starting #ACCPAM19 with the amazing @emilylheil presenting an update on the recently-published community-acquired pneumonia #CAP guidelines ncbi.nlm.nih.gov/pubmed/31573350 
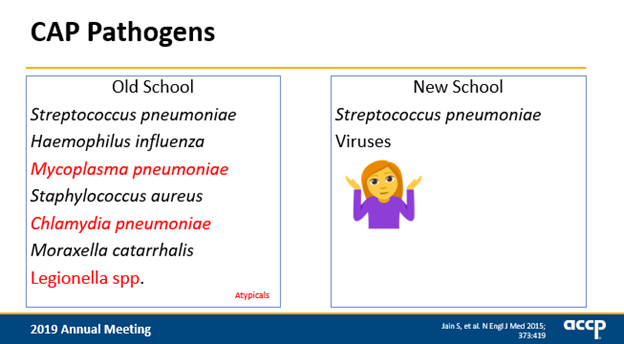
@emilylheil So what actually causes CAP? @emilylheil states "the pathogenesis and etiology of CAP has changed over time with increased rates of vaccination and better diagnostics." Jain et al 2015 unable to identify a pathogen in > 60% of patients, viruses most common
ncbi.nlm.nih.gov/pubmed/26172429
ncbi.nlm.nih.gov/pubmed/26172429
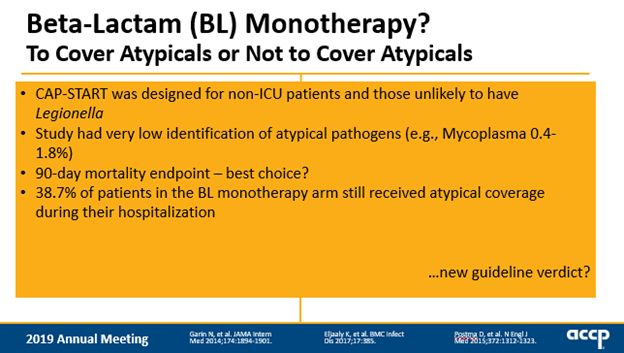
@emilylheil Since etiology a great unknown, do we need to cover atypicals? Garin et al found BL monotherapy NOT non-inferior to combo, but on flip CAP-START suggested atypical coverage perhaps unneeded...
ncbi.nlm.nih.gov/pubmed/25286173
ncbi.nlm.nih.gov/pubmed/25830421
ncbi.nlm.nih.gov/pubmed/25286173
ncbi.nlm.nih.gov/pubmed/25830421
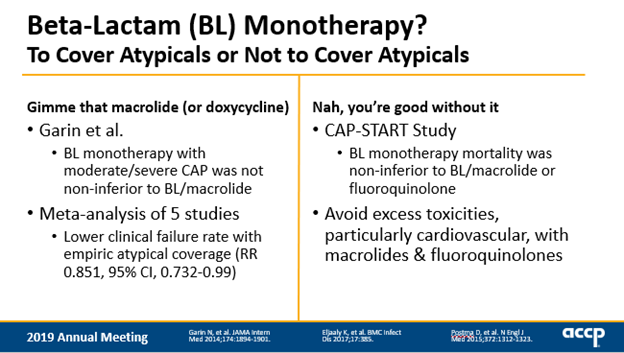
@emilylheil Challenge is CAP-START designed for non-ICU pts, had low identification rates of atypical patients, questionable endpoint for acute infection. Prescribers could add on other antibiotics for non-CAP indication, so 40% of patients in monotherapy arm had atypical coverage #accpam19
