,
17 tweets,
11 min read
Read on Twitter
Just wrapped up 2 weeks on the @MGHMedicine service! Let's celebrate with....
#CELLULITIS - a #tweetorial/#medthread!
#MedEd #FOAMEd #dermtwitter #medtwitter #derm #dermatologia #dermatology PC:@dermnetnz
1/
#CELLULITIS - a #tweetorial/#medthread!
#MedEd #FOAMEd #dermtwitter #medtwitter #derm #dermatologia #dermatology PC:@dermnetnz
1/
What is cellulitis? It's a bacterial infection of the deep dermis & subcutis. Every year, there are ~ 14.5 million cases diagnosed in the US, leading to >600,000 admissions! What does it usually look like? Remember: Tumor, rubor, color, dolor (swelling, red, warm, painful)!
2/
2/

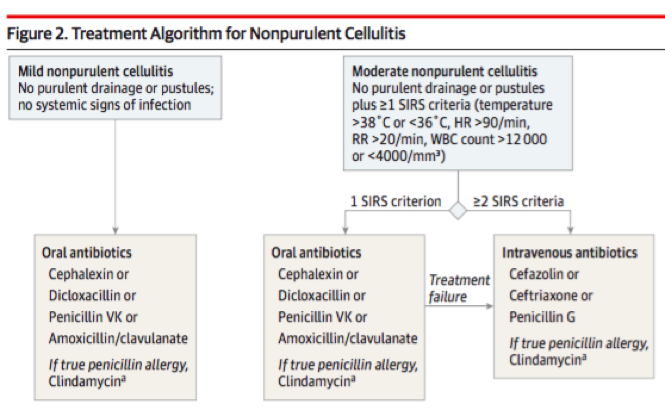
Most likely organisms are staph or strep. Abx choice targets those organisms. For a non-purulent cellulitis in a non-sick pt (1 or fewer SIRS criteria), oral abx are good. IV for non-responders or those with 2 or >SIRS. Check out the algorithm from: jamanetwork.com/journals/jama/…
3/
3/
For purulent cellulitis, it's the same algorithm, but throw a wound culture in. MRSA coverage should be considered. Oral abx (with MRSA coverage often) for pts with 1 or fewer SIRS criteria, and IV only for treatment non-responders or those with 2 or > SIRS at presentation.
4/
4/
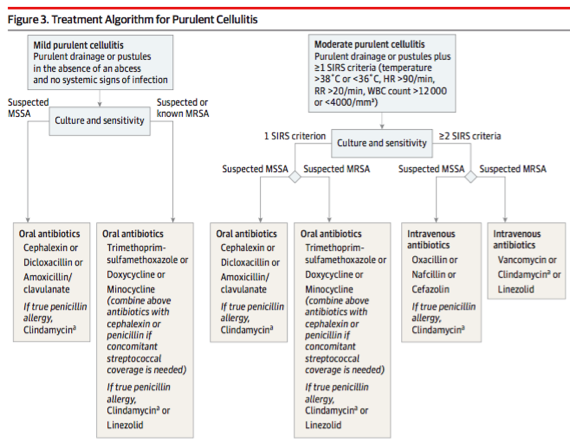
However, certain things should buy you broad spectrum antibiotics. In short, these are immunocompromised hosts, septic shock, or rapid progression of disease. This goes regardless of if you've got purulence on exam or not. Check out the right most side of these algorithms!
5/
5/


A brief aside about antibiotic choice: I still see many people treat uncomplicated non-purulent cellulitis with the trimethoprim/sulfamethoxasole + cephalexin combination. Did you know that's unnecessary? This paper showed cephalexin alone is fine.
6/
6/


