
With the opportunity to engage and influence Draft #PCN guidance, I will do a full twitter thread on each aspect of the new Service Spec!
The aim is to be objective, so there will be no screaming etc!
Why on twitter
1. I would like it to be public
2. Easy to share images
The aim is to be objective, so there will be no screaming etc!
Why on twitter
1. I would like it to be public
2. Easy to share images
Spec ONE - Structured Medicine Reviews #PCN
As a concept SMRs are a positive initiative, polypharmacy should be addressed.
As a concept SMRs are a positive initiative, polypharmacy should be addressed.
The draft assumes that the SMRs will be delivered in principle by Clinical Pharmacists. Funding for the post is available via PCN monies therefore, should not impact GP workload. 

Q - How many CPs have been recruited by PCNs up until now? How many CPs are available to start working from Apr 2020 - I need numbers to be convinced.
If PCNs cant recruit CPs who will do the SMR? Are PCNs allowed to say No to SMRs if unable to recruit CPs?
If PCNs cant recruit CPs who will do the SMR? Are PCNs allowed to say No to SMRs if unable to recruit CPs?

NHS is likely to save more CO2 emissions if it reduces the number of meetings people need to attend under #PCN driven initiatives.
So please stop this nonsense to switching meds based on this flimsy argument. Evidence the example.
So please stop this nonsense to switching meds based on this flimsy argument. Evidence the example.
The mere fact that all PCNs will not be able to recruit CP, this #SMR work will fall on the GPs!
What work / review GPs should to drop in provide the "Considerably Longer than average GP appointment"
What work / review GPs should to drop in provide the "Considerably Longer than average GP appointment"

