,
40 tweets,
17 min read
Read on Twitter
1/ In October 2018 the @SCC_CCS released an update to the AF guidelines. This update included a significant revision of the recommendations for anticoagulation therapy around cardioversion. Space limited the discussion so...
onlinecjc.ca/retrieve/pii/S…
onlinecjc.ca/retrieve/pii/S…
2/ Last month Dr. Mitchell and myself wrote a follow-up article that expanded the evidence review.
In light of that article I thought I'd expand on the previous tweetorial.
@CAEP_Docs @UBCDoM @Vadeboncoeur_Al @CANet_nce @BCEmergMedNtwrk onlinecjc.ca/article/S0828-…
In light of that article I thought I'd expand on the previous tweetorial.
@CAEP_Docs @UBCDoM @Vadeboncoeur_Al @CANet_nce @BCEmergMedNtwrk onlinecjc.ca/article/S0828-…
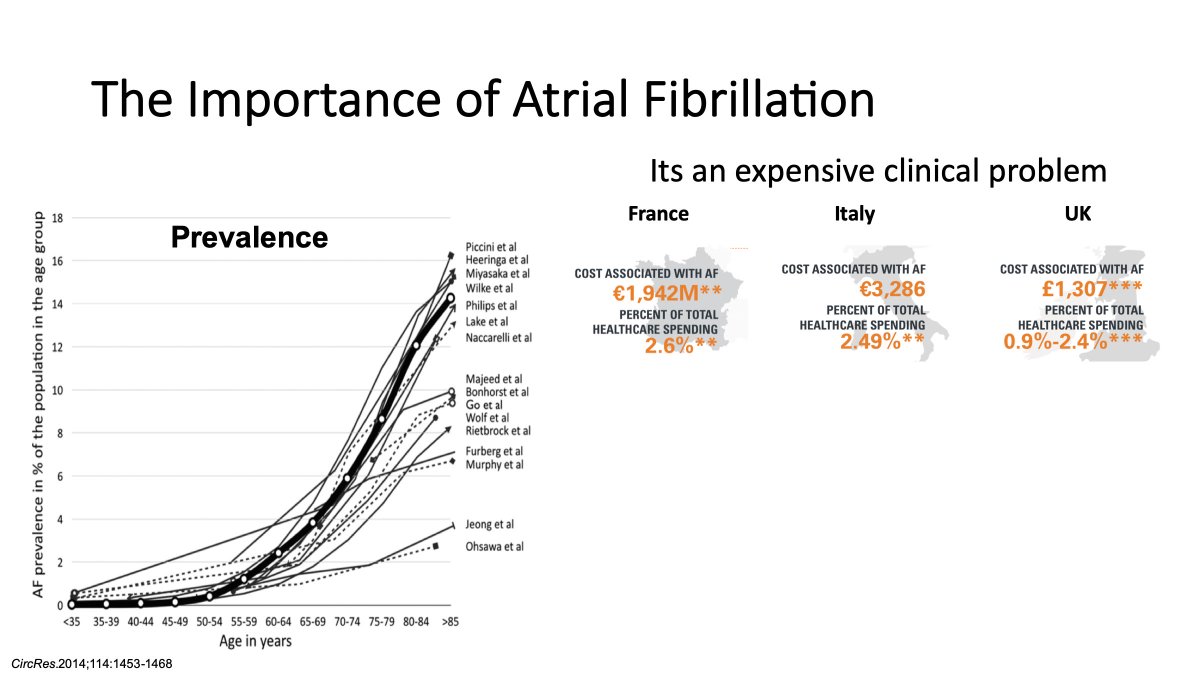
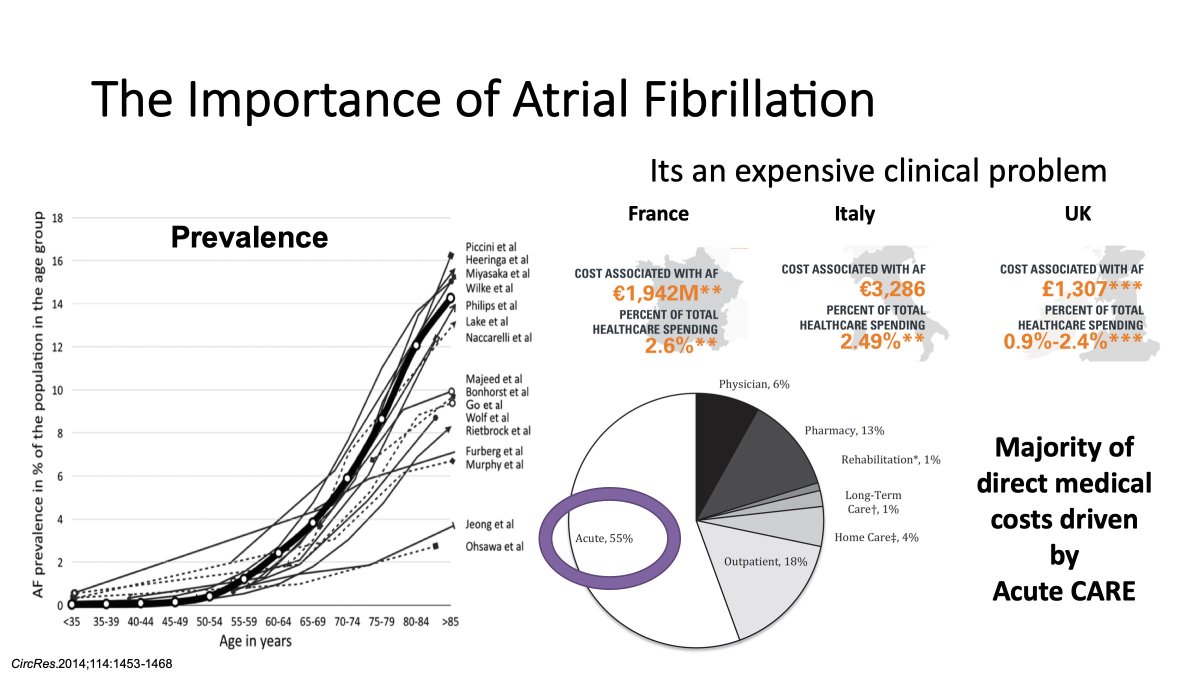
3/ First, it is important to remember why AF is important. AF is increasingly common as the general population ages (and by extension our patients). The estimated lifetime-risk of developing AF is 22-26% for individuals 40-55 years of age. 

4/ Beyond this high prevalence, AF is an expensive clinical problem. Acute care of AF accounts for ~2.5% of overall healthcare spending. And that doesn't take into account lost productivity, premature mortality, or nursing home costs.
5/ The big driver of this health care utilization is acute care costs. Why?
Because, AF patients are symptomatic. So they seek care during an acute exacerbation, typically in the form of sinus rhythm restoration through cardioversion.
Because, AF patients are symptomatic. So they seek care during an acute exacerbation, typically in the form of sinus rhythm restoration through cardioversion.
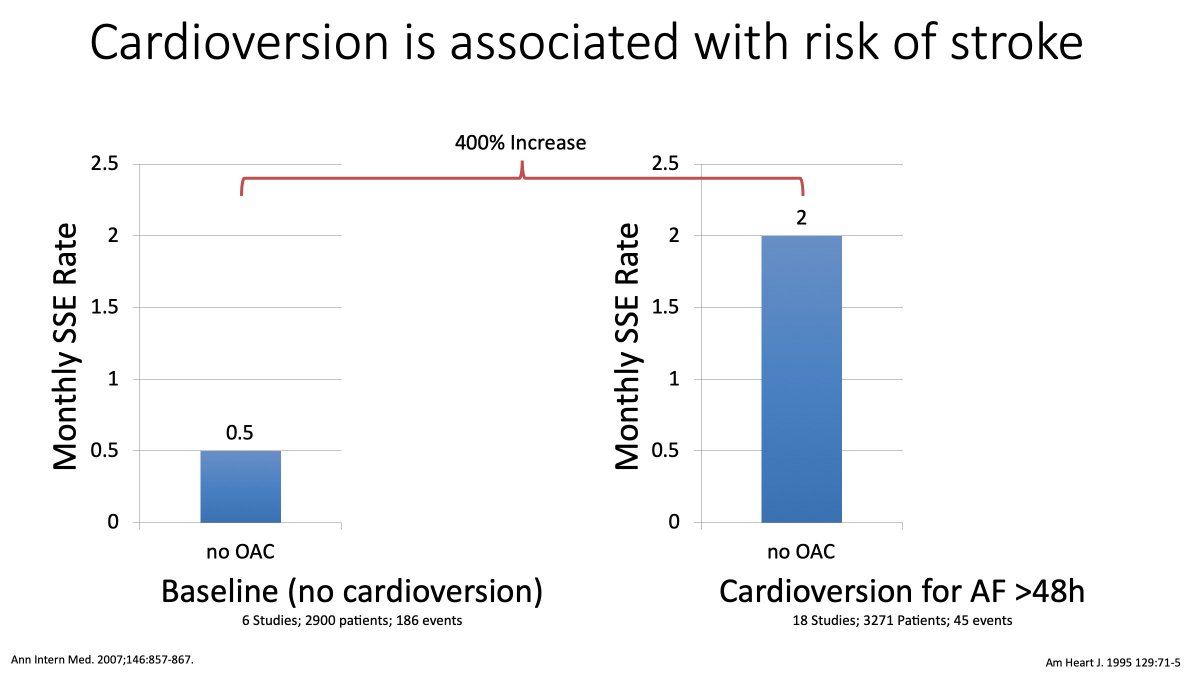
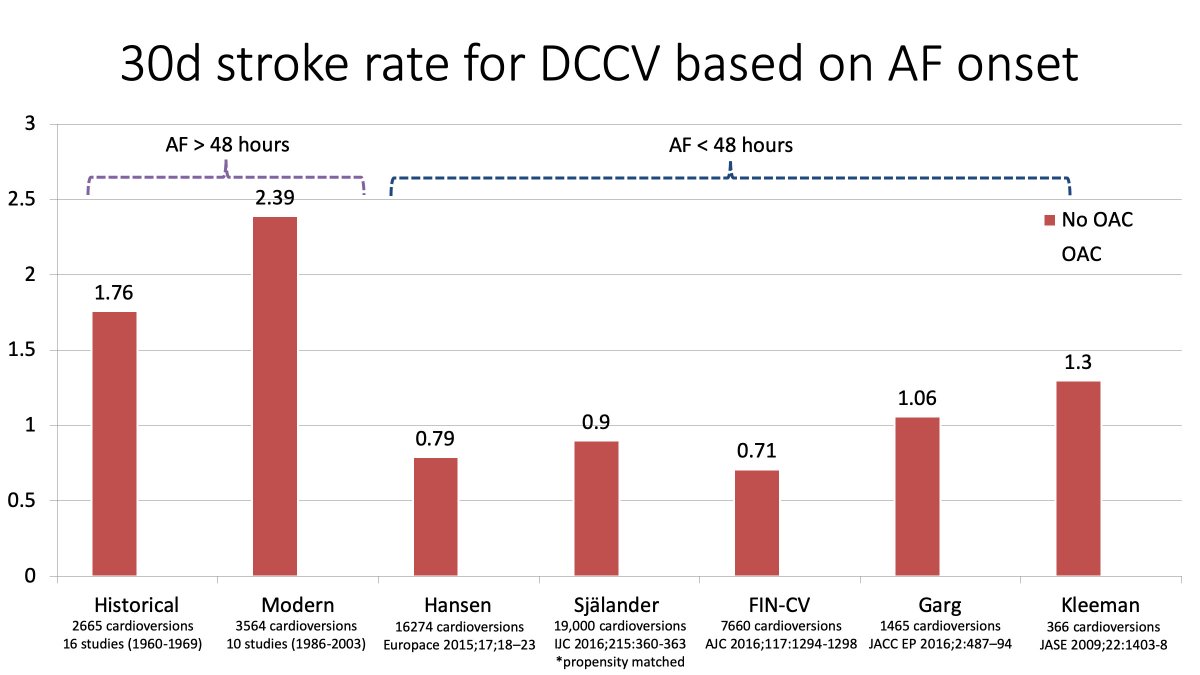
6/ Relevant to this thread - is the observation that cardioversion represents a high risk period for stroke and systemic embolism.
