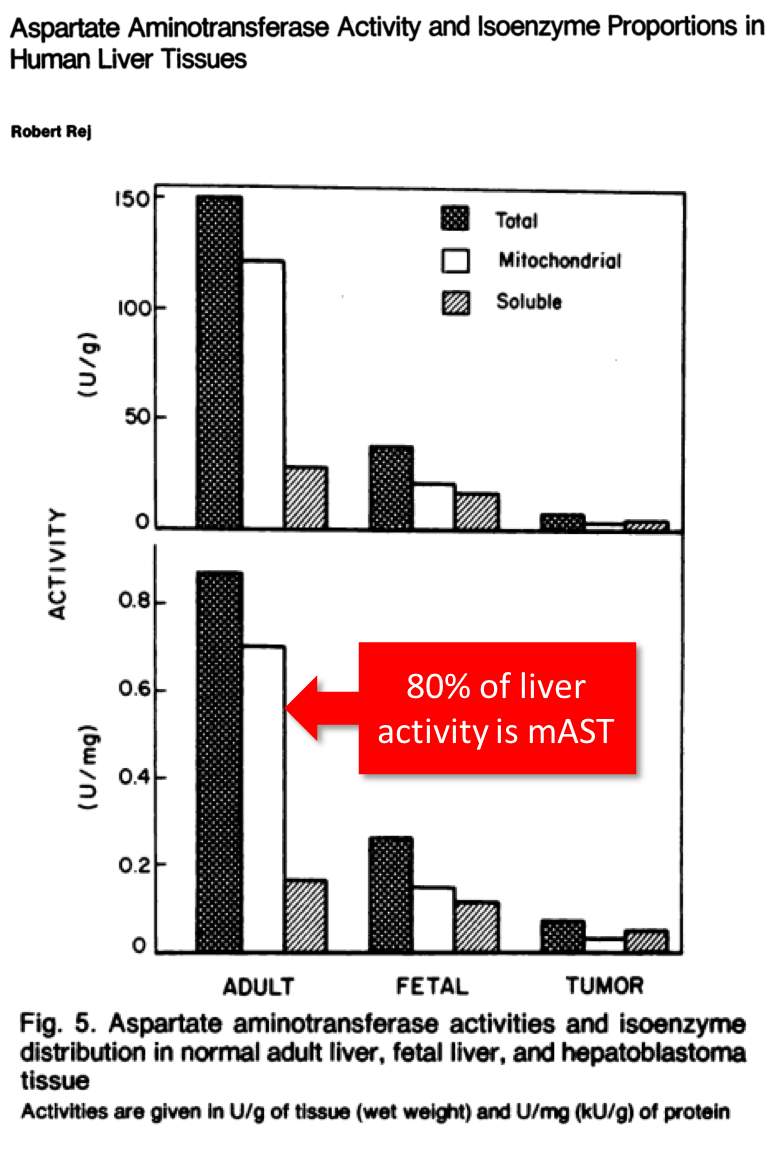
Three key points:
*there are two AST isoenzymes in the liver: cytoplasmic (cAST) and mitochondrial (mAST)
*80% of AST activity in human liver is mAST (Pic 1)
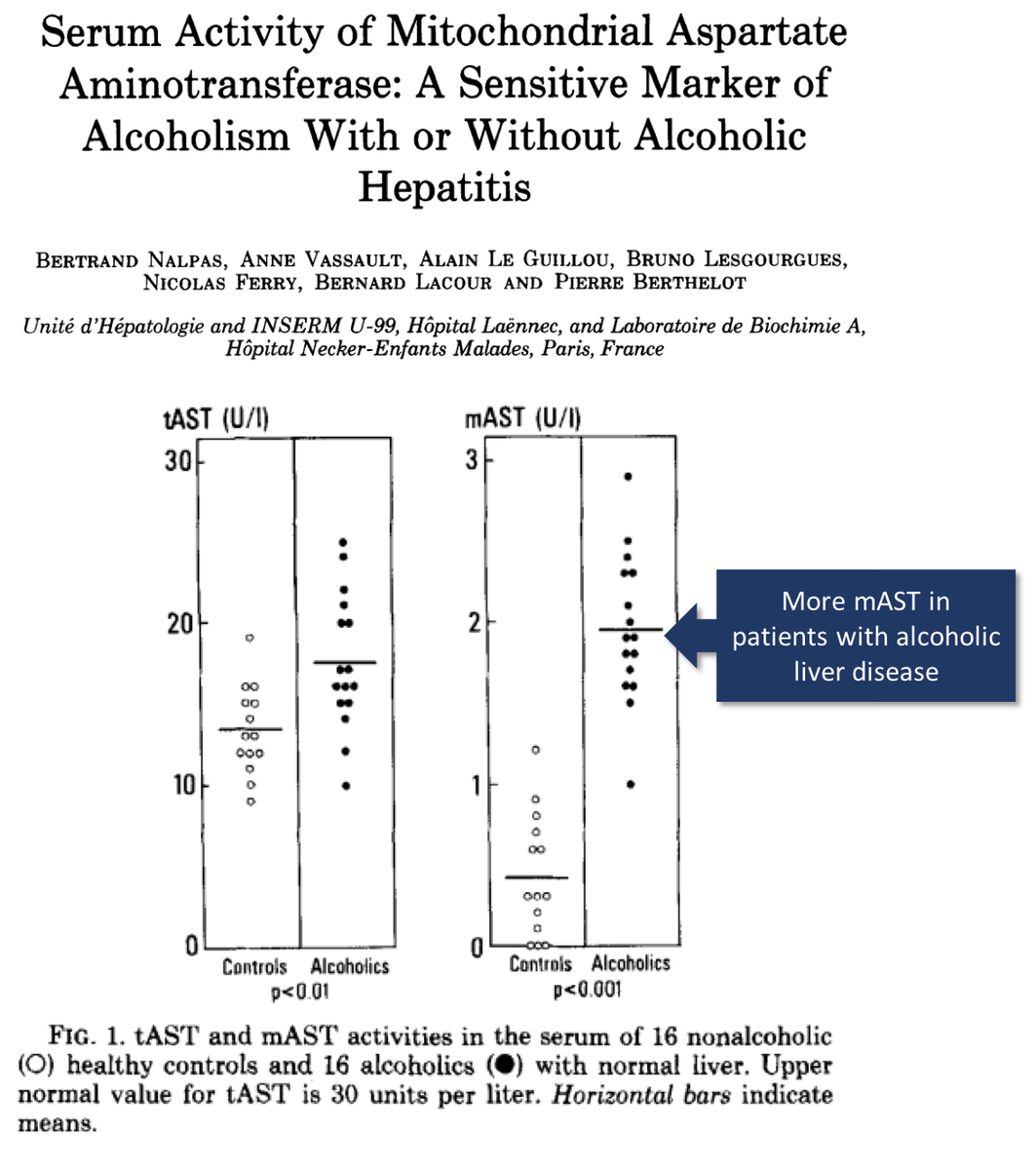
*alcohol leads to increases mAST, via mitochondrial injury (Pic 2)
ncbi.nlm.nih.gov/pubmed/213206
ncbi.nlm.nih.gov/pubmed/6148299
Three key points:
*there are two AST isoenzymes in the liver: cytoplasmic (cAST) and mitochondrial (mAST)
