
@teampelosi @EnergyCommerce @WaysMeansCmte @EdLaborCmte @SenateHELP Over 100 physician specialty societies & state medical societies are urging you to solve surprise billing with #IDR. drive.google.com/file/d/1YdR6HF…
A chorus of independent physicians (not PE companies or the people who surprise bill) recognize the danger of a benchmark solution and are asking you to listen.
"Simply put, certain proposed solutions for surprise billing will kill you or someone you love."linkedin.com/pulse/your-chi…
"Simply put, certain proposed solutions for surprise billing will kill you or someone you love."linkedin.com/pulse/your-chi…
The health policy "experts" you have heard from don't want to tell you about EMTALA. You MUST understand EMTALA in order to understand how new benchmark regulation would cede #RateSetting power to #BigInsurance at the expense of patients & the safety net.
EMTALA is an unfunded, federal anti-dumping mandate that requires physicians to provide medical screening and stabilization to EVERY patient who walks through the ER door, regardless of ability to pay, their balance owed, their insurance or whether their insurer has contracted.
If a physician violates EMTALA, they face civil penalties of $100K per violation (not per patient) that are not covered by malpractice insurance. Since the hospital also can be fined, a physician who makes a mistake would likely lose employment.
In effect, since "medical screening exam and stabilization" are not well defined, in effect, EMTALA means that physicians and hospitals treat all patients the same, regardless of what rate their insurance will pay or whether they will get paid at all.
EMTALA applies to every patient an ER doctor sees, but also to those specialists like neurosurgeons who have agree to "take call" for a hospital. ER docs are great, but we aren't neurosurgeons and we rely on specialists to come to the hospital and perform life saving procedures.
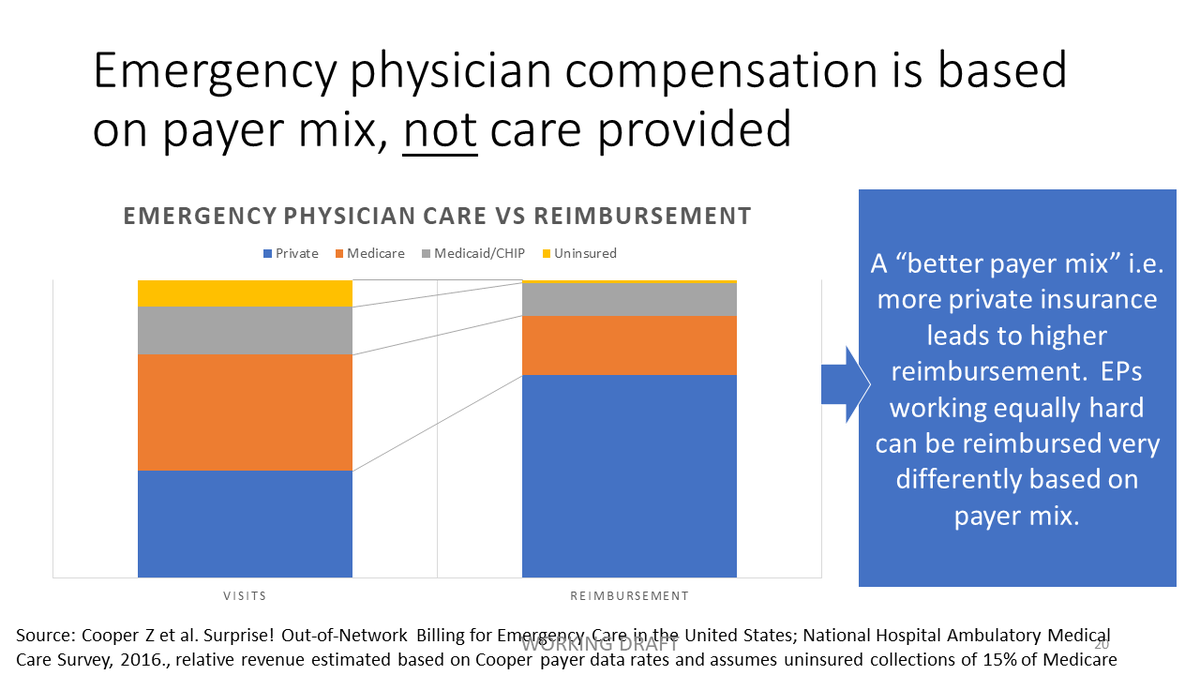
Because of EMTALA, EM physicians comprise just 4% of doctors yet provide 2/3 of all acute care visits for the uninsured and 1/2 of the Medicaid/CHIP visits. We can't limit the number of lower or non-paying patients we see. 