7/ For example, if you look at non-anticoagulated patients there is a 400% increase in the 30 day rate of stroke and systemic embolism following cardioversion (relative to the background 30 day rate of stroke and systemic embolism)
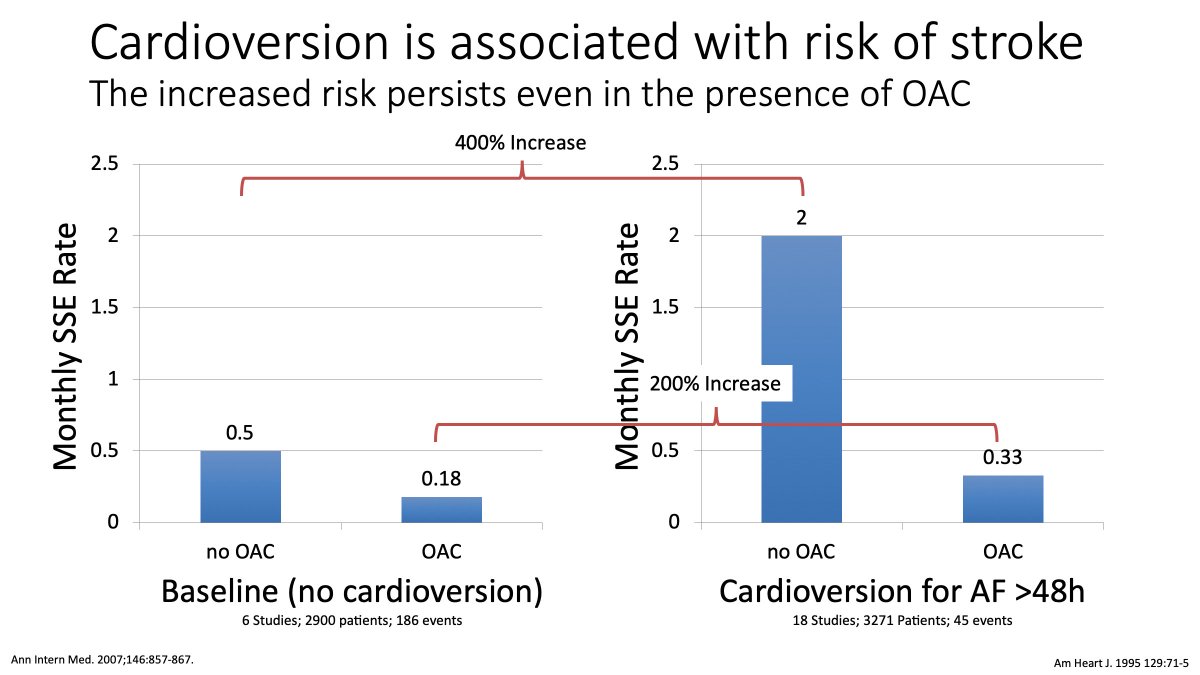
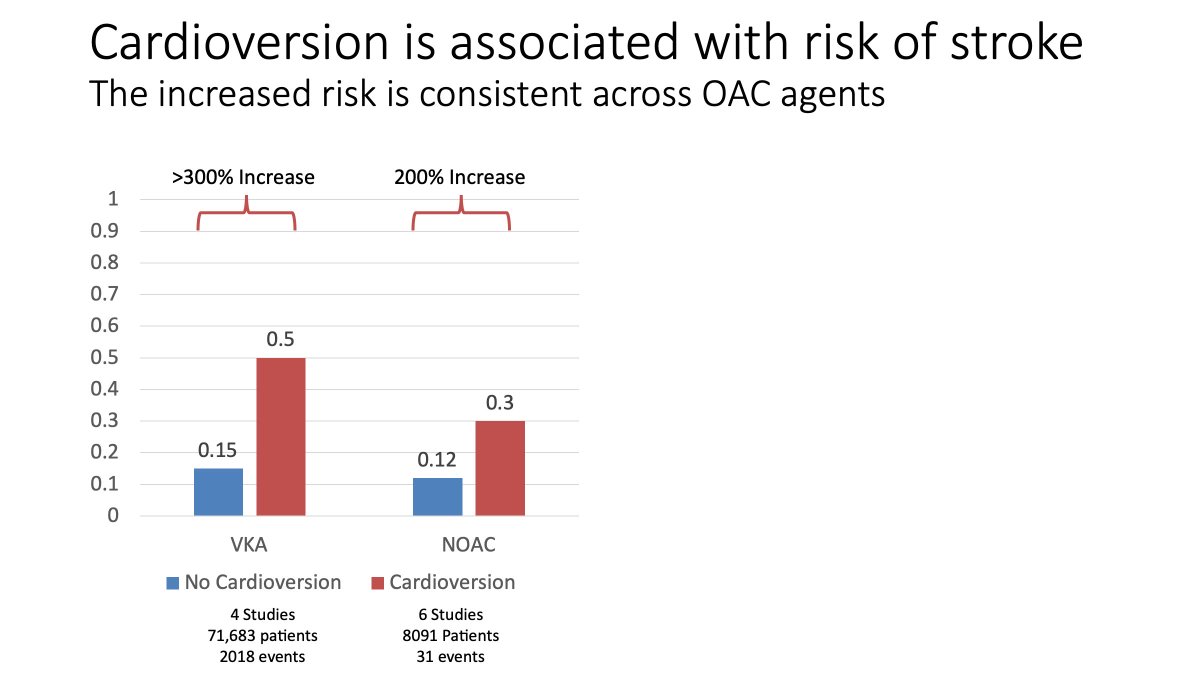
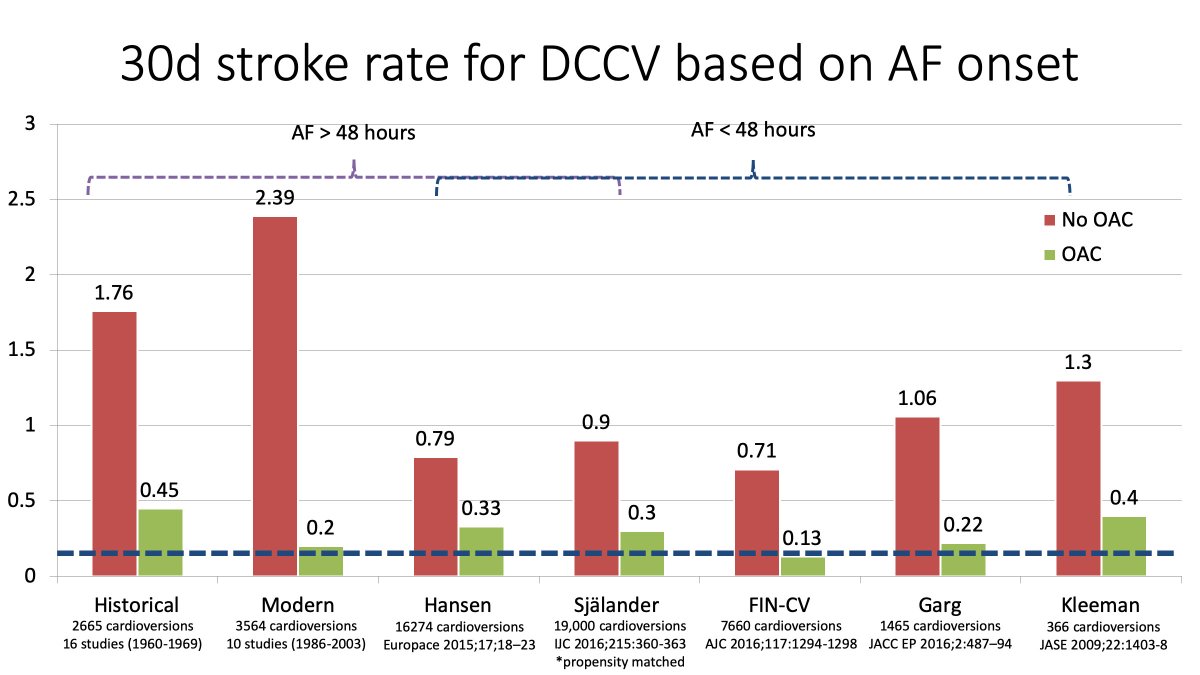
8/ This same pattern applies to those receiving OAC therapy (ie VKA).
Although the magnitude of risk is less when patients are anticoagulated there is still a 200% increase in the risk of stroke and systemic embolism.
Although the magnitude of risk is less when patients are anticoagulated there is still a 200% increase in the risk of stroke and systemic embolism.
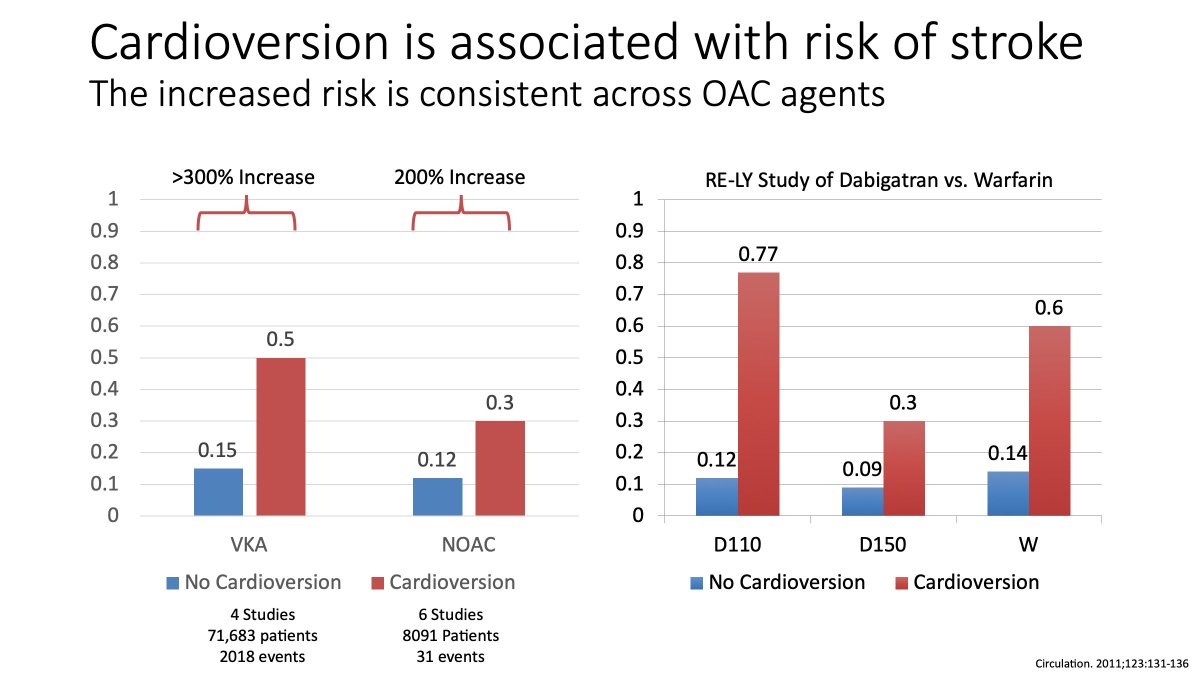
9/ This same pattern is again observed in those treated with VKA vs. NOAC...
