1/ This is the third #tweetorial #MedThread on contrast nephropathy from my grand rounds. For more information take a look here: pbfluids.com/2019/11/contra…
2/ The 1st #Tweetorial looked at the lack of evidence tying contrast to AKI. The 2nd looked at data tying poor clinical outcomes to CIN and if it was causal or not (it’s not).
3/ This #Tweetorial #MedThread deals with the major question, “if it’s not CIN causing AKI, what is it?”
4/ the question of what is causing AKI after contrast is going to have lots of answers but the curious case of radial catheterizations deserves examinations. 

5/ for the last decade or so we have seen a movement from femoral to radial access for cardiac catheterizations.
Early reports showed lower complication rates among other advantages for the radial procedure but these were largely case series.
Early reports showed lower complication rates among other advantages for the radial procedure but these were largely case series.
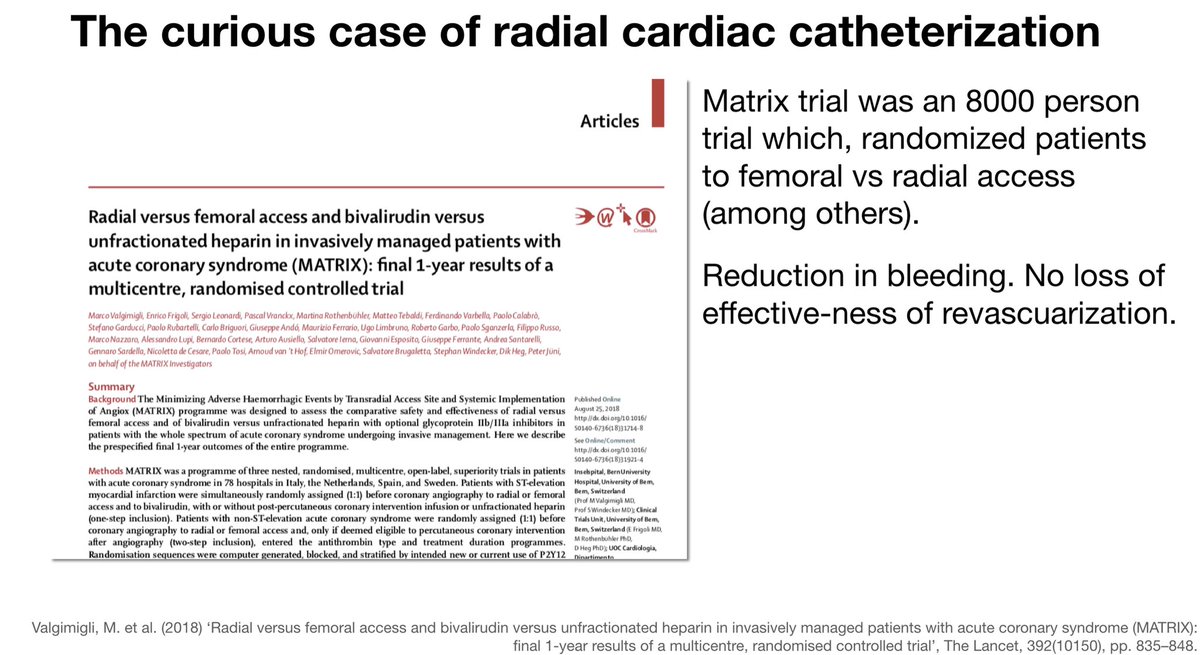
6/ the MATRIX Trial (Lancet 2018)was an RCT that compared radial to femoral approach. It showed definitively that radial was safer with similar therapeutic outcomes. sciencedirect.com/science/articl…
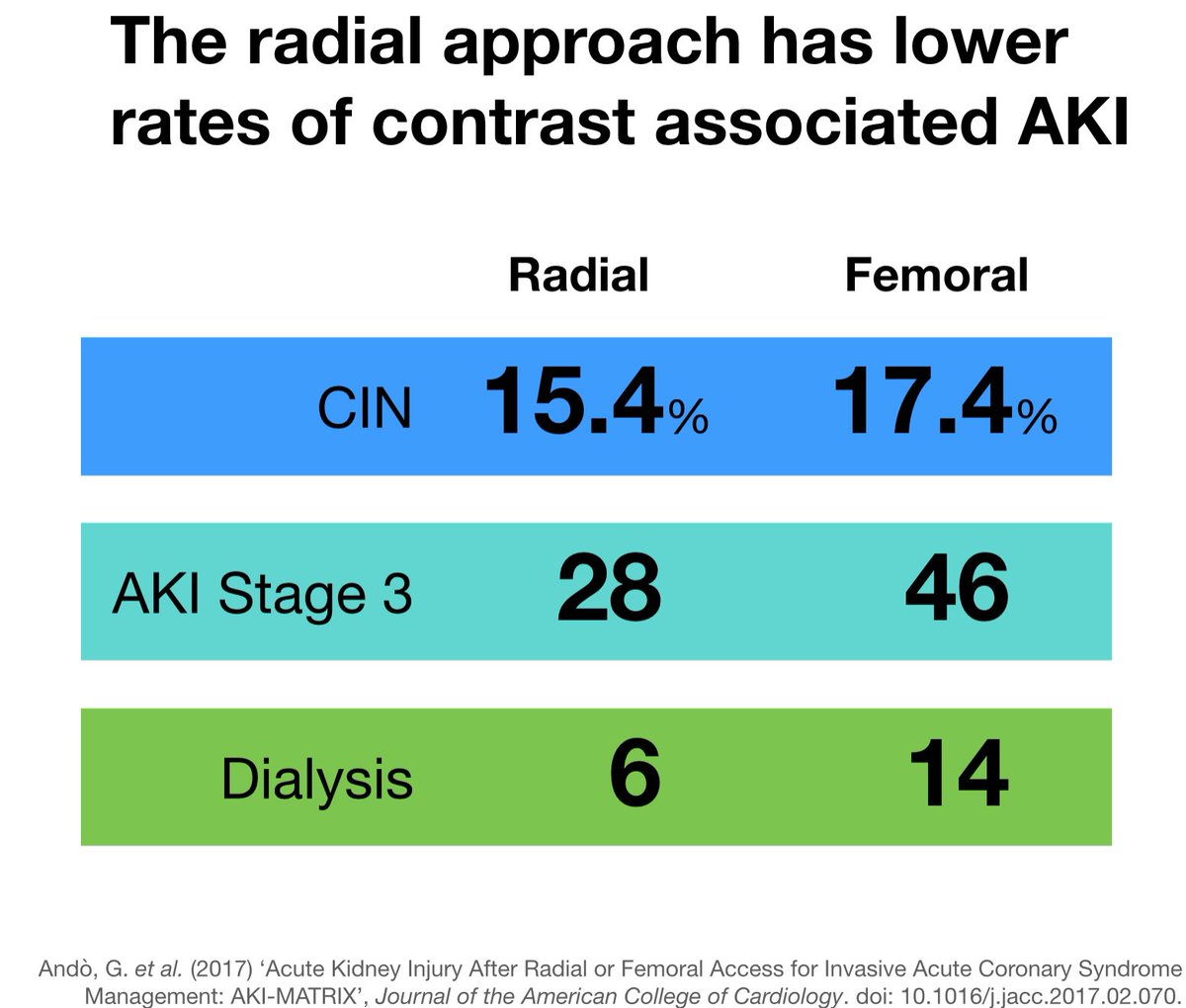
7/ One of the secondary outcomes of the MATRIX trial was the rate of contrast nephropathy. These results were published in a separate publication. The rate of AKI after cath was significantly lower and the rates of the worst AKI was even more improved. ncbi.nlm.nih.gov/pubmed/28528767