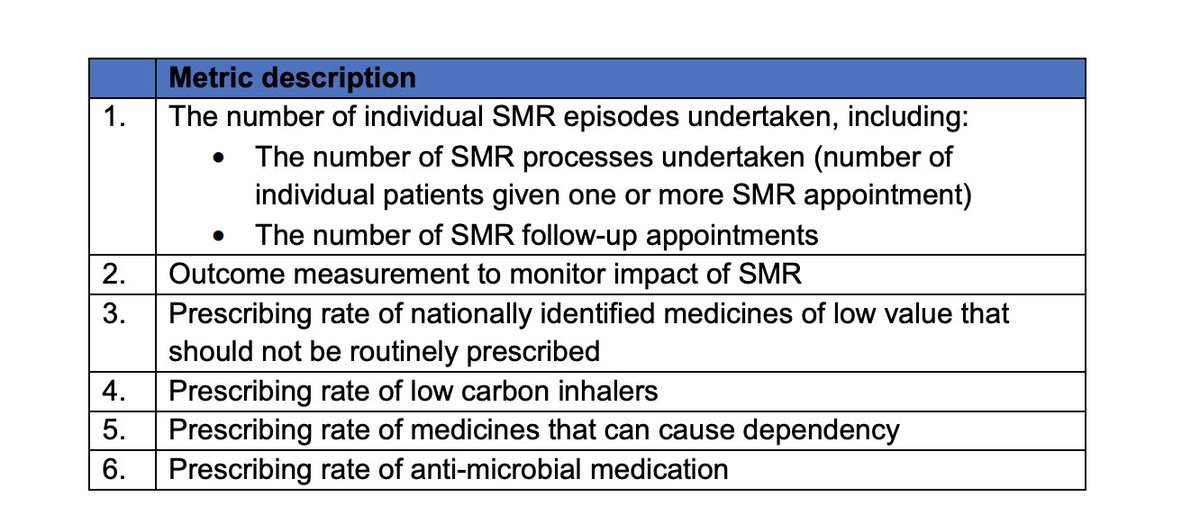
#SMR Metric - Review.
Metric 1; QoF under a different name. Will not increase Quality.
Metric 2; Need to define the impact ( not included in the spec document)
Metric 3; This is a totally wrong priority - must be removed!
Metric 4; anti-microbial rarely Rx long-term!
Metric 1; QoF under a different name. Will not increase Quality.
Metric 2; Need to define the impact ( not included in the spec document)
Metric 3; This is a totally wrong priority - must be removed!
Metric 4; anti-microbial rarely Rx long-term!
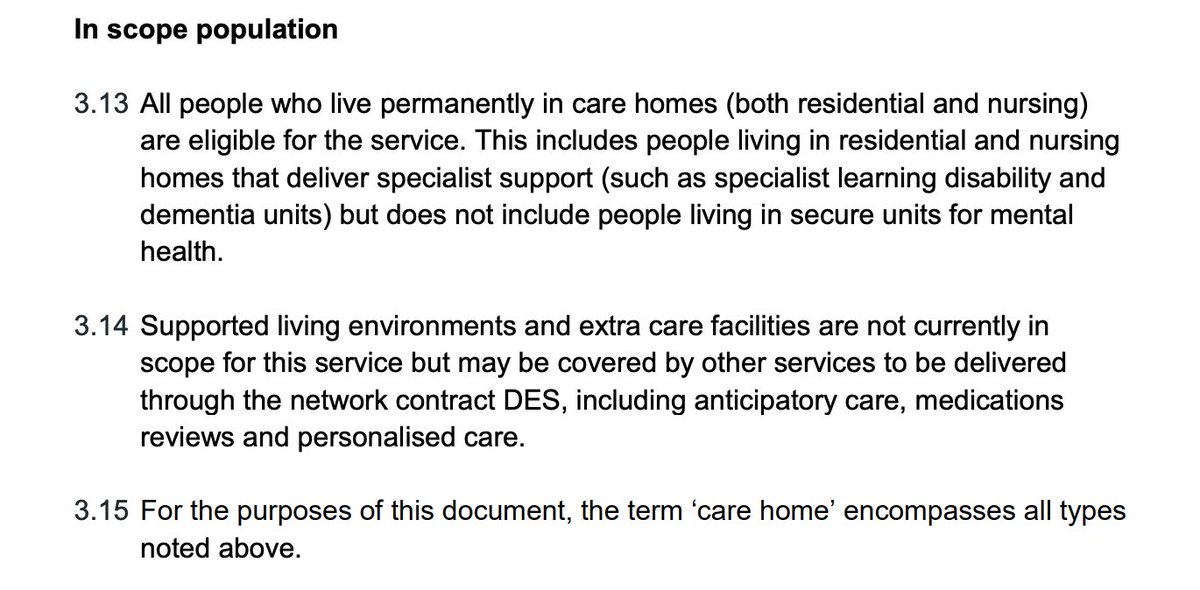
Spec Two: Enhanced Health & Care Homes.
Reading the title has put me off, what is Enhanced and Non-Enhanced ?
Is the aim of #PCN spec promoting 2 tier treatment ? People nursed in care homes to get Enhanced care & People living in their own home reduced care - Really!
Reading the title has put me off, what is Enhanced and Non-Enhanced ?
Is the aim of #PCN spec promoting 2 tier treatment ? People nursed in care homes to get Enhanced care & People living in their own home reduced care - Really!
Reading further, it is actually clear that a two tier system is being proposed under #PCN
Not that i am against providing extra support to people in NH/RH etc, but people not included in the scope may actually benefit more from Enhanced Service!
Not that i am against providing extra support to people in NH/RH etc, but people not included in the scope may actually benefit more from Enhanced Service!

Primary Care has little control over 👇Q: Should it be in GP Contract under #PCN or otherwise?

What is NHSE's fascination with Named Clinician!
JH introduced named GP concept - have things changed for the better to assume that named clinician will improve the care?
JH introduced named GP concept - have things changed for the better to assume that named clinician will improve the care?