10/ ...As well as those receiving varying VKA and NOAC doses.
11/ In other words, all of these studies, with all of these agents, demonstrate a significant increased risk of stroke and systemic embolism in the 30 days following cardioversion.
This suggests that there is a risk inherent to the act of cardioversion.
This suggests that there is a risk inherent to the act of cardioversion.
12/ But. Up until now we've focused on cardioversion itself.
We haven't specifically been speaking to those patients who are OAC naive who present with "Acute AF."
But to discuss this group we need to decide what duration of "Acute AF" is safe to cardiovert.
We haven't specifically been speaking to those patients who are OAC naive who present with "Acute AF."
But to discuss this group we need to decide what duration of "Acute AF" is safe to cardiovert.
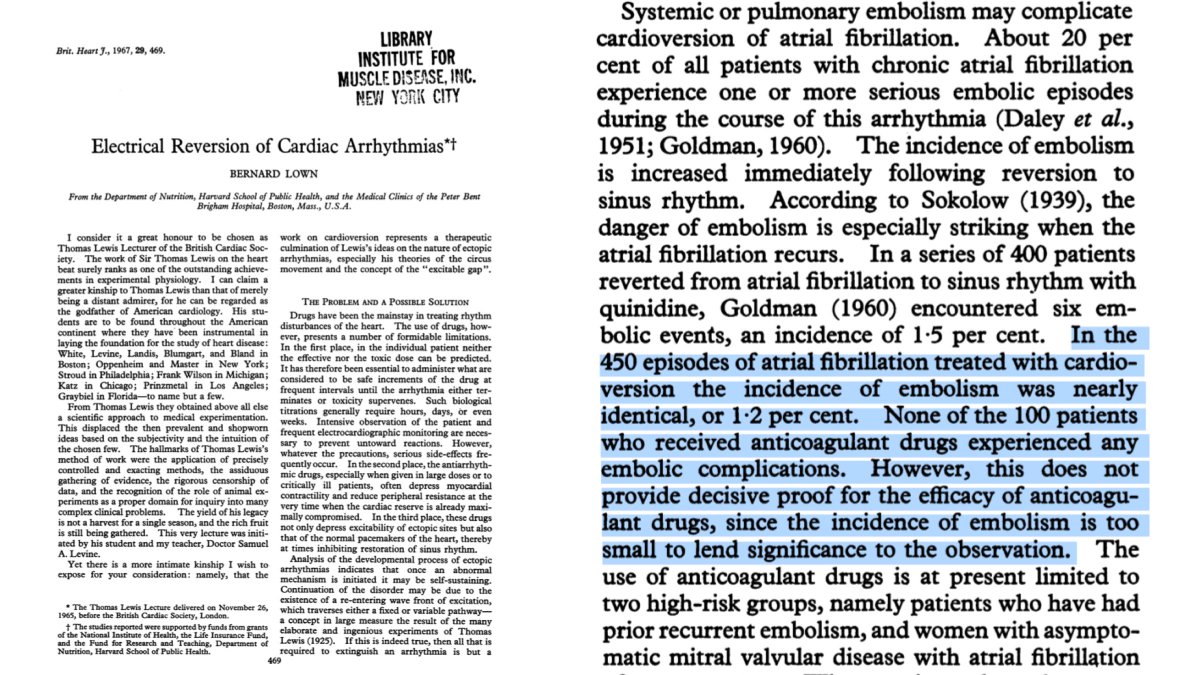
13/ To understand this we have to go back to 1967
Lown observed that: 1) cardioversion was associated with an increased risk of stroke , and 2) patients receiving OAC were at lower risk of stroke.
But they didn't feel that OAC was necessary.
Nor did they mention acute AF
Lown observed that: 1) cardioversion was associated with an increased risk of stroke , and 2) patients receiving OAC were at lower risk of stroke.
But they didn't feel that OAC was necessary.
Nor did they mention acute AF
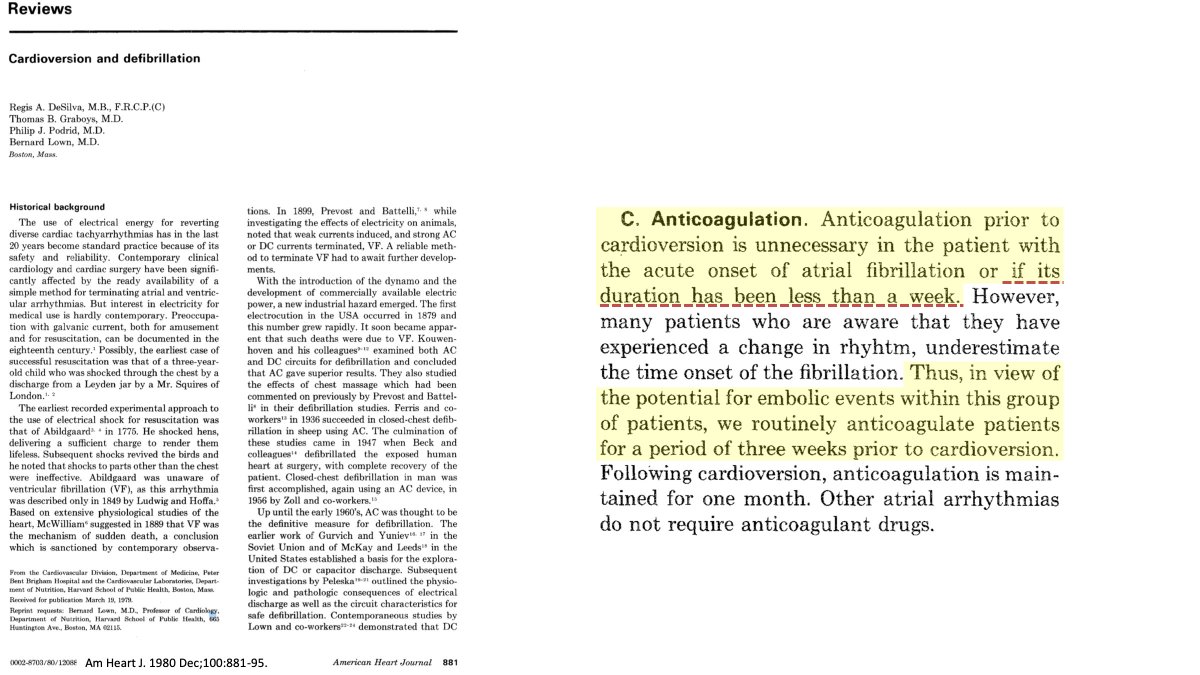
14/ In 1980 Lown et al updated the discussion. In this discussion they indicated that anticoagulation was not necessary if the AF episode duration was <7 days (ie ACUTE).
But they also recommended routine anticoagulation as patients may not recognize the episode onset.
But they also recommended routine anticoagulation as patients may not recognize the episode onset.
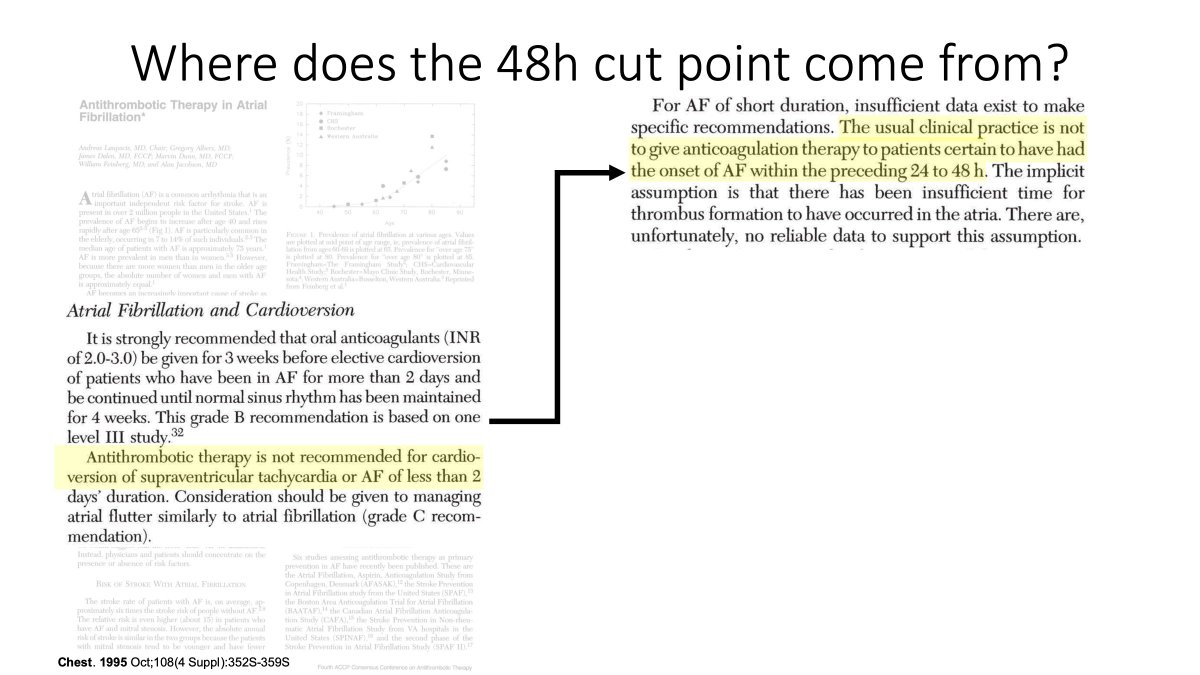
15/ In 1995, the CHEST guidelines revised the ACUTE episode duration down to 48 hours. The recommendation to anticoagulate AF of >48 hour duration was based on a "single level III study"

16/ This study was from 1969. In it the physicians decided to cardiovert everyone presenting to their hospital beginning in February 1964.
If they were on OAC then they continued, if not then NO OAC was given.
The majority of patients were way past the ACUTE AF threshold.
If they were on OAC then they continued, if not then NO OAC was given.
The majority of patients were way past the ACUTE AF threshold.
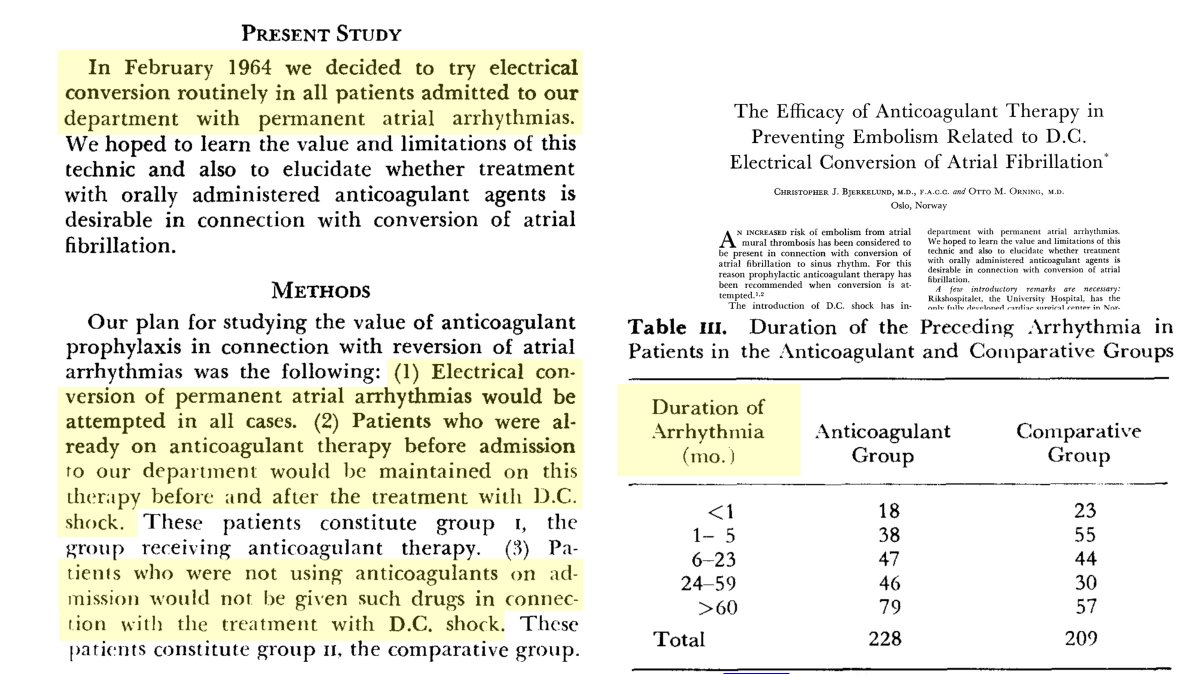
17/ In those not anticoagulated there was a significantly increased risk of stroke relative to those who were receiving OAC therapy. This finding, while not specifically addressing the issue of ACUTE AF, was consistently observed across contemporary studies.