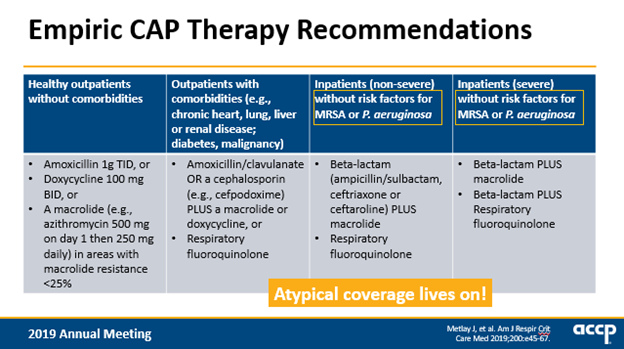
@emilylheil after great background @emilylheil moves into #CAP guideline recommendations "new to the party we have amoxicillin” (!!!) targeting S. pneumoniae, the most common bacterial pathogen. Zpacks have been demoted unless resistance less than 25%, EVERYWHERE in US has resistance >25% 🤦♀️
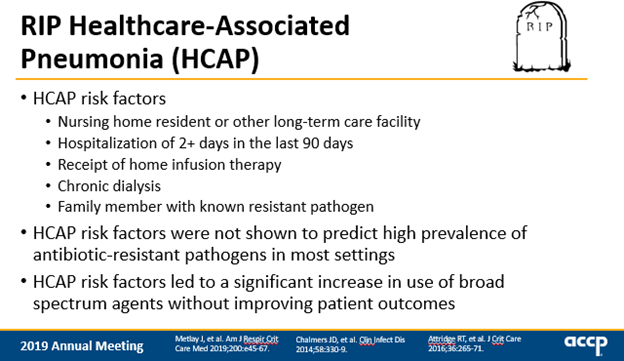
@emilylheil what about HCAP? the 2007 risk factors for healthcare-associated pneumoniae were not good at predicting patients with MRDO, but led to massive overuse of broad spectrum. luckily this concept was retired with new guidelines☠️
@emilylheil a beautiful pause in this talk to remind the audience that the NPV and PPV of a test or score *is dependent on prevalence* of disease. also love @emilylheil's trick to remember sensitive (SNout = rule out) vs specific (SPin = rule in) #ACCPAM19
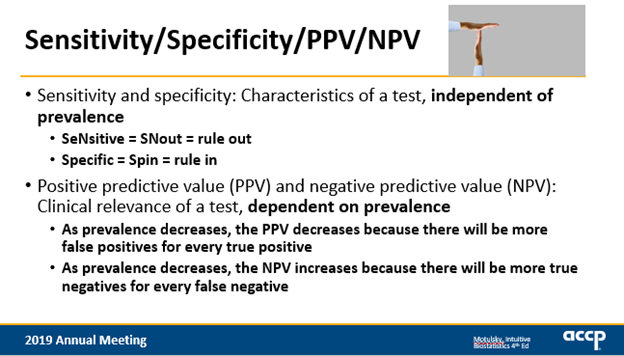
@emilylheil @accpinfdprn love that @emilylheil takes a moment in the talk to remind the audience that the NPV and PPV of a test *is dependent on disease prevalence*. also love her way to remember sensitive (SN = rule out) vs specific (SPin = rule in) #accpam19