*80% of AST activity in human liver is mAST (Pic 1)
*alcohol leads to increases mAST, via mitochondrial injury (Pic 2)
ncbi.nlm.nih.gov/pubmed/213206
ncbi.nlm.nih.gov/pubmed/6148299
8/
Mechanism 1 (updated): excess (high) mAST
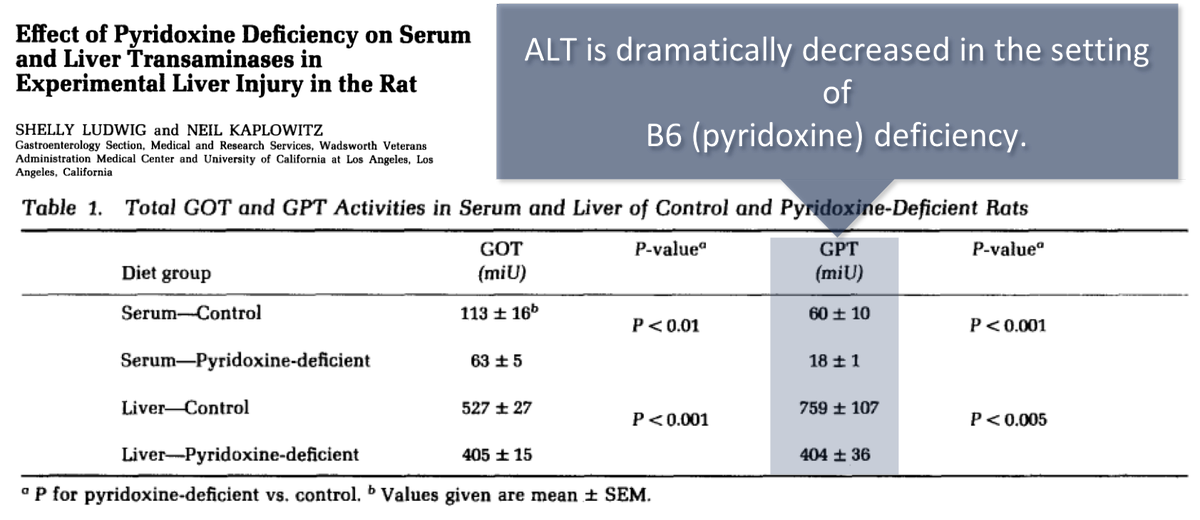
Mechanism 2: suppressed ALT
B6 is a required cofactor for AST and ALT activity. Decreased B6 levels are associated with decreased serum activity, though the suppressive effect seems more pronounced with ALT.
