
,
27 tweets,
8 min read
Read on Twitter
So hey #medtwitter, I know that Invega and Zyprexa and Saphris are new sexy drugs, but for bipolar disorder, have you considered lithium? Yeah, I know, that drug rep WAS pretty hot... but... this medication deserves a rep.
LITHIUM MEGATHREAD!!
#somepsych #psychtwitter #MedEd
LITHIUM MEGATHREAD!!
#somepsych #psychtwitter #MedEd
I'm nowhere near sexy enough to be hired by a Pharma company, but allow me to be that rep.
(This is particularly targeted at my American psychiatric colleagues, who for whatever reason seem quite enthralled with every new medication that comes down the pipeline)
(This is particularly targeted at my American psychiatric colleagues, who for whatever reason seem quite enthralled with every new medication that comes down the pipeline)
The last decade has brought out SO MUCH EVIDENCE for Lithium (Li+) in bipolar disorder (BD). Many old ideas about Li+ have changed, and our knowledge has just gotten so much stronger.
MECHANISM OF ACTION:
We still don't know!
Current top candidates include:
* membrane transport (Na+/K+ ATPase)
* increase neurotransmitter signalling
* stimulates inhibitory transmitters
* 2nd messenger systems galore!
We still don't know!
Current top candidates include:
* membrane transport (Na+/K+ ATPase)
* increase neurotransmitter signalling
* stimulates inhibitory transmitters
* 2nd messenger systems galore!
However, the science is on it! The number of articles investigating the biological effects of lithium in bipolar disorder is skyrocketing! The next decade will likely be very helpful to understanding Lithium.
Graph: # of Li+ mechanism publications over time
Graph: # of Li+ mechanism publications over time

SAFETY:
Li+ has very predictable toxicity, and understanding the lithium toxidrome is important to using litihum.
However, some of the "cautions" about Lithium are very "work-aroundable".
Tremor, for example, can often be solved by lowering the dose of lithium (0.6 mEq/L).
Li+ has very predictable toxicity, and understanding the lithium toxidrome is important to using litihum.
However, some of the "cautions" about Lithium are very "work-aroundable".
Tremor, for example, can often be solved by lowering the dose of lithium (0.6 mEq/L).

Lithium is likely neuroprotective and antisuicidal. It could actually significantly improve safety to be on Li+.
There are real concerns, hypothyroidism (about 14% of pts, but very manageable), and hypoparathyroidism (monitor calcium).
There are real concerns, hypothyroidism (about 14% of pts, but very manageable), and hypoparathyroidism (monitor calcium).
Famously, Lithium is metabolized by the kidney. A 2018 15-year (!) follow-up study showed that the cases that can reduce kidney function were strated >40 years of age, and no patients experienced end-stage renal failure.
Monitor kidney function, and it'll probably be OK.
Monitor kidney function, and it'll probably be OK.
But I started this by comparing to the antipsychotic class! C'mon, are we really going to try and say APs are safer?
In BD, outcomes of nontreatment are horrific & include suicide, major social disruptions, and hospitalization.
Li+ likely has the BEST safety profile.
In BD, outcomes of nontreatment are horrific & include suicide, major social disruptions, and hospitalization.
Li+ likely has the BEST safety profile.
(Pregnancy)
This 2018 6-cohort metaanalysis concluded "Li+ was not associated with any of the predefined pregnancy complications or delivery outcomes."
Post-hoc: readmission, malformations may be increased (Graph)
This 2018 6-cohort metaanalysis concluded "Li+ was not associated with any of the predefined pregnancy complications or delivery outcomes."
Post-hoc: readmission, malformations may be increased (Graph)

Still a class D medication for pregnancy, so one that requires clinical consideration. Balancing Bipolar distress vs Li+ in pregnancy is still a hard task. Remember, THE most unstable time is postpartum, and lithium during prevents bipolar illness.
EFFICACY (ADULT)
PLEASE CONSIDER LITHIUM FOR MONOTHERAPY
It's cheaper. It's the most evidenced. It has the least pharma bias. It has established levels. Informed consent is fully achievable.
A 2018 nationwide cohort found that Li+ outperformed APs on rehospitalization.
PLEASE CONSIDER LITHIUM FOR MONOTHERAPY
It's cheaper. It's the most evidenced. It has the least pharma bias. It has established levels. Informed consent is fully achievable.
A 2018 nationwide cohort found that Li+ outperformed APs on rehospitalization.

