In honor of #skin #cancer awareness month, here's a #tweetorial on #SKINCANCER!
There is SO much we could talk about, so I'm going to keep it basic. #Dermtwitter, please add more!
#MedEd #FOAMed #dermatology #medtwitter @aadmember #dermatologia pc: @dermnetnz & @aadskin
1/
There is SO much we could talk about, so I'm going to keep it basic. #Dermtwitter, please add more!
#MedEd #FOAMed #dermatology #medtwitter @aadmember #dermatologia pc: @dermnetnz & @aadskin
1/
There are many types of skin cancer, but we'll focus on the big 3 in this #thread. We'll discuss basal cell carcinoma (BCC), Squamous cell carcinoma (SCC) & melanoma. The first two are types of "non-melanoma skin cancer (NMSC)," or more aptly named "keratinocytic carcinomas."
2/
2/
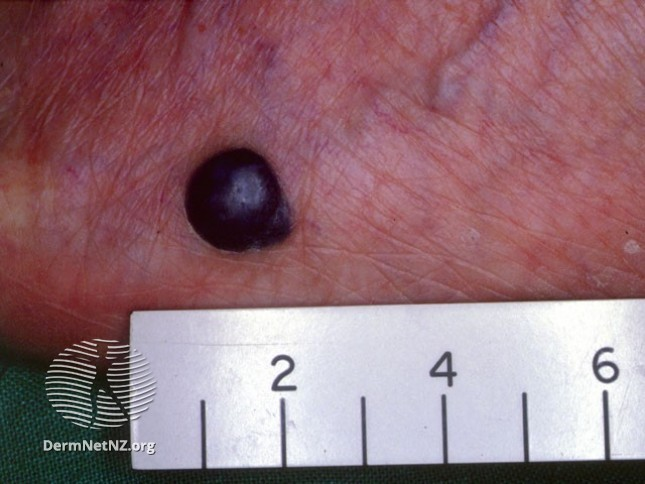
BCCs are the most common cancer diagnosed. Classically described as "pink pearly papules," they often have "arborizing" (tree-like) telangiectasias. But, they don't always have to look classic. The 1st pic is the classic, but the others are also BCCs (superficial & pigmented)!
3/
3/



Did you know there is a genetic syndrome called "Basal Cell Nevus Syndrome (BCNS)" aka "Gorlin's?" It's an autosomal dominant mutation in the tumor suppressor PTCH1 gene. Patients get many BCCs (pic 1), along with palmar pits (pic 2), jaw cysts, frontal bossing, and more.
4/
4/


BCCs almost never metastasize to other organs, & instead are locally invasive if not treated. Rare cases of metastatic BCC, BCNS, or locally aggressive disease may require targeted therapy with vismodegib, which was approved in 2012 & is now in trials for other cancers!
5/
5/
SCCs are the 2nd most common type of skin cancer. They look like scaly papules and plaques (photo 1). They can arise in a longstanding wound (Marjolin's ulcer - photo 2) but usually are from sun damage. Actinic keratoses (photo 3) are precancerous lesions that can become SCCs.
6/
6/