ncbi.nlm.nih.gov/pubmed/7429115
Mechanism 1 (updated): excess (high) mAST
Mechanism 2: suppressed ALT
B6 is a required cofactor for AST and ALT activity. Decreased B6 levels are associated with decreased serum activity, though the suppressive effect seems more pronounced with ALT.
ncbi.nlm.nih.gov/pubmed/7429115
9/
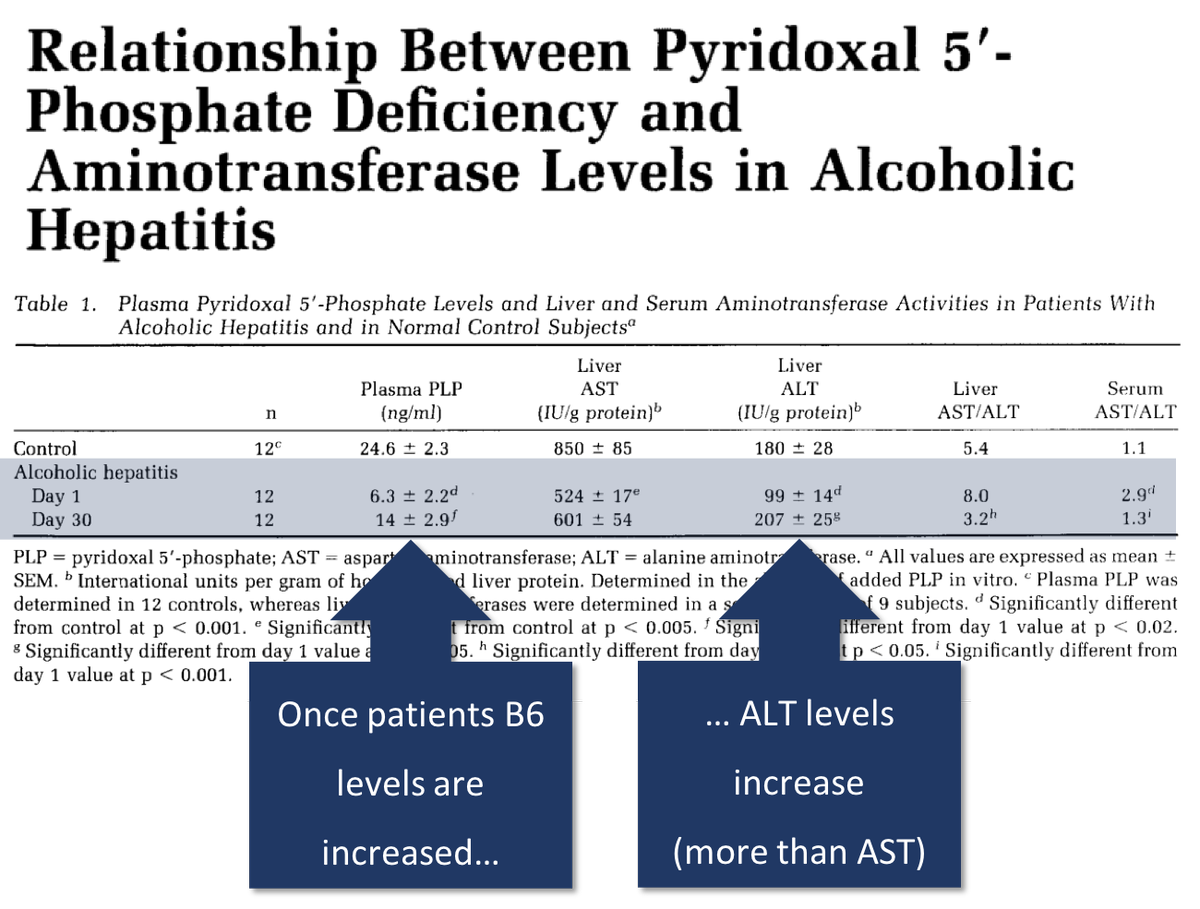
Low B6 levels are seen in patients with alcoholic hepatitis. If you give back B6, the liver ALT rises. The AST does as well, but not nearly as much.
ncbi.nlm.nih.gov/pubmed/6698365
Low B6 levels are seen in patients with alcoholic hepatitis. If you give back B6, the liver ALT rises. The AST does as well, but not nearly as much.
ncbi.nlm.nih.gov/pubmed/6698365
10/
The clearance of AST and ALT is also relevant to their ratio.