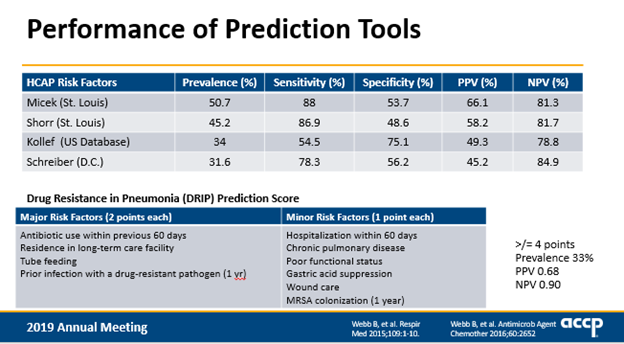
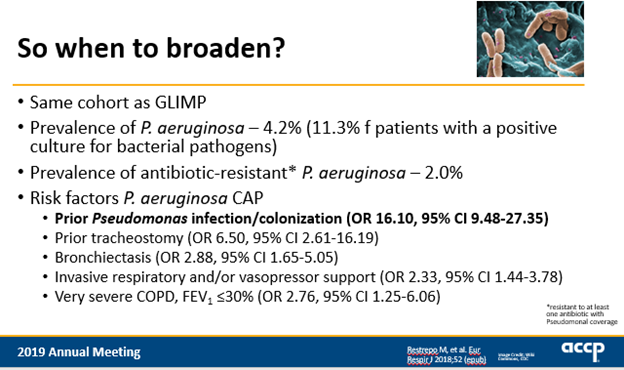
@emilylheil @accpinfdprn so we want to know who are the patients who are most likely to need MRSA/pseudo coverage up front, and risk scores don’t perform well . There’s no silver bullet to say who needs empiric coverage, unfortunately. #cap #accpam19
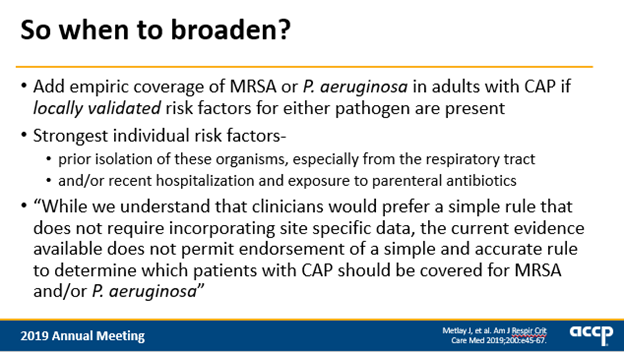
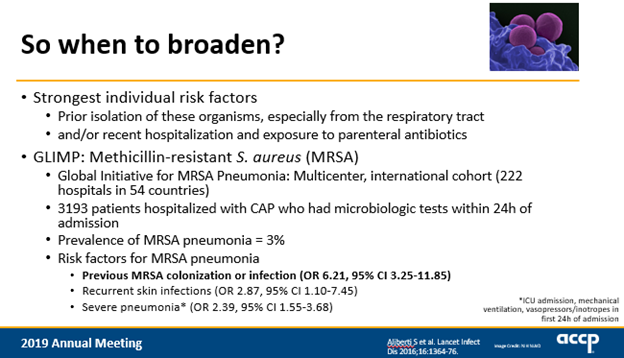
@emilylheil @accpinfdprn guidelines put emphasis on local epi and point out how strongest individual risk factors are patient-specific history of abx exposure, hospitalization, and MDROs #accpam19 @emilylheil with best quote of conference: "you can drive a mack truck thru that confidence interval"
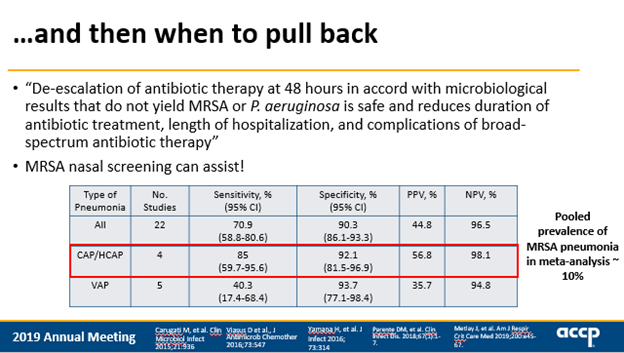
@emilylheil @accpinfdprn if you start MRSA/pseudo therapy, guidelines say you can and should de-escalate therapy at 48 hours in patients that don’t yield MRSA or P. aeruginosa. "It is safe and the stewardly thing to do" MRSA nasal screening can assist (based on a pooled prevalence of MRSA pneumonia ~10%)
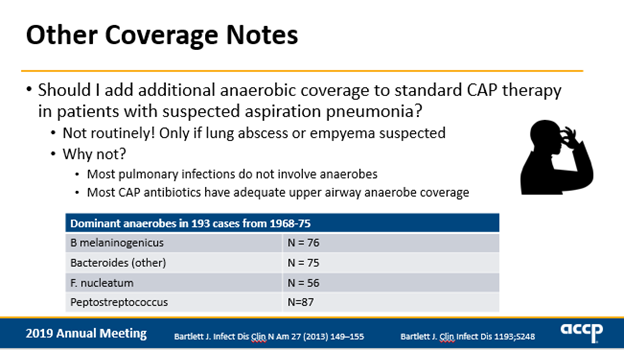