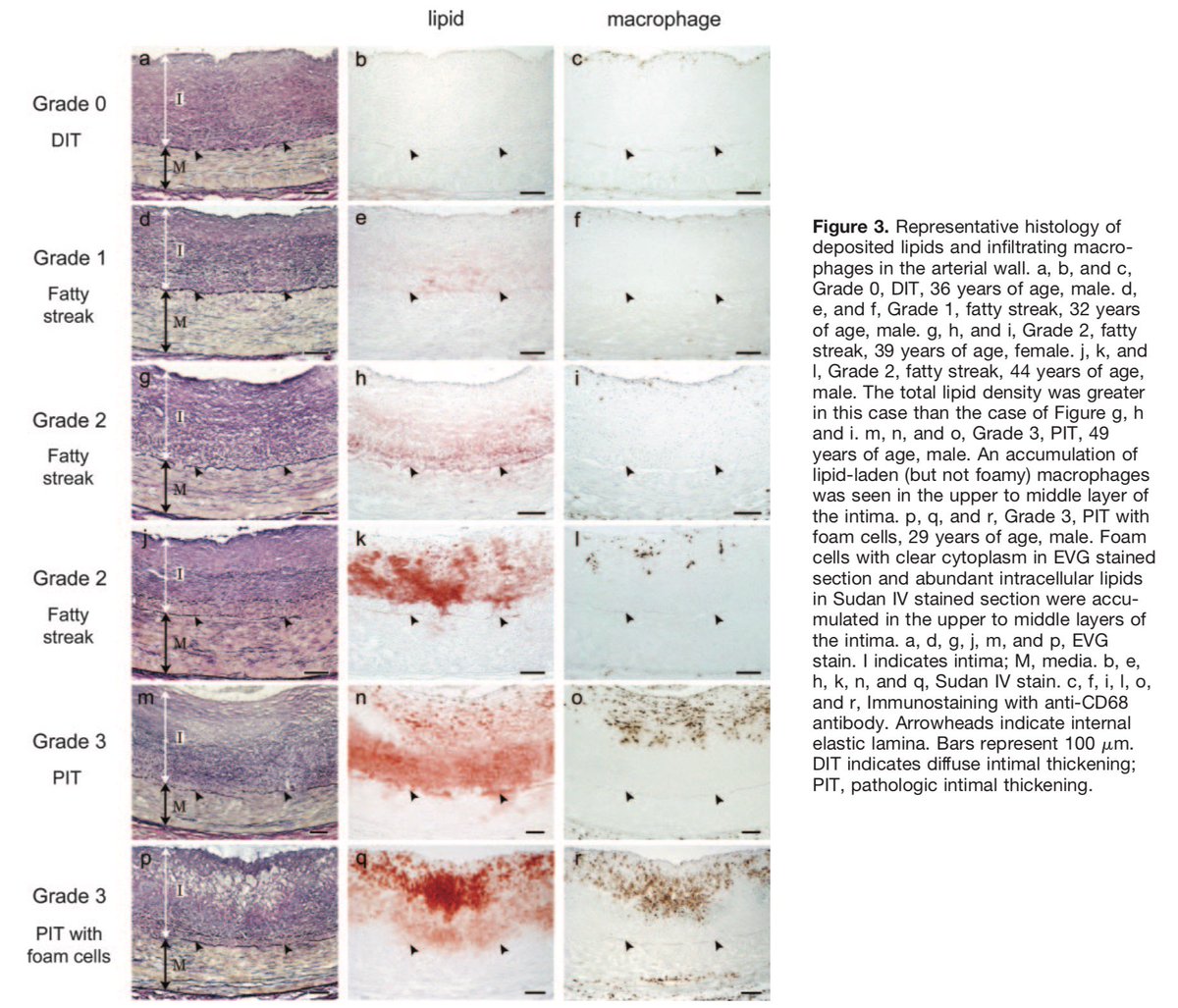
8/ the authors suggest the lower rate of major hemorrhage was the factor that increased renal safety, but nephrologists I’ve spoken with suspect an alternative explanation: decreased cholesterol emboli syndrome
9/ cholesterol emboli syndrome occurs when the catheter disrupts the fibrous cap on a cholesterol plaque allowing cholesterol crystals to float downstream causing all kinds of inconvenient ischemia.

10/ in prospective trials, evidence of cholesterol emboli syndrome can be found in 1% of caths. However in autopsy series following cardiac caths or aortic instrumentation the rate of renal biopsy findings consistent with cholesterol emboli syndrome ranges from 10-70%.