A 2014 Network Analysis stated: "[Li+] is one of the most effective treatments in the prevention of both manic & depressive episodes, with the most robust & unbiased evidence, with a higher rate of adverse events than placebo, [but not more dropout]"
Graph: the network analysis
Graph: the network analysis

A 2015 meta-analysis went back to old lithium studies and established how well it works vs. placebo.
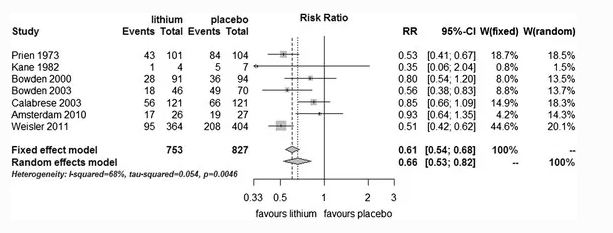
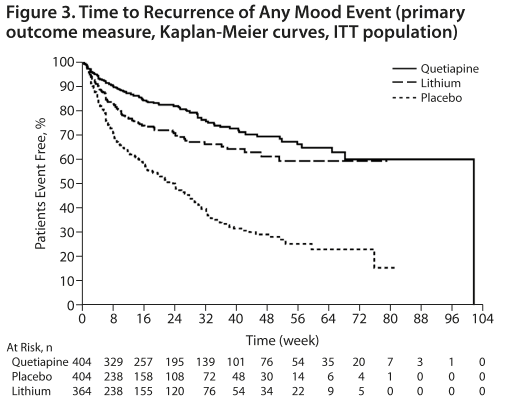
And while the CHOICE in 2016 trial showed that Quetiapine = Lithium in the first 26 weeks; look what this 2017 ASTRAZENICA FUNDED (kudos, a negative study that was published!) trial showed for the weeks that followed.
Graph: Boom, that's not good.
Graph: Boom, that's not good.

Note: this is hard to reconcile with Weisler 2011, where this was not seen. But... that was QUET-->QUET/Li/Placebo, and some of the Li+ dip initially could have been withdrawal from QUET. The 2017 study started with QUET+Li, then randomly discontinued either. Better design.
I know this goes against many guidelines (like CANMAT) to put Lithium>other "1st line agents", but please hear this from a clinician who has full informed consent patient with many families affected by BD:
IF YOU SEE CLASSIC BIPOLAR DISORDER, USE THE CLASSIC TREATMENT (Li+)
IF YOU SEE CLASSIC BIPOLAR DISORDER, USE THE CLASSIC TREATMENT (Li+)
EFFICACY (CHILD+ADOLESCENT)
A 2019 study showed that removing Li+ from children with BD who were previously stabilized on 24 weeks of lithium fared much worse. This graph shows the return of mood symptoms of Li+ vs placebo over 28 weeks.
A 2019 study showed that removing Li+ from children with BD who were previously stabilized on 24 weeks of lithium fared much worse. This graph shows the return of mood symptoms of Li+ vs placebo over 28 weeks.

Another brand new study (2019) showed that compared to other mood stabilizers, children receiving lithium had less suicide attempts, fewer depressive symptoms, less psychosocial impairment, and less aggression.
(by the way, if you are using Risperidone as a first line agent because of Geller 2012 - stay tuned for a later thread, as I describe it as one of the WORST BIPOLAR ARTICLES OF ALL TIME.)
In kids, if they are BIPOLAR (you know, manic and depressive, not "aggressive"), use Li+
In kids, if they are BIPOLAR (you know, manic and depressive, not "aggressive"), use Li+
EFFICACY (OLDER ADULT)
Li+ is the GOLD STANDARD for bipolar disorder in older adults. While GERI-BD (2017) was a bit equivocal, a 281 cohort study showed rather convincingly that OA's with Li+:
* reduced depression
* required less benzo
* had no renal impairment
Li+ is the GOLD STANDARD for bipolar disorder in older adults. While GERI-BD (2017) was a bit equivocal, a 281 cohort study showed rather convincingly that OA's with Li+:
* reduced depression
* required less benzo
* had no renal impairment
In Summary:
Probably the only reason Li+ isn't used more is because of:
* lack of Pharma backing
* lack of seductive pharma advertising (people + events)
* overestimation of Li+ risk / underestimation of AP risk
Lithium is an EXCELLENT drug for Bipolar Disorder.
$0.21/pill!
Probably the only reason Li+ isn't used more is because of:
* lack of Pharma backing
* lack of seductive pharma advertising (people + events)
* overestimation of Li+ risk / underestimation of AP risk
Lithium is an EXCELLENT drug for Bipolar Disorder.
$0.21/pill!
References attached. This is my first time doing a "evidence update" on Twitter, not sure how else to do references.
Images were snipped when open access seemed available, and re-presented using excel when not.
Images were snipped when open access seemed available, and re-presented using excel when not.

Sorry I can't be as good looking as the Rexulti reps, or offer you lunch. But, Lithium needs a drug rep, and I'm gonna be that guy.
(that was exhausting!)
Correction: the "2015 meta-analysis" referenced in the EFFICACY section is the 2014 Severus reference. (Thx @SameiHuda )
Addition: a great review of lithium kidney toxicity.
bmcnephrol.biomedcentral.com/articles/10.11…
(Thanks @MDaware )
bmcnephrol.biomedcentral.com/articles/10.11…
(Thanks @MDaware )








{kind=link}