But this also means that ER docs don't get paid for a lot of the care we provide and our compensation depends on "payer mix." Many of us work in independent private practice groups. We don't have salary guarantees. Much of the care we provide is, literally, free.
Office-based practices can limit the number of Medicaid or uninsured patients they see. They don't have to see a patient again who owes a balance. They can choose to contract with insurers, or not. Insurers need "network adequacy" to ensure that their subscribers will be seen.
But this is NOT the case for hospital-based physicians subject to EMTALA. Insurers do NOT have to guarantee "network adequacy" for us. They know their subscribers will be taken care of in an emergency and that they can refuse to pay after the fact.
This is why the benchmark cedes rate setting to #BigInsurance & starts a #RaceToTheBottom. Insurers don't need to contract anymore to get in-network rates. So they will drop out of any contracts above the "median in network." And then the median will drop. highyieldscript.com/take-action-ag…
Independent physician groups cannot defend against this. We believe it is a virtual certainty that insurance companies, with a fiduciary duty to shareholders alone, will step away from the contracting table and take advantage of this regulatory mechanism to manipulate rates down
You may think it isn't a problem to decrease physician reimbursement by 20-40%, but it is. It may save a lot of money or CBO currency, but it will have very real and significant costs. kevinmd.com/blog/2019/07/p…
When physicians become "the most expensive cost" to the hospital, competing with nurses and equipment, physician staffed hours will likely be cut. This will translate into longer wait times, more errors and increased patient morbidity and mortality.
25% of rural hospitals are already at risk for closure. They can't afford to provide more "subsidies" to pay for physicians. When a rural hospital closes mortality increases by 6% in the rural area with an increase in mortality at the high-occupancy receiving hospital as well.
On-call specialists like neurosurgeons, OB, orthopedists come in 24/7/365 to care for patients now. Why would they do so when they can just work in their office and operate at their outpatient surgical center? Call lists will become empty and patients will have to transfer.
There are many situations here time means the difference between life and death. As with rural hospital closures, patients will die because they can't access timely care.
The "experts" like to tell you that EM docs are paid too much because the average commercial contracted rates are ~300% of Medicare and higher than other office-based specialties. This demonstrates they don't understand the market at all...or they are being deceptive.
(To start with, it’s kind of absurd that economists are arguing that an administered price - Medicare - is a better approximation of the true market than the actual market.)
Here are a number of reasons why their argument is faulty. 1) the contracted rates aren’t the actual rates paid. The net or “effective” rate is much lower. Because insurers refuse to collect coinsurance & deductibles & force docs to do it so they can shift costs to us...
Our bad debt is huge yet care for patients regardless under EMTALA. High deductible health plan design is bankrupting patients and they can’t afford to pay their deductible. Overall, providers are paid just 15% of the balances. crowe.com/news/rca-q4-20…
So the rate we are actually paid by those with commercial insurance is much lower than the contracted rate. This phenomen differentially impacts hospital-based physicians due to EMTALA. 2) Medicare rates do not include an adjustment for the impact of the unfunded EMTALA mandate.
3) Medicare rates don’t take into account the shift differential pay required to staff on nights/weekends/holidays 4) Medicare rates don’t take into account the “standby costs”. An ER doc has to show up and be ready for an unplanned emergency...
...yet they don’t get reimbursed anything for the readiness and availability. 5) Medicare rates don’t take into account convenience of nearby, 24/7/365 care yet the market does.
So, honestly, the argument that ER docs are paid at inflated rates and proven by high % Medicare contracted rates is...wrong.
Once you understand more about EMTALA, the more accurate conclusion would be that it shows Medicare administrated rates are actually wrong.

And you may think that physicians make too much money and deserve to have their pay cut. But an overnight 20%+ pay cut will have severe impacts. It will drive independent practice physicians to become employed and, ironically, increase prices through consolidation.
Uwe Reinhardt wrote: “If we...cut that take-home pay [of all physicians] by, say, 20%, we would reduce total national health spending by only 2% in return for a wholly demoralized medical profession to which we so often look to save our lives.”forbes.com/sites/physicia…
The CBO itself estimated that 80% of benchmark savings comes from 20% cuts to rates of previously in-network physicians - the ones who don’t surprise bill. But they actually underestimate the impact because they don’t account for downward spiral in rates due to EMTALA.
This amount of collateral damage is not acceptable. It will have devastating impacts on the emergency care system.
Imagine if EM docs at hospitals across the country decided to keep bankers hours for a single weekend. CBO would tell you it would save a lot of money...but what would the real cost be? We know, unfortunately, that it would staggering.