Back to the algorithm, I have 1 caveat. It suggest that if pts don't respond to oral antibiotics, you should trial IV abxs. I would point out though that this algorithm assumes the diagnosis is correct. There are many mimickers of cellulitis (below) that also wouldn't respond!
7/
7/
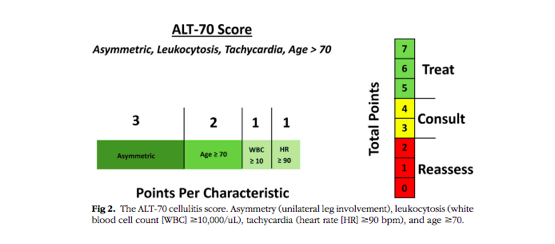
So, what if you're not sure? Enter ALT-70! This paper can help with the diagnosis of cellulitis.
Asymmetry: 3 pts
Age>70: 2
WBC>10: 1
HR> 90: 1
5-7 pts: treat as cellulitis
3-4 pts: #derm consult
1-2: reassess
Great work from @AMostaghimi & others - jaad.org/article/S0190-…
8/
Asymmetry: 3 pts
Age>70: 2
WBC>10: 1
HR> 90: 1
5-7 pts: treat as cellulitis
3-4 pts: #derm consult
1-2: reassess
Great work from @AMostaghimi & others - jaad.org/article/S0190-…
8/
Not only is getting the right diagnosis important for the pt, but also for the whole system! A follow up study showed the misdiagnosis of cellulitis may add 50-130,000 unnecessary admissions a year, & 195-515 million avoidable healthcare dollars spent! jamanetwork.com/journals/jamad…
9/
9/
And for all you lab hawks: remember that cellulitis is a localized infection that might not necessarily get a systemic response. Leukocytosis only occurs in ~50% of patients, & while procalcitonin has been studied in PNA, it hasn't been validated/proven to be helpful in SSTI.
10/
10/
So let's talk about mimickers! The @JAMA review on cellulitis has great figures that show how difficult it is. The mimickers I usually see are: stasis dermatitis, contact dermatitis, & (being in Boston) erythema migrans....(insert comment about #climatechange affecting that).
11/
11/


Stasis dermatitis, from venous insufficiency, is usually chronic, & BILATERAL. As my friend @MishaRosenbach would say, "Bilateral cellulitis is case reportable." Photo2 is lipodermatosclerosis, which is end stage stasis. On exam, we often see this "inverted champagne bottle."
12/
12/


These patients should get compression primarily, & a little topical steroid helps if inflamed. Off the rack compression hose is good, but pts should be measured for the right pair.
What do you think would happen if we gave these stasis patients some IV abx & admitted them?
13/
What do you think would happen if we gave these stasis patients some IV abx & admitted them?
13/
The poll is to point out something we hear. "This pt was admitted for recurrent cellulitis, & always improves with vancomycin!" However, pts with stasis will also improve if you admit them! It's not the vanco/abx, it's the leg elevation from being in bed! So don't be fooled!
14/
14/
Contact dermatitis is an allergic or irritant reaction to something in the environment. We usually see a GEOMETRIC shape (sharp lines & shapes; cellulitis is more ill-defined and doesn't skip normal skin)! These patients are ITCHY. Cellulitis patients usually aren't.
15/
15/

And finally, erythema migrans! As you all know, this is usually a TARGETOID eruption, but sometimes it can just look like a round red plaque. Patients may remember a tick bite, which obvi helps. If the location of the rash is atypical for cellulitis, definitely think of this!
16/
16/

Recap:
- Cellulitis: usually unilateral, painful, red, swollen, & warm
- It's a clinical dx. ALT-70 can help.
- If pt isn't sick: non-purulent ->oral MSSA/strep coverage; Purulent-> think MRSA.
- If no response, reconsider dx. IV abx can be tried.
Thanks for tuning in!
17/17
- Cellulitis: usually unilateral, painful, red, swollen, & warm
- It's a clinical dx. ALT-70 can help.
- If pt isn't sick: non-purulent ->oral MSSA/strep coverage; Purulent-> think MRSA.
- If no response, reconsider dx. IV abx can be tried.
Thanks for tuning in!
17/17