@emilylheil @accpinfdprn .@emilylheil: "I want to give the guidelines a big hug when I saw this recommendation” Unless patient has suspected lung abscess or empyema, you do not need anaerobic coverage #ACCPAM19 #CAP
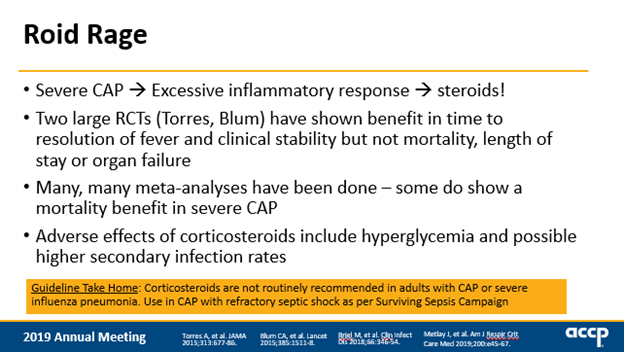
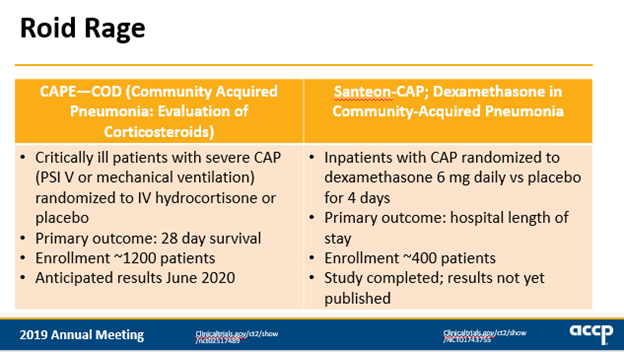
@emilylheil @accpinfdprn Guidelines address potential adjunctive role of corticosteroids in #CAP. Can steroids help temper inflammatory response? Authors state no—do not routinely recommend steroids in patients with CAP unless patient has refractory septic shock #accpam19
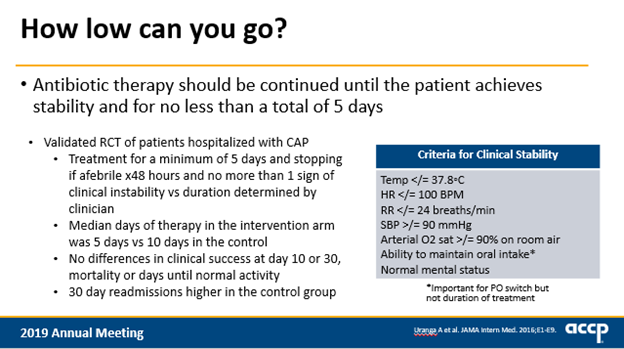
@emilylheil @accpinfdprn duration of therapy recommendation is short and sweet:
5 days is about all we need for most patients with #CAP
5 days is about all we need for most patients with #CAP
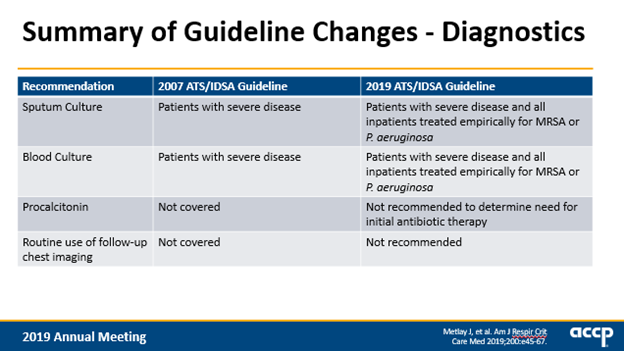
@emilylheil @accpinfdprn nice slides from @emilylheil reviewing other changes from 2007 to 2019 #cap guidelines. Cultures recommended in anyone you’re treating empirically for MRSA and Pseudomonas to help tailor therapy as well as to track and validate your local epi and risk factors. #accpam19