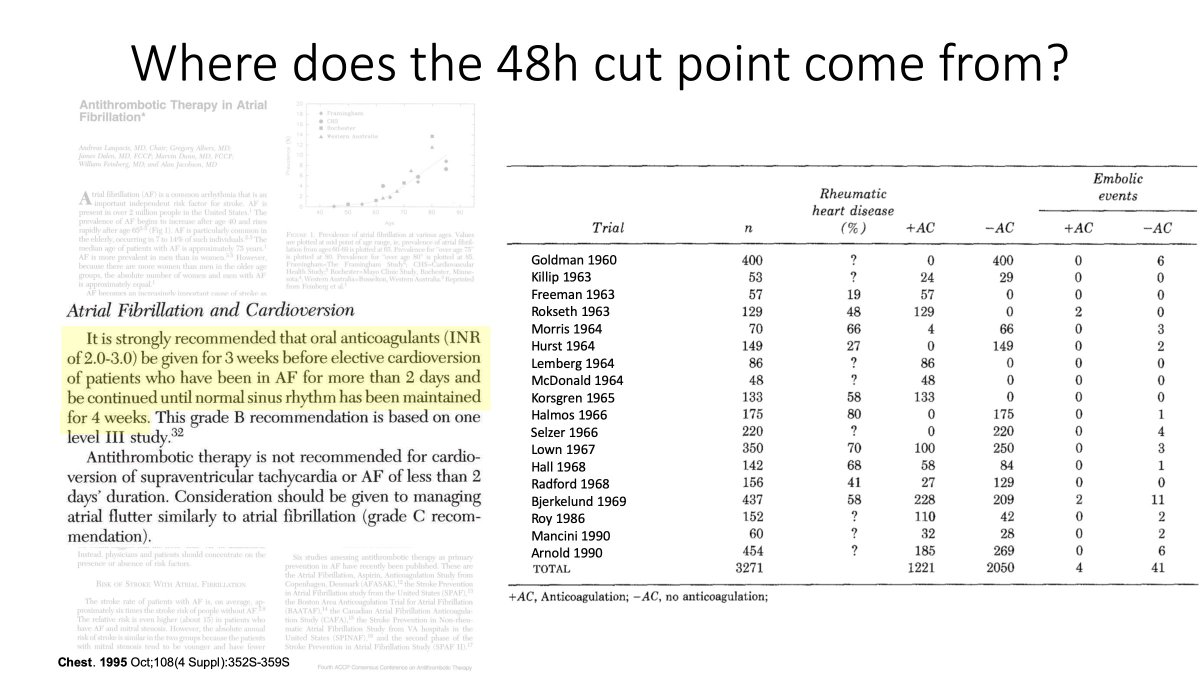
18/ But, we're still not clear on where the 48 hour "safe to cardiovert without OAC" threshold comes from. For that the 1995 CHEST guidelines suggests that it is "usual practice" to not give OAC to those with AF onset < 24-48 hours.
BUT...
BUT...
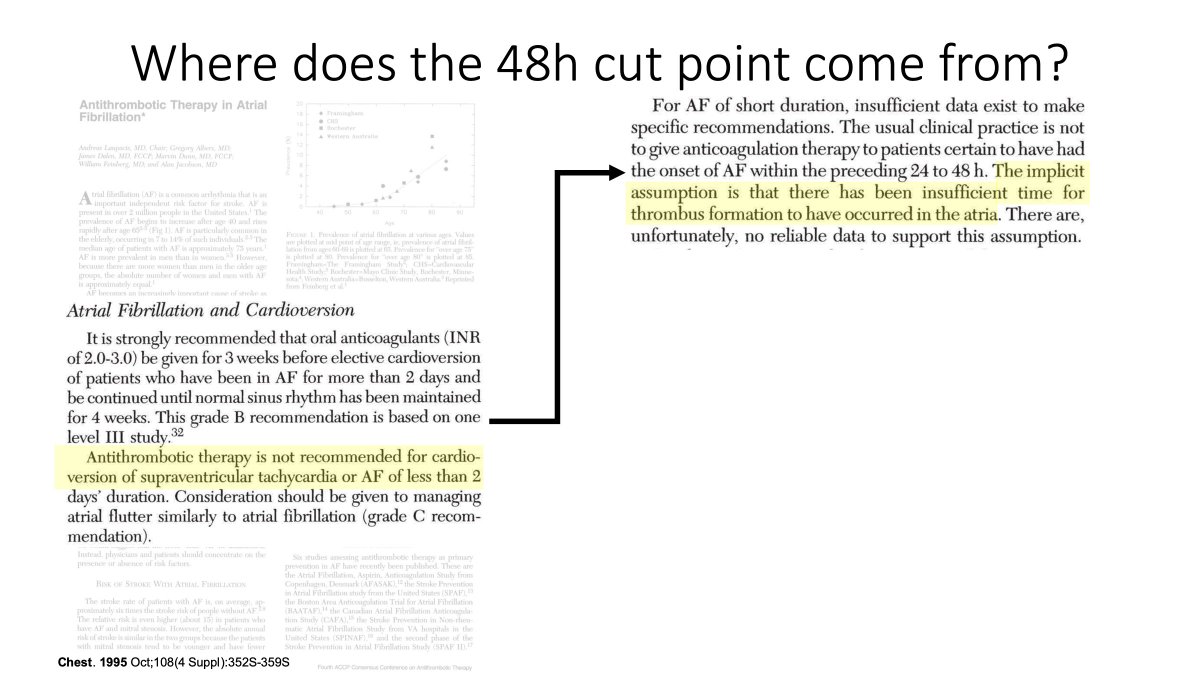
19/ This assertion is based on the assumption that there hasn't been enough time for a clot to form.
The authors note, however, that "there is no reliable data to support this assumption"
The authors note, however, that "there is no reliable data to support this assumption"
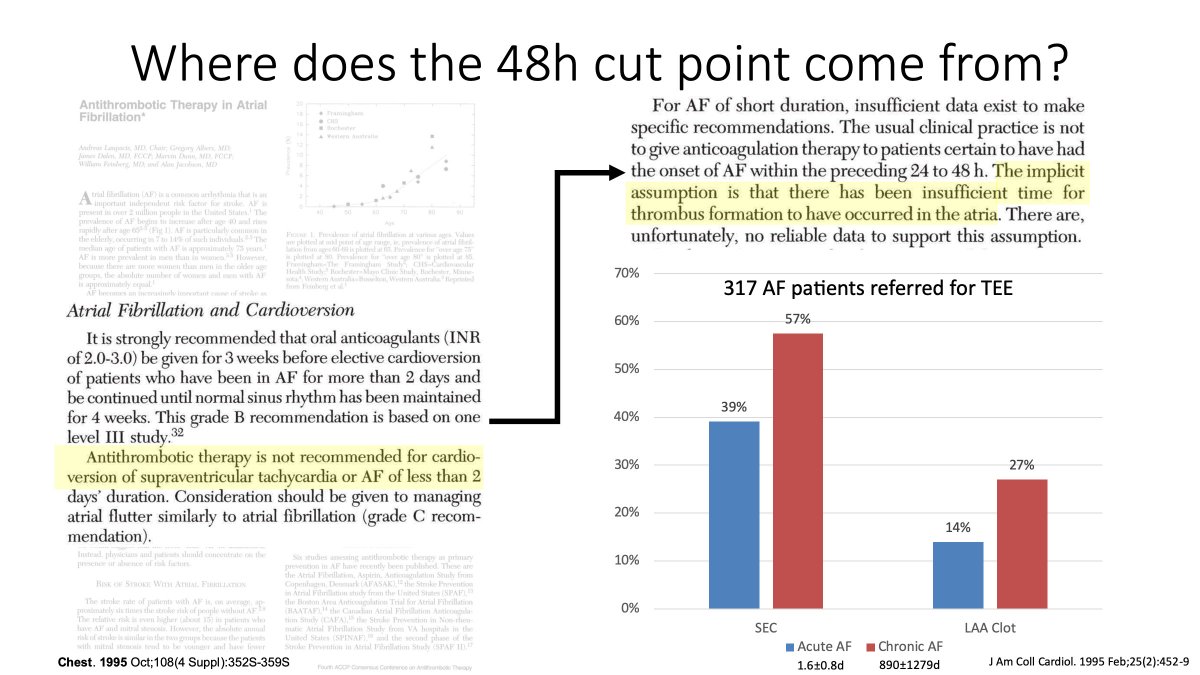
20/ Published that same year, was a study that examined patients with ACUTE and CHRONIC AF referred for cardioversion. In this study patients with ACUTE AF still had a rate of LAA clot of 14%.
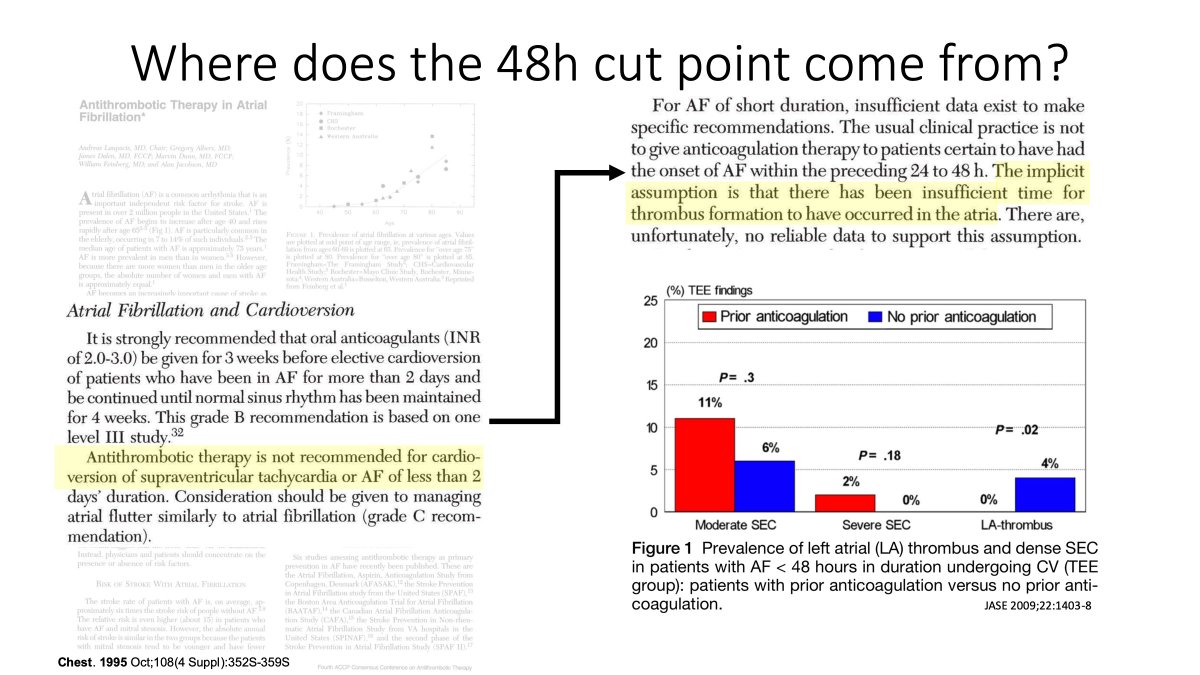
21/ A similar study supported these findings, demonstrating that non-anticoagulated patients with AF of <48 hour duration have a rate of LA clot in the range of 4%.