Immunosuppressed pts are at increased risk of SCC. As such, all our transplant patients are referred to our high risk skin cancer clinic for more frequent surveillance. Unlike BCCs, SCCs can metastasize! High risk lesions should prompt further work up.
ascopubs.org/doi/full/10.12…
7/
ascopubs.org/doi/full/10.12…
7/
Usually, the tx for these NMSC is usually destruction or surgical removal. Those on the head & neck may need mohs surgery, which is a tissue sparing surgery to allow for real time margin control. Some NMSCs can be treated with creams! Any #dermatologist can help guide tx!
5/
5/
However, high risk lesions may require staging scans, lymph node biopsies, and further work up, including multidisciplinary care. It's important to refer these patients to an appropriate center if that's the case!
6/
6/
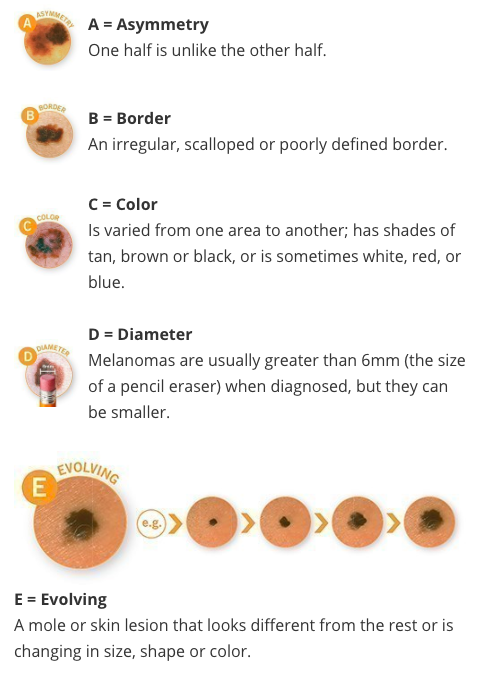
Let's move on to melanoma. Although not as common, it is the deadliest skin cancer. Unlike the previous two that are from changing keratinocytes, #melanoma is from atypical melanocytes (pigment producing cells). We always spend time education our patients on the ABCDEs!
7/
7/
There are many different types of melanoma. Some are superficial spreading (pic 1), some just start growing down and are nodular (pic 2). The ones that really scare every #derm (and really everyone) are the amelanotic ones (pic 3). Some can be in the nails and acral (pic 4).
8/
8/



Different patient characteristics change our risk assessment. Darker skinned individuals are less likely to have melanoma, but relatively speaking, acral melanomas are a concern. Patients with strong family histories, including pancreatic cancer, might have a genetic factor!
9/
9/
When melanoma is diagnosed, staging is important for prognosis & planning next steps. I think most of us know that the Breslow depth of the lesion is the most important for staging. But, do you know which of the following was REMOVED from melanoma staging of T1 tumors in 2018?
10
10
The 8th ed AJCC guidelines in 2018 removed mitotic rate from T1 melanoma staging, and also reduced the Breslow cutoff from 1mm to 0.8mm for differentiating T1a and T1b lesions. Ulcerations remained, and Clark's level was never a part of it!
skincancer.org/publications/t…
11/
skincancer.org/publications/t…
11/
Early stage melanoma lesions can be removed via wide local excision by a dermatologist or surgical oncologist. More advanced lesions and disease may require multidisciplinary care including the above, and of course a medical oncologist. Things are improving all the time!
12/
12/
Remember that the best thing to do for all these skin cancers is prevention. We know that UV has been linked with the development of these malignancies, so mitigating that risk with prevention can be our best strategy for tackling the skin cancer epidemic!
13/
13/
A brief interlude to mention a topic of interest. Immune checkpoint inhibition was first approved for melanoma and it has since revoluntionized #oncology! My own research interest is in the skin toxicities our patients get from these drugs! I hope to share our research soon!
14/
14/
To recap:
- Skin cancer is unbelievably common.
- Prevention is key to decreasing burden on patients & the healthcare system.
- If early, local therapy guided by a board certified #dermatologist can be all you need.
- More aggressive forms may require multidisciplinary care.
15/
- Skin cancer is unbelievably common.
- Prevention is key to decreasing burden on patients & the healthcare system.
- If early, local therapy guided by a board certified #dermatologist can be all you need.
- More aggressive forms may require multidisciplinary care.
15/
Thanks for listening! I hope this was somewhat helpful, no matter what your own role may be in the healthcare field.
Again, #dermtwitter, please feel free to add your own thoughts, and check out this link from @aadskin for more pt friendly info:
aad.org/public/spot-sk…
16/16
Again, #dermtwitter, please feel free to add your own thoughts, and check out this link from @aadskin for more pt friendly info:
aad.org/public/spot-sk…
16/16