@emilylheil @accpinfdprn to touch on remaining issues: FQ recommended first-line for #CAP, but always consider your patient and choose the safest therapy
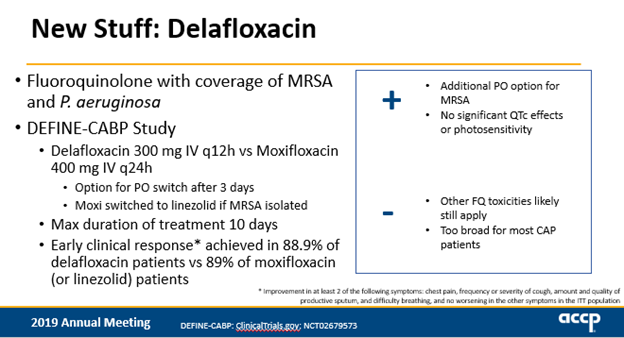
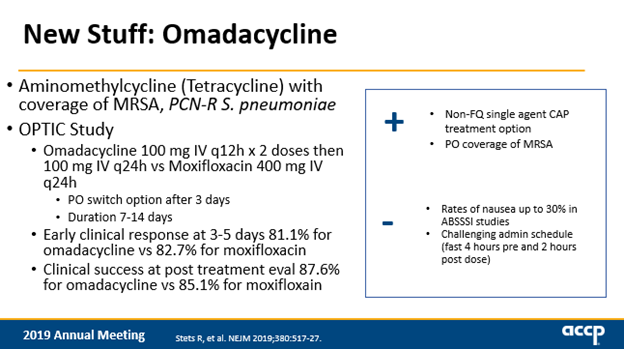
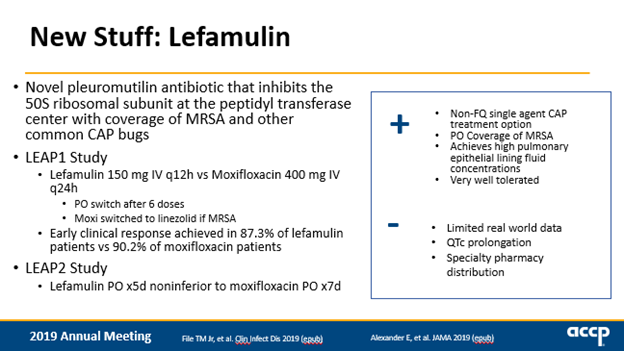
@emilylheil @accpinfdprn last but certainly not least: recently FDA-approved drugs for #CAP! Delafloxacin, omadacycline, and lefamulin all shown non-inferior to moxifloxacin. #ACCPAM19
clinicaltrials.gov/ct2/show/NCT02…
ncbi.nlm.nih.gov/pubmed/25286173
ncbi.nlm.nih.gov/pubmed/25286173
clinicaltrials.gov/ct2/show/NCT02…
ncbi.nlm.nih.gov/pubmed/25286173
ncbi.nlm.nih.gov/pubmed/25286173
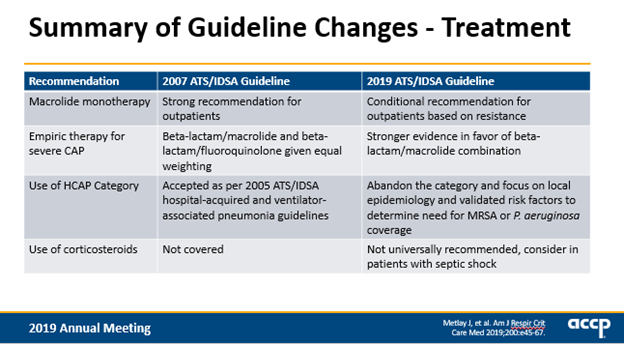
@emilylheil @accpinfdprn .@emilylheil brings it home to summarize 2019 #CAP guidelines at #ACCPAM19: treatment regimens for CAP haven’t substantially changed since 2007. HCAP replaced by individualized risk factors. Don’t give steroids. 5 days good for most patients. Watch for role of new agents.
@emilylheil @accpinfdprn thank you @emilylheil for being funny and brilliant and sending me your slides in advance to help create this #tweetorial 🤗 #accpam19 #cap #idtwitter #medtwitter