Meaning, that the assumption that there isn't enough time for clot to form in ACUTE AF is incorrect.
Meaning, that the assumption that there isn't enough time for clot to form in ACUTE AF is incorrect.
22/ In addition, it's important to note that the clot that's present at the time of cardioverison may not be the only reason why patients have a stroke following CV.
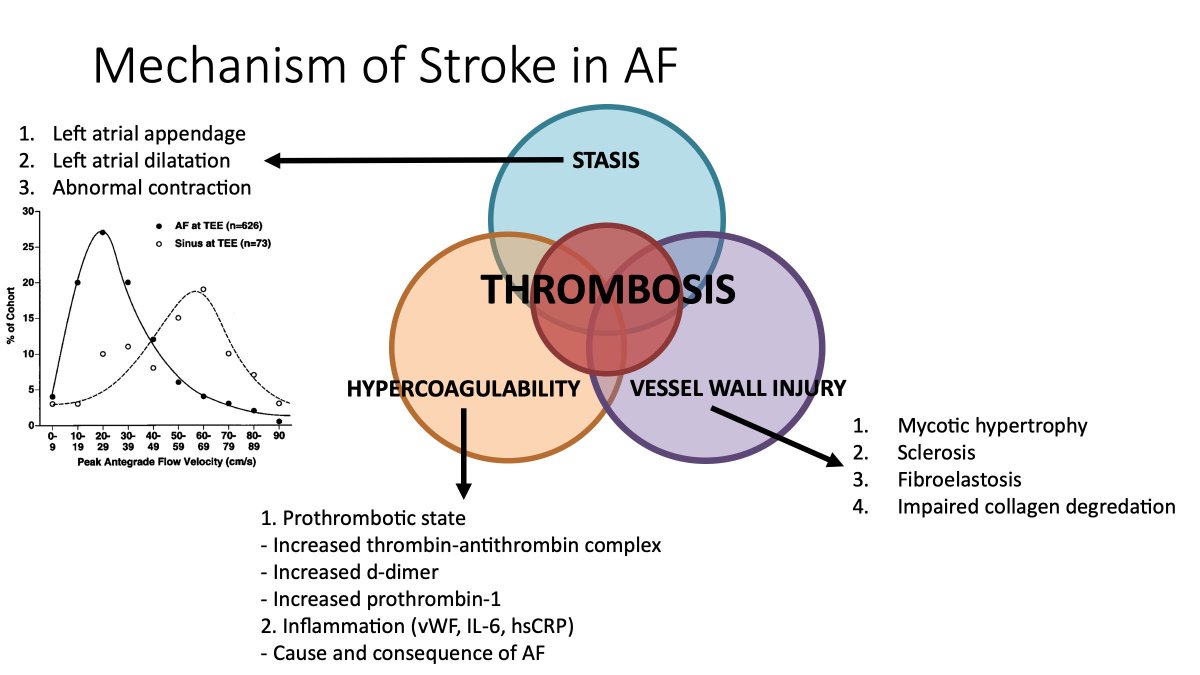
23/ Recall the (simplified) mechanism of stroke in AF. Basically a combination of vessel wall dysfunction/atrial cardiomyopathy, stagnation (LAA/LA contractile dysfunction), and hyper coagulability.
24/ With respect to atrial contractile dysfunction ("stunning").
AF results in a reduction in left atrial appendage contractile function, which is why we think clot forms in the LAA.
AF results in a reduction in left atrial appendage contractile function, which is why we think clot forms in the LAA.
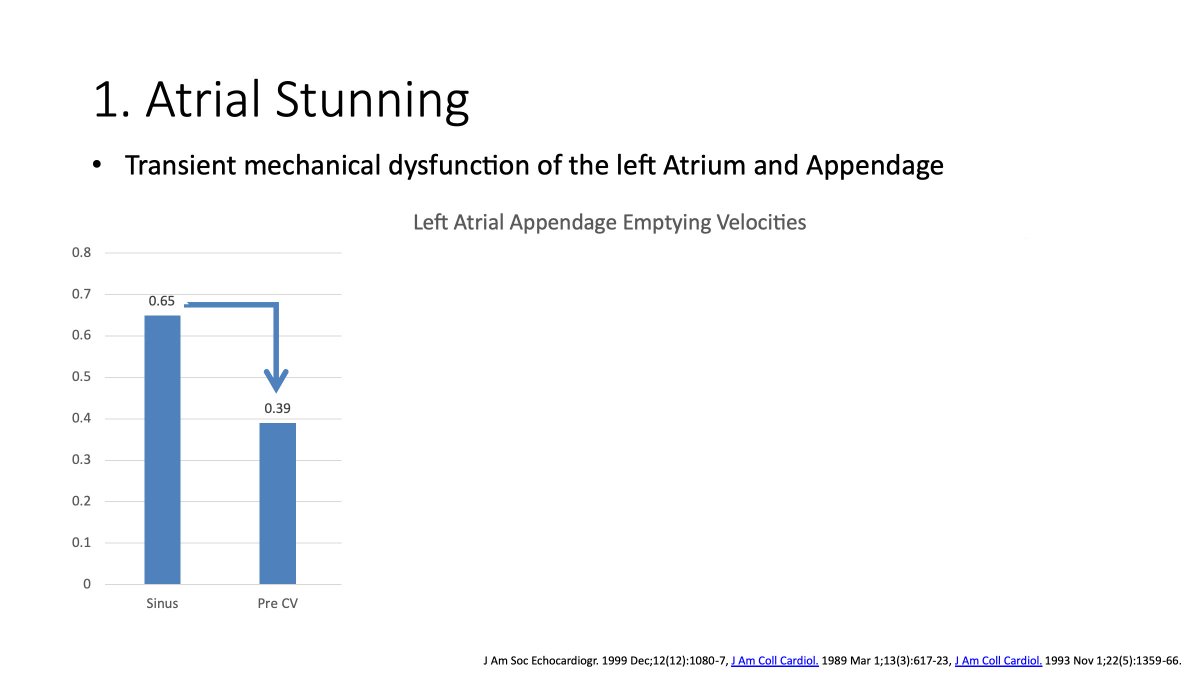
25/ BUT... sinus rhythm restoration results in an acute WORSENING in LA contractile function independent of the mechanism of cardioversion (ie it's observed with spontaneous, pharmacological and electrical conversion).
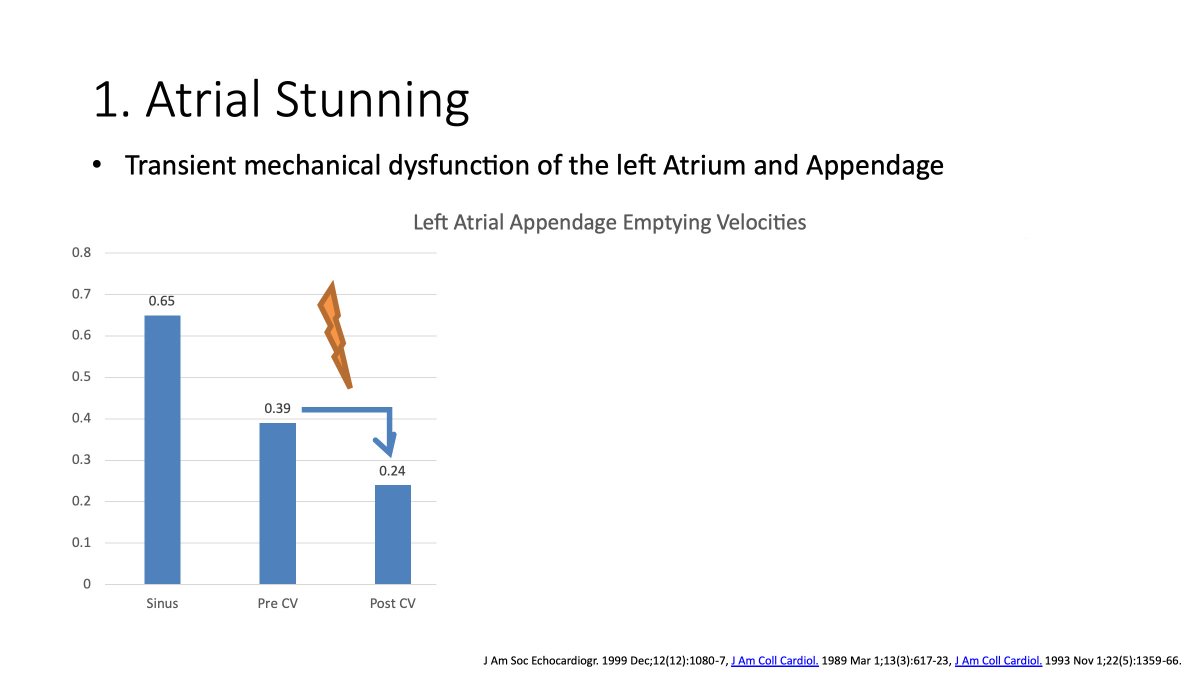
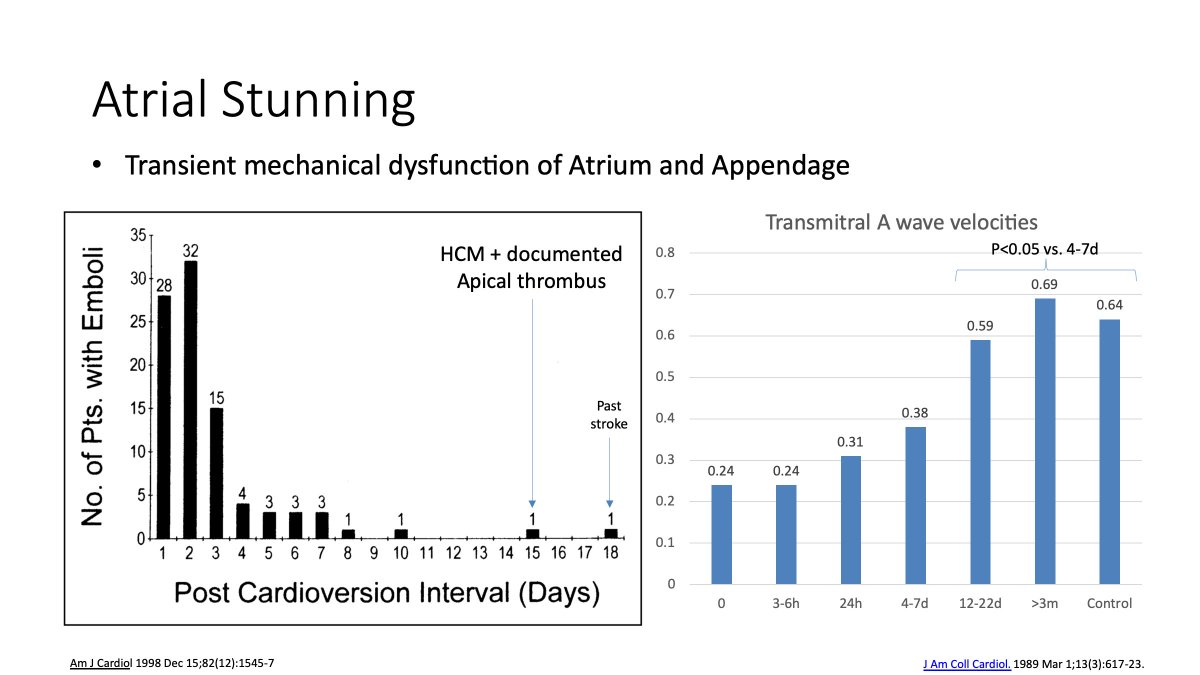
26/ This dysfunction is related to AF episode duration, and can result in a prolonged period of LAA mechanical impairment.