11/ So perhaps the way to reconcile the conflicting signals of
1. AKI after cardiac cath
2. Lack of toxicity w/ venous contrast
3. Decreased AKI with radial cath
Is sub-clinical cholesterol emboli syndrome.
1. AKI after cardiac cath
2. Lack of toxicity w/ venous contrast
3. Decreased AKI with radial cath
Is sub-clinical cholesterol emboli syndrome.
12/ An implication of this is that 0 contrast cardiac caths (yes, that is a thing) would still have some degree of AKI. In fact, I had one patient that I diagnosed with contrast nephropathy after a cath only to later find that the contrast dose was 0 😱
academic.oup.com/eurheartj/arti…
academic.oup.com/eurheartj/arti…
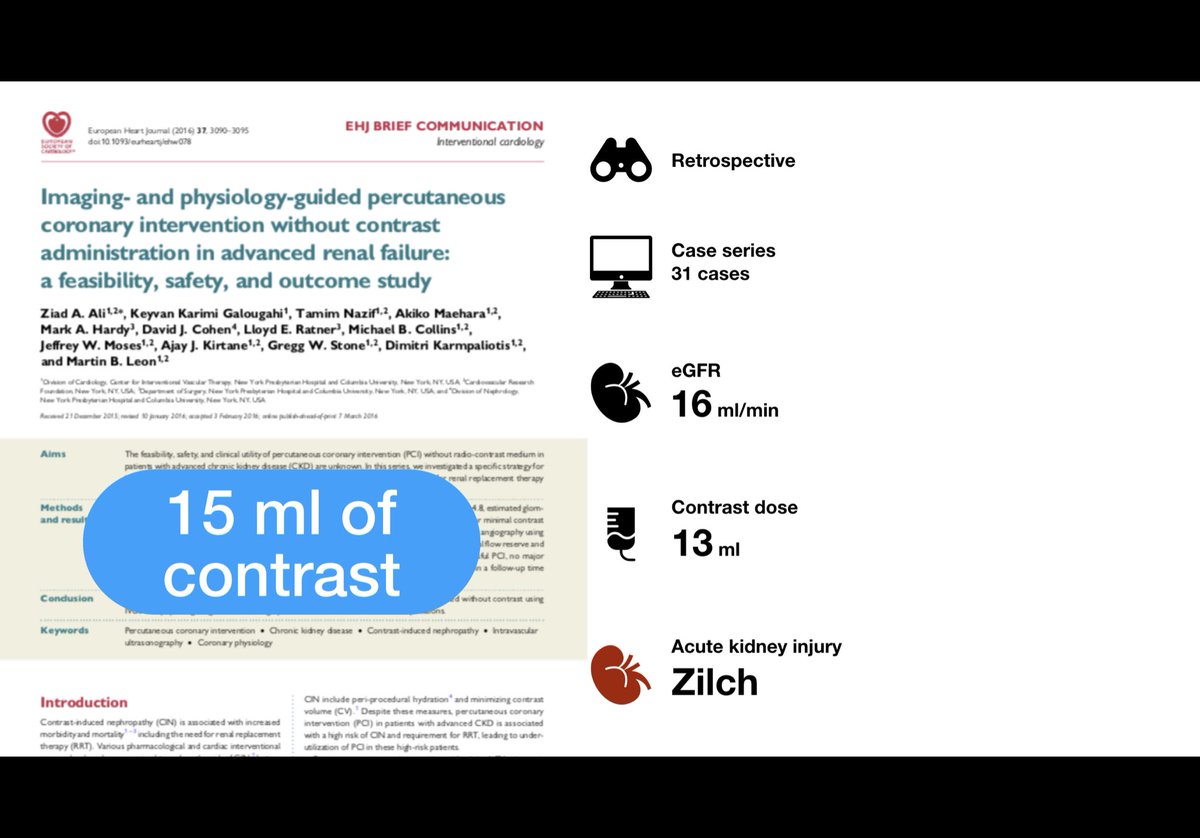
12/ Fun fact: when researchers want extremely accurate measures of GFR they don’t use eGFR like MDRD or CKD-EPI they measure GFR (mGFR) and usually use 5-15 ml of iohexol or iothalamate, you know the same iodinated contrast your nephrologist screams is so toxic.