*half-life for AST = 18 hours
*half-life for ALT = 36 hours
Given this, what would you predict happens to the AST/ALT ratio after an acute liver injury?
The clearance of AST and ALT is also relevant to their ratio.
*half-life for AST = 18 hours
*half-life for ALT = 36 hours
Given this, what would you predict happens to the AST/ALT ratio after an acute liver injury?
11/
As AST has a shorter half-life, the AST/ALT ratio may decrease over the course of a hospitalization. One study found:
Day 1: AST/ALT ratio = 2.7
Day 4-6: 2.2
Day 7-10: 1.7
ncbi.nlm.nih.gov/pubmed/15208167
As AST has a shorter half-life, the AST/ALT ratio may decrease over the course of a hospitalization. One study found:
Day 1: AST/ALT ratio = 2.7
Day 4-6: 2.2
Day 7-10: 1.7
ncbi.nlm.nih.gov/pubmed/15208167
12/
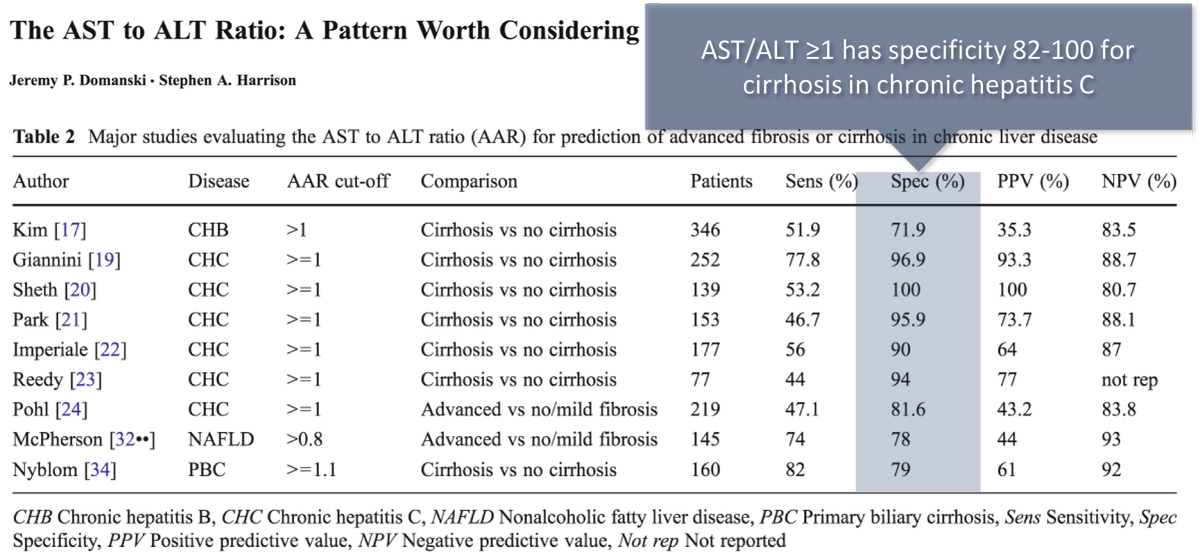
On the other hand, because AST is cleared within the liver by sinusoidal cells, as cirrhosis develops, clearance may decrease.
Result: the AST/ALT ratio increases as cirrhosis develops; this change may be seen over years.
link.springer.com/article/10.100…
On the other hand, because AST is cleared within the liver by sinusoidal cells, as cirrhosis develops, clearance may decrease.
Result: the AST/ALT ratio increases as cirrhosis develops; this change may be seen over years.
link.springer.com/article/10.100…
13/
Before summarizing, let's ask re-ask a question from above:
What's your current explanation for the elevated AST/ALT ratio in alcoholic liver disease?
Before summarizing, let's ask re-ask a question from above:
What's your current explanation for the elevated AST/ALT ratio in alcoholic liver disease?
14/
In summary, explanations for the AST/ALT ratio >2 in alcoholic liver disease include:
⭐️mitochondrial damage leading to mAST release
⭐️low B6, leading to suppressed ALT
And, if cirrhosis is present:
⭐️decreased clearance of AST
In summary, explanations for the AST/ALT ratio >2 in alcoholic liver disease include:
⭐️mitochondrial damage leading to mAST release
⭐️low B6, leading to suppressed ALT
And, if cirrhosis is present:
⭐️decreased clearance of AST