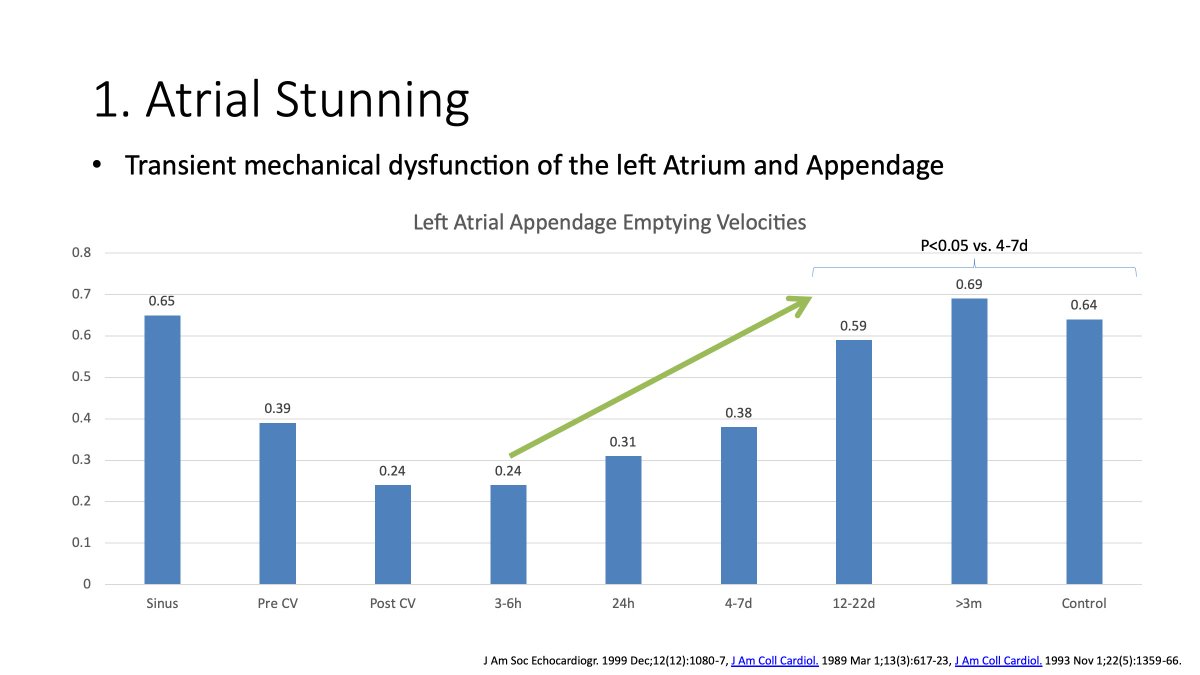
27/ A period that mirrors the incidence and timing of stroke following cardioversion.
Note, the highest rate of stroke is in the first 72 hours following sinus rhythm restoration, with a continued but lower rate out to a week, then essentially nothing following that point
Note, the highest rate of stroke is in the first 72 hours following sinus rhythm restoration, with a continued but lower rate out to a week, then essentially nothing following that point
28/ While I think we are comfortable with the concept of stunning, another interesting and relevant point is the hyper coagulable state induced by AF.
In studies looking at platelet reactivity there is a 2 SD increase in platelet activation beginning 12 hours after AF onset.
In studies looking at platelet reactivity there is a 2 SD increase in platelet activation beginning 12 hours after AF onset.
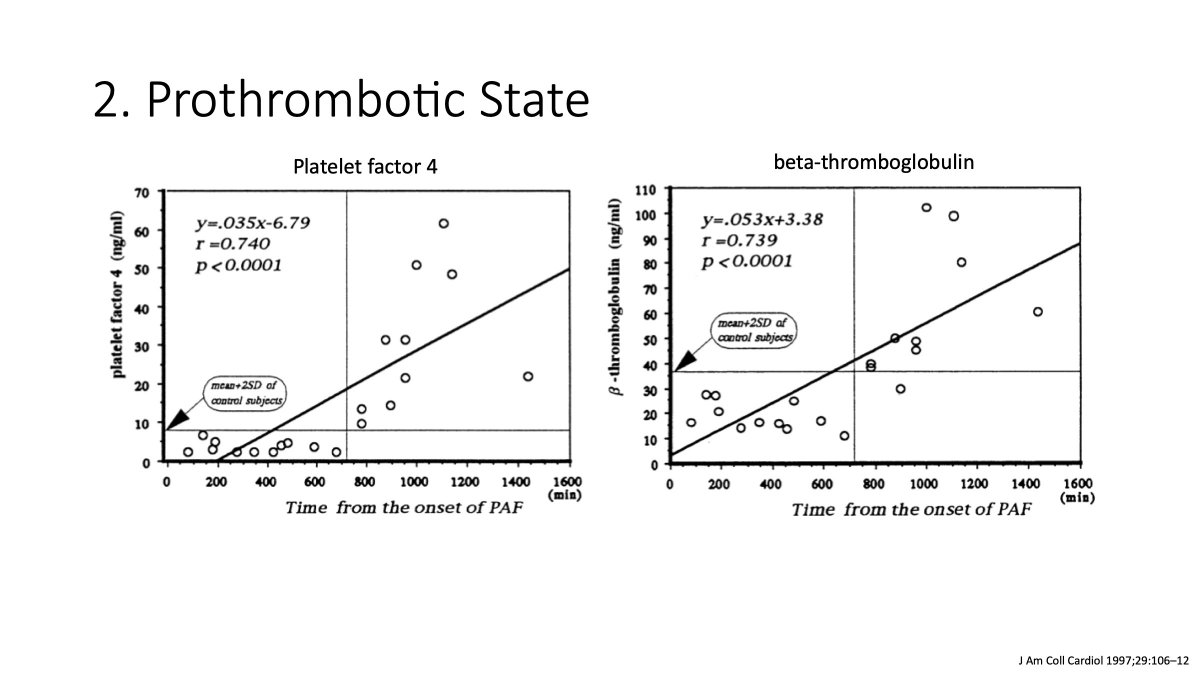
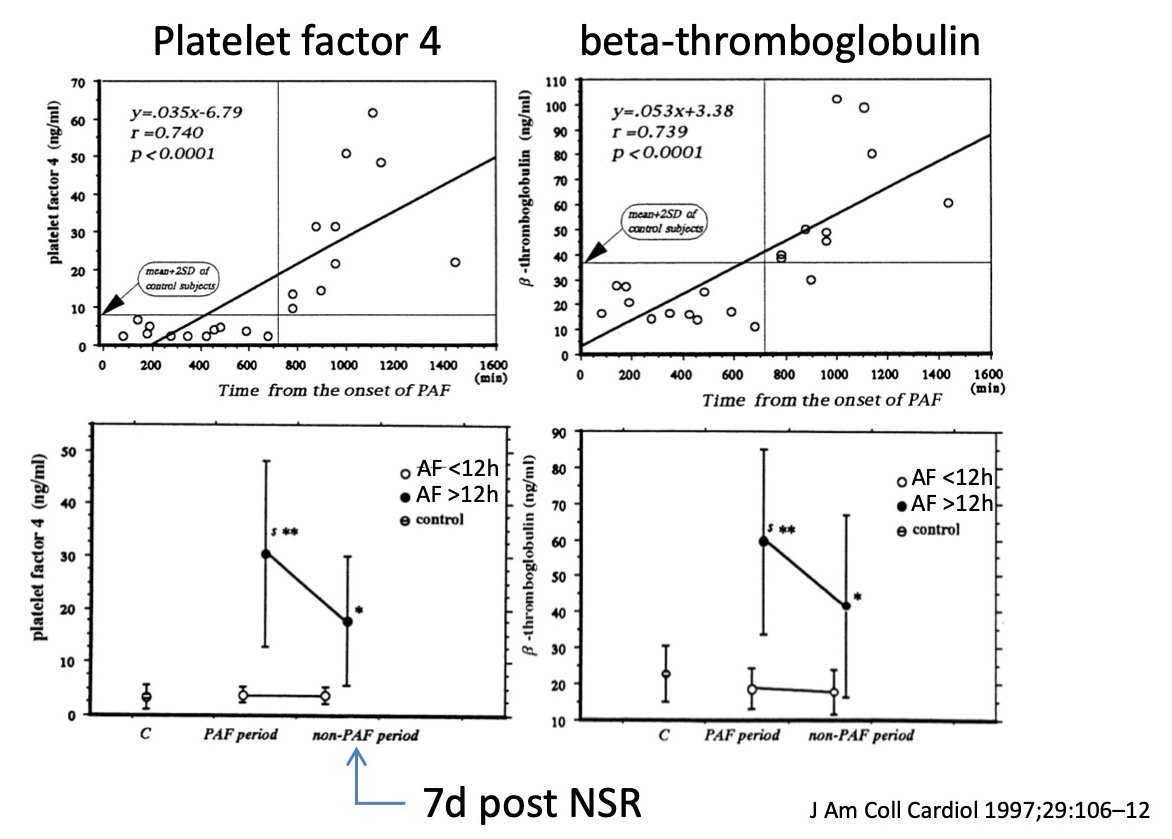
29/ The interesting point here is that the activation in fibrinogen, PF4, thromboglobulin, and TAT
1. only occurs in those with AF episode duration of >12 hours (remember this number) and
2. persists for 7 days AFTER the AF episode is terminated.
1. only occurs in those with AF episode duration of >12 hours (remember this number) and
2. persists for 7 days AFTER the AF episode is terminated.
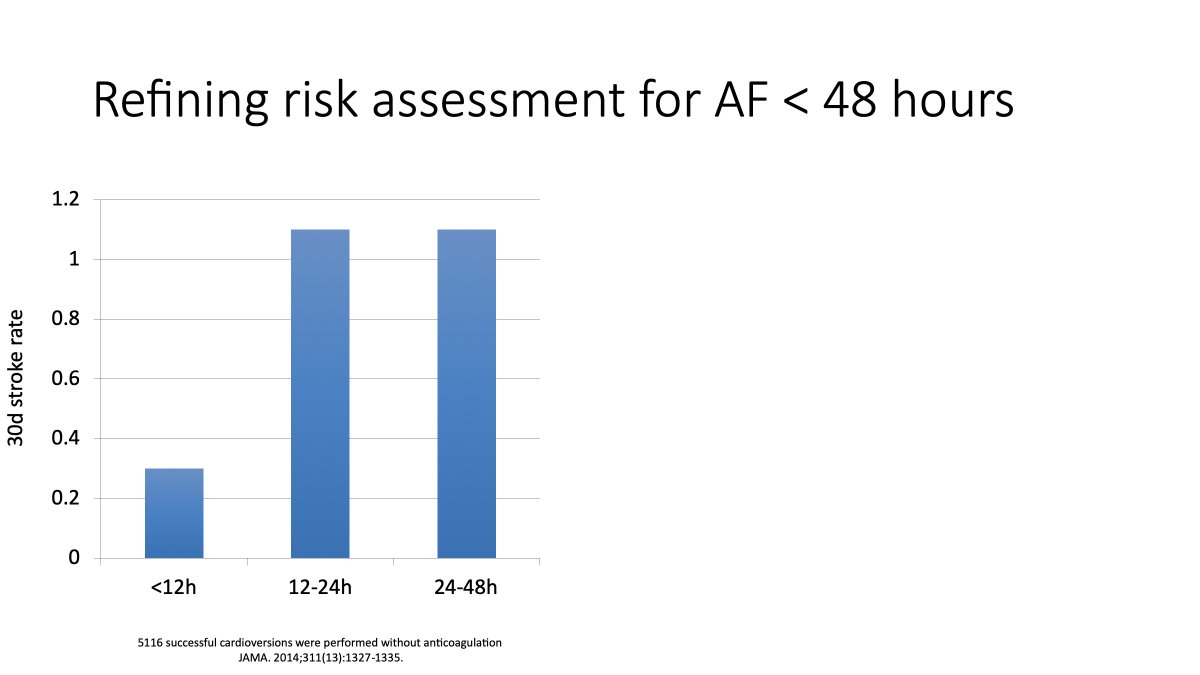
30/ So. To return to the 48 hour cut-off. If this were a "safe period" for cardioversion then there should be an expectation that cardioversion >48 hours after AF episode onset would have a differential rate of stroke at 30 days.
Again, this isn't the case.
Again, this isn't the case.
31/ Moreover, while OAC therapy substantially reduces the risk of stroke and systemic embolism relative to OAC naive patients, the rate of stroke remains above what the @SCC_CCS AF Guidelines committee considers the minimum threshold for OAC initiation for SPAF.
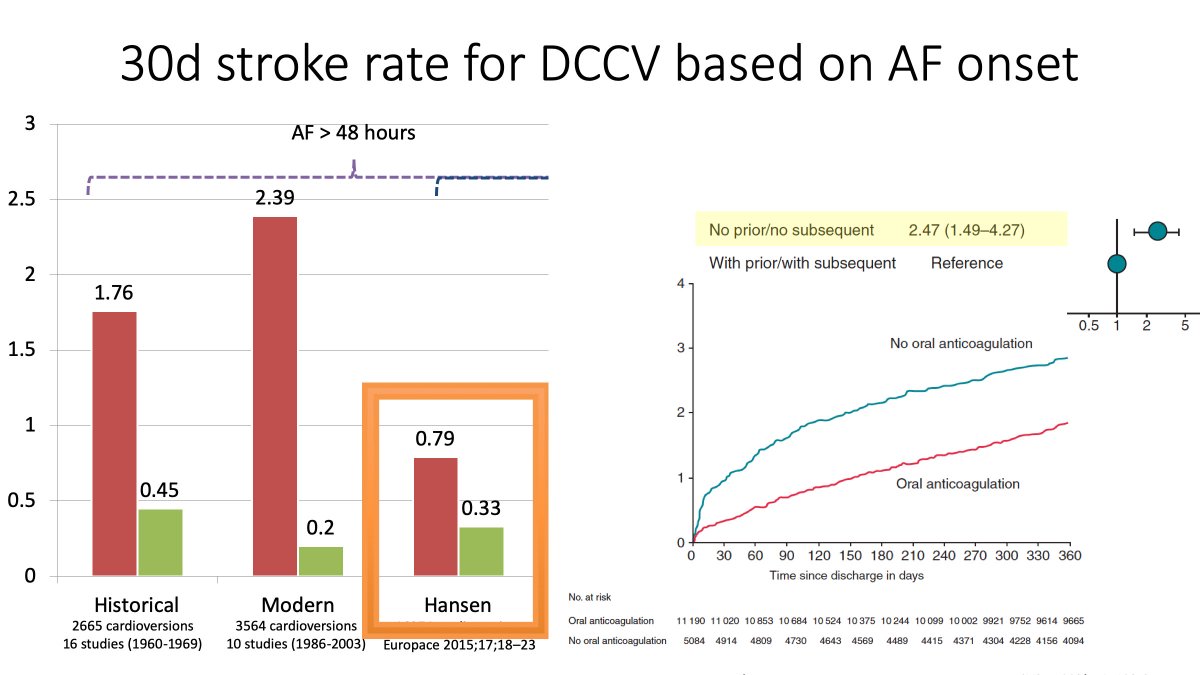
32/ What about those patients coming in who are OAC naive. The Hansen study examined that group and showed that OAC initiation only after CV results in a similar rate of stroke to those receiving OAC pre- and post. This likely reflects the benefit of preventing de novo clot
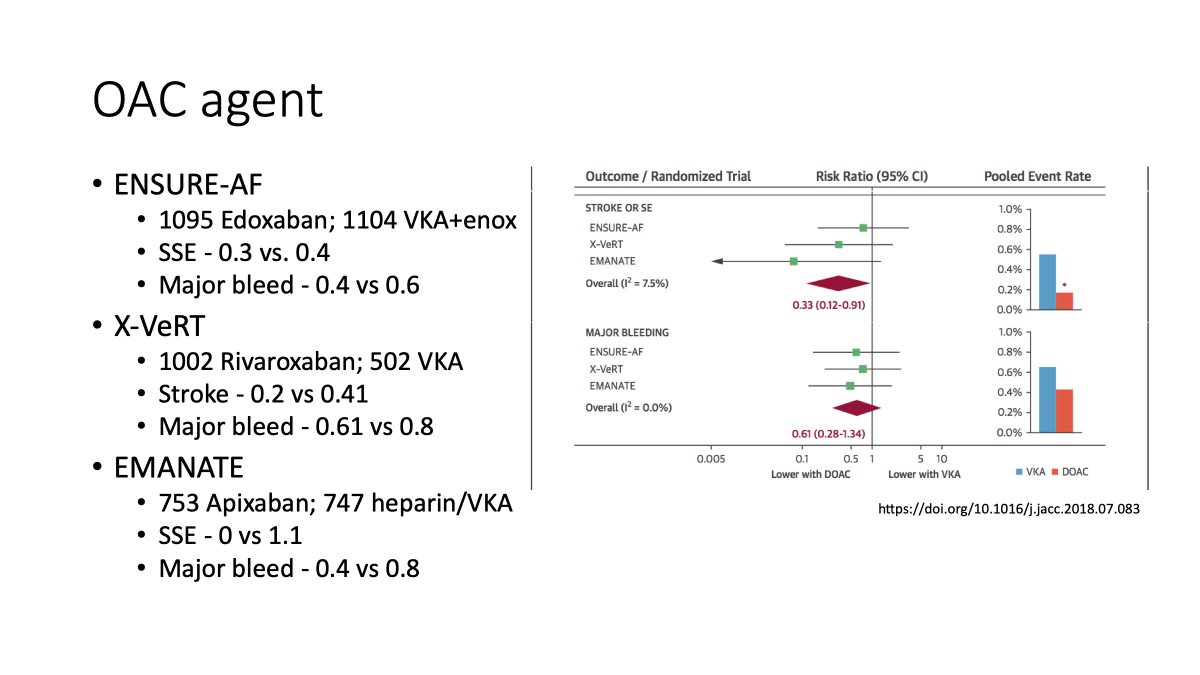
33/ In terms of the agent - the @SCC_CCS AF guidelines does not provide a recommendation about NOAC or VKA. However, if a VKA is chosen then bridging with LMWH is necessary given the early peak in stroke. Conversely, we have some reasonable evidence of benefit for NOAC over VKA.
34/ So. Thats a bit of a review on the CCS AF Guidelines.
We use the 12 hour threshold for patients with risk factors.
But also recommend OAC for all after pharmacologic or DC cardioversion
More can be found in the following:
onlinecjc.ca/article/S0828-…
onlinecjc.ca/article/S0828-…
We use the 12 hour threshold for patients with risk factors.
But also recommend OAC for all after pharmacologic or DC cardioversion
More can be found in the following:
onlinecjc.ca/article/S0828-…
onlinecjc.ca/article/S0828-…
35/ I lost steam yesterday.
But thought I'd come back to address a couple of lingering points/questions.
The first is the 12h threshold.
I alluded to this previously in the comment about platelet activation. Interestingly, the risk of clinical SSE follows this same time course.
But thought I'd come back to address a couple of lingering points/questions.
The first is the 12h threshold.
I alluded to this previously in the comment about platelet activation. Interestingly, the risk of clinical SSE follows this same time course.
36/ This increase is less dramatic in those without risk factors, BUT there is still a tangible risk of stroke in the 30d following CV in those with no stroke risk factors presenting <12 hours after AF onset. And that risk is above the accepted monthly risk threshold for OAC.
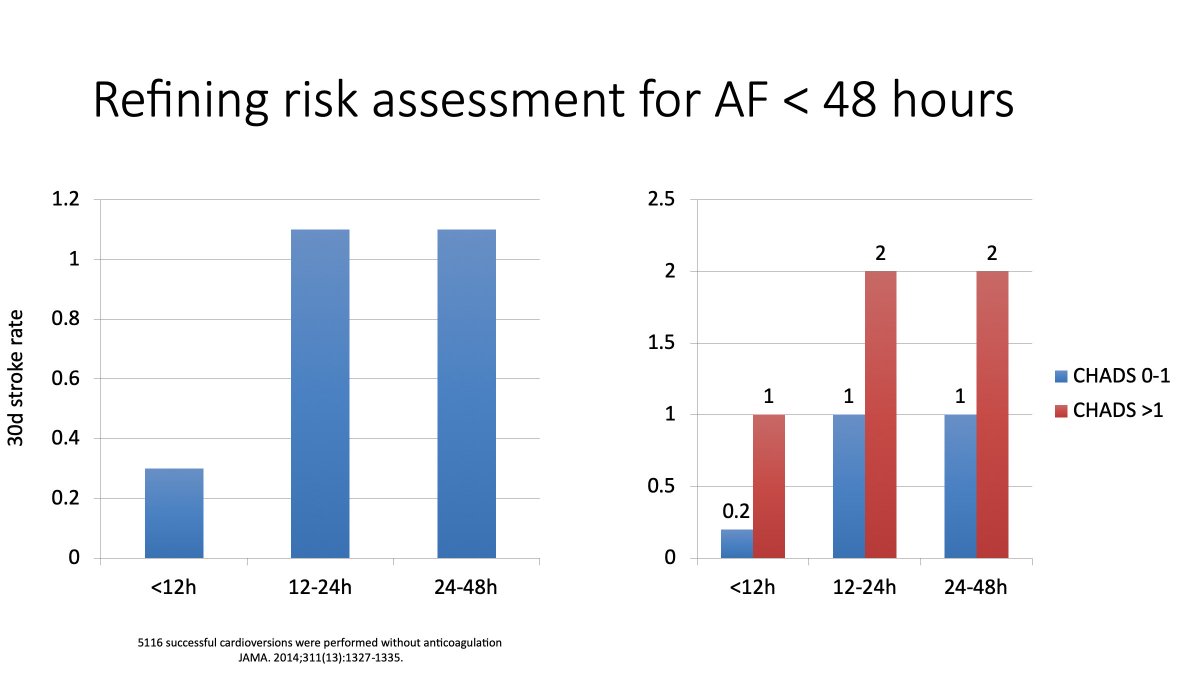
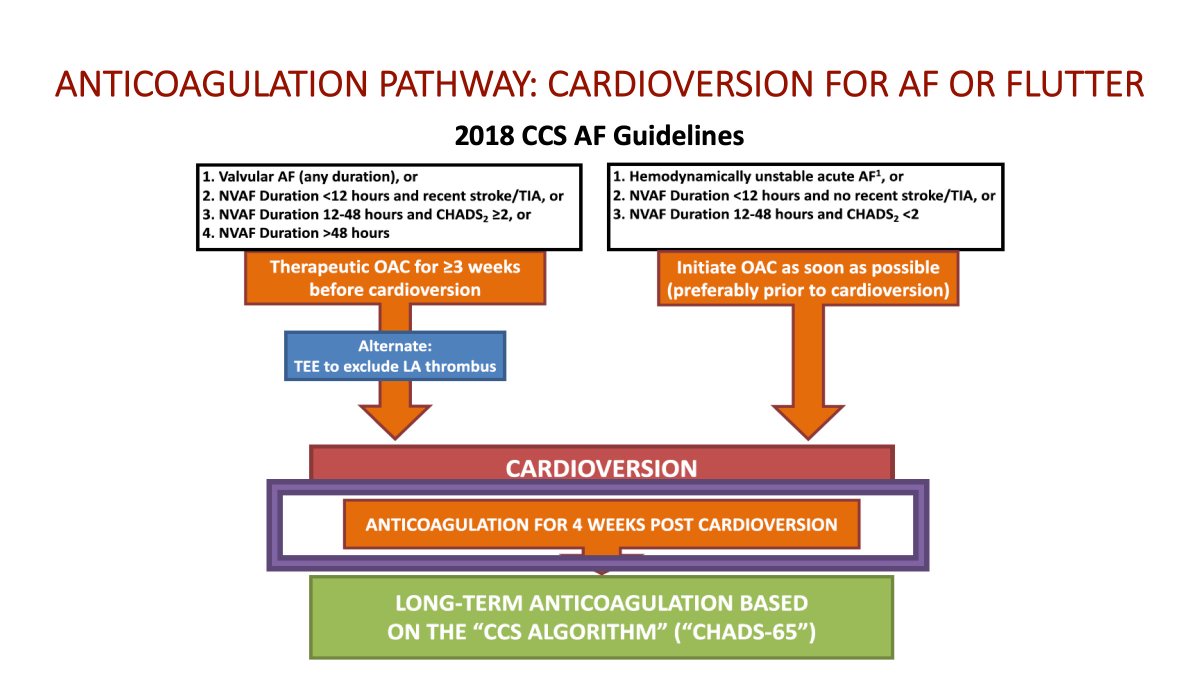
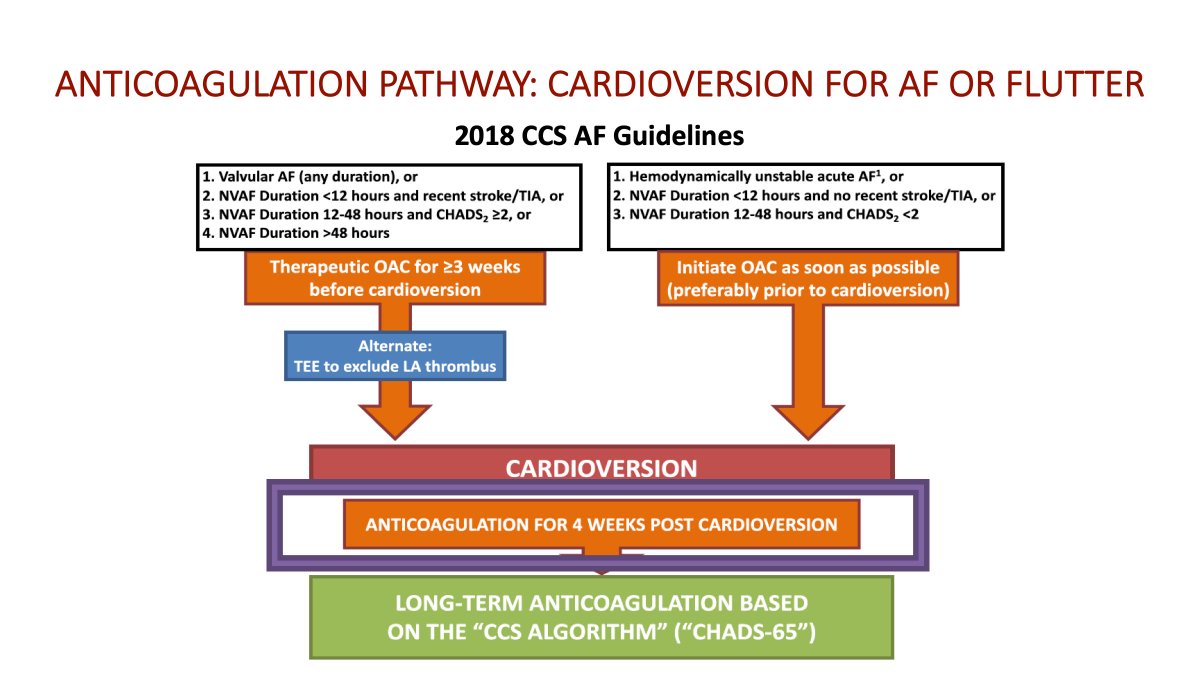
37/ So if we go back to the CCS algorithm.
The decision to proceed with cardioversion is dependent on both the episode duration AND the patients risk of stroke:
- presentation early is generally ok to proceed
- presentation late necessitates some trepidation, if RF presentation
The decision to proceed with cardioversion is dependent on both the episode duration AND the patients risk of stroke:
- presentation early is generally ok to proceed
- presentation late necessitates some trepidation, if RF presentation
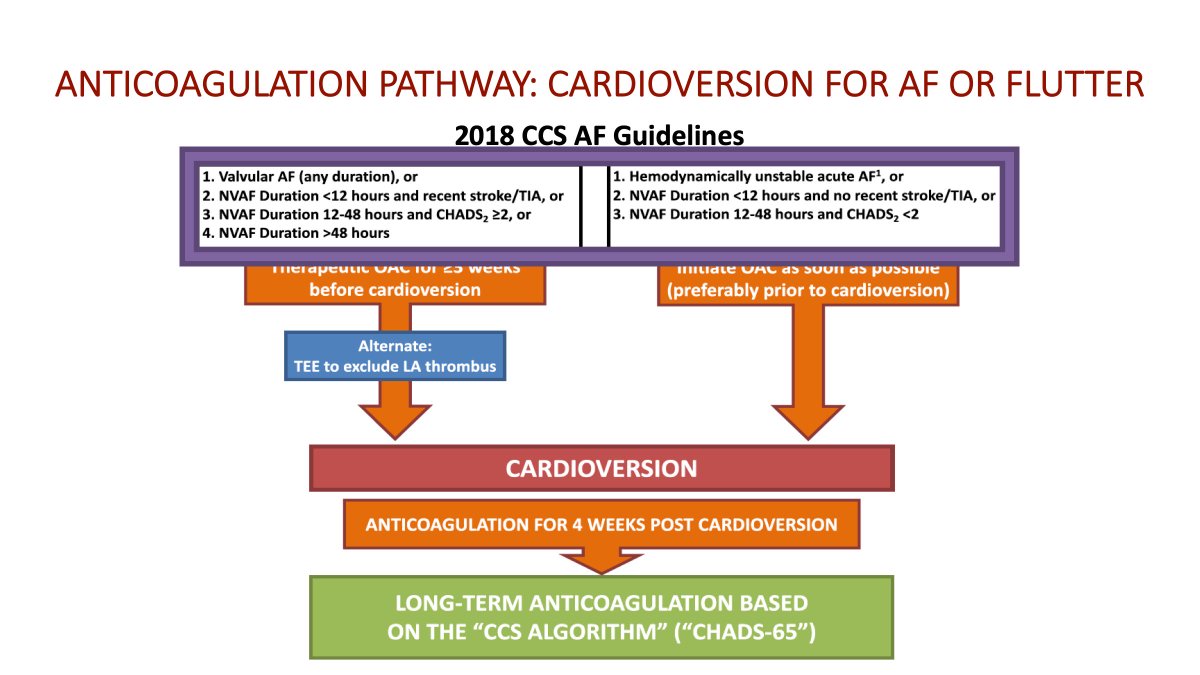
38/ But, all patients would leave the department on therapeutic OAC for a minimum of 30 days given the risk of developing clot following sinus rhythm restoration (as outlined above).
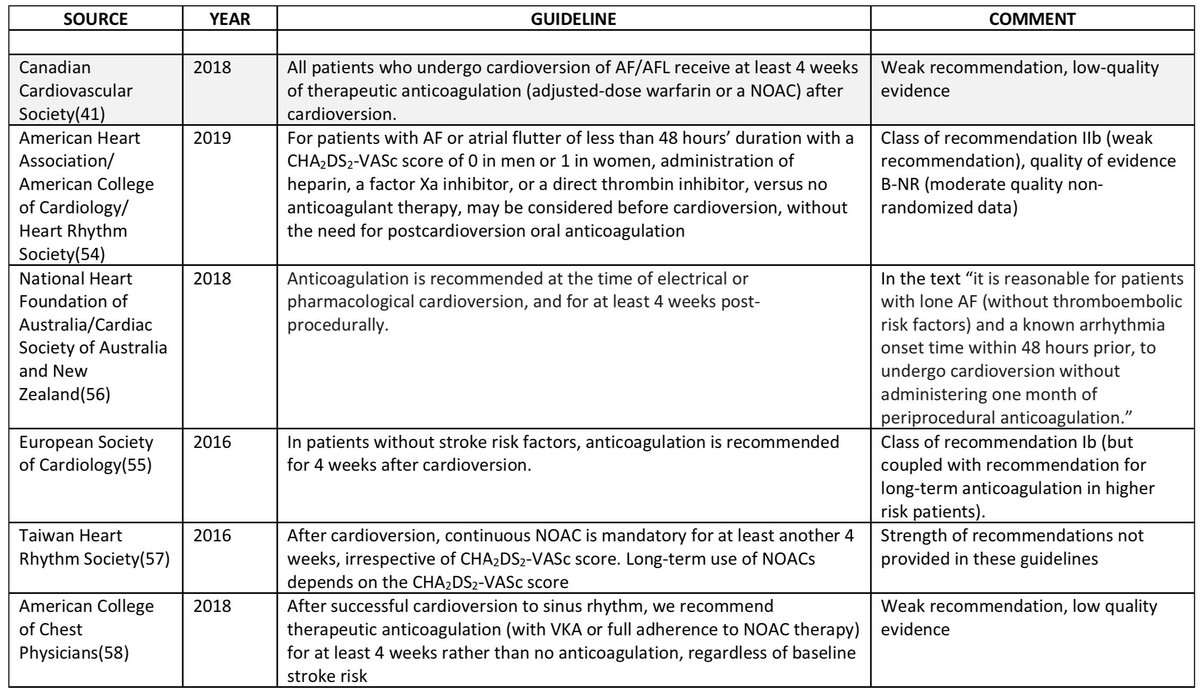
39/ So where do the @SCC_CCS AF guidelines land relative to other societies?
We are more restrictive than most about early cardioversion, suggesting stroke risk be assessed for those presenting between 12-48 hours.
Most other societies would suggest proceeding if AF episode <48h
We are more restrictive than most about early cardioversion, suggesting stroke risk be assessed for those presenting between 12-48 hours.
Most other societies would suggest proceeding if AF episode <48h

40/ With respect to the need for post-cardioversion OAC the @SCC_CCS AF guidelines are in line with the @escardio, CHEST, and @thecsanz guidelines.
In this case it is the @ACCinTouch @American_Heart who do not advocate for a period of post cardioversion OAC therapy
In this case it is the @ACCinTouch @American_Heart who do not advocate for a period of post cardioversion OAC therapy