So #EHCH becomes a contractual obligation for Primary Care under #PCN guise yet, primary care has no control over
#CountyCouncil
#CommunityProvider
#Carehomes
#MentalHealthProviders
How are GPs expected to include all other partners with no contractual commitment to #EHCH ?
#CountyCouncil
#CommunityProvider
#Carehomes
#MentalHealthProviders
How are GPs expected to include all other partners with no contractual commitment to #EHCH ?
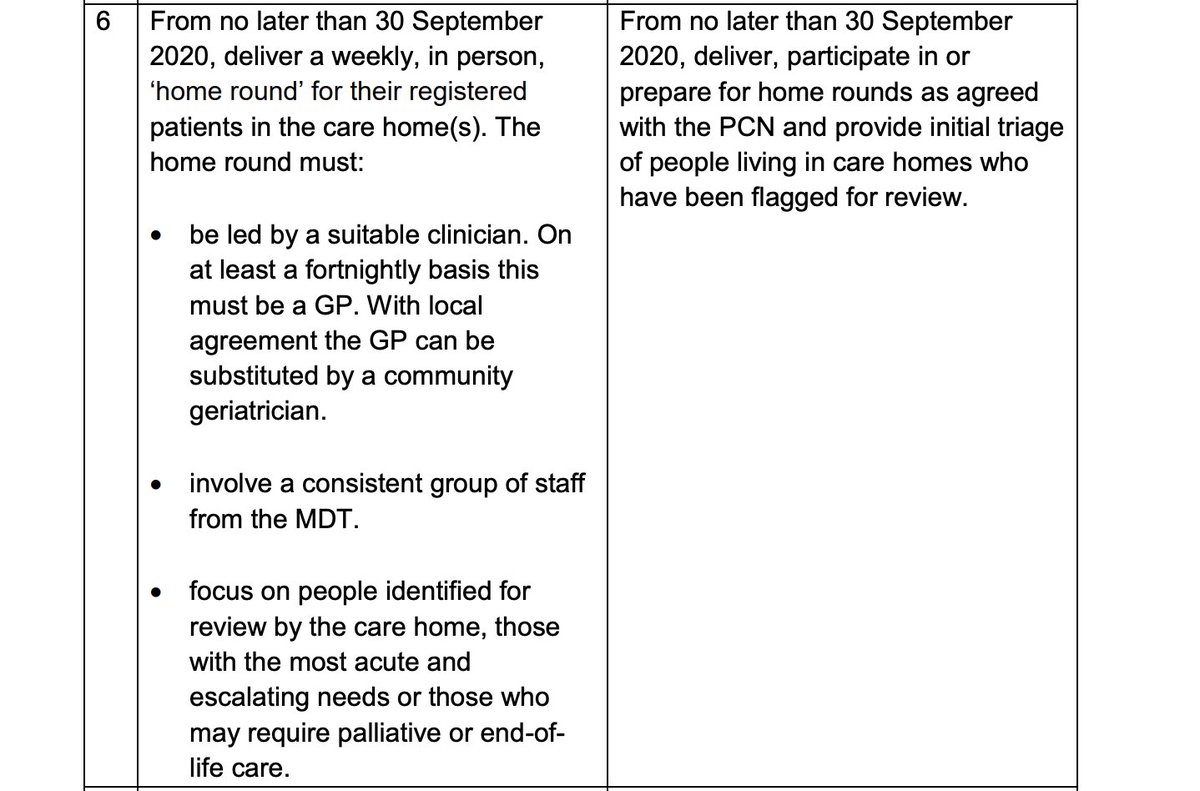
This is a cracker of a sub-spec!
NHSE assumes that every single person living in a care home is physical and/or mentally unwell and need a GP VISIT every week!
1st ask the person, family or their loved ones before making this really serious assumption!
NHSE assumes that every single person living in a care home is physical and/or mentally unwell and need a GP VISIT every week!
1st ask the person, family or their loved ones before making this really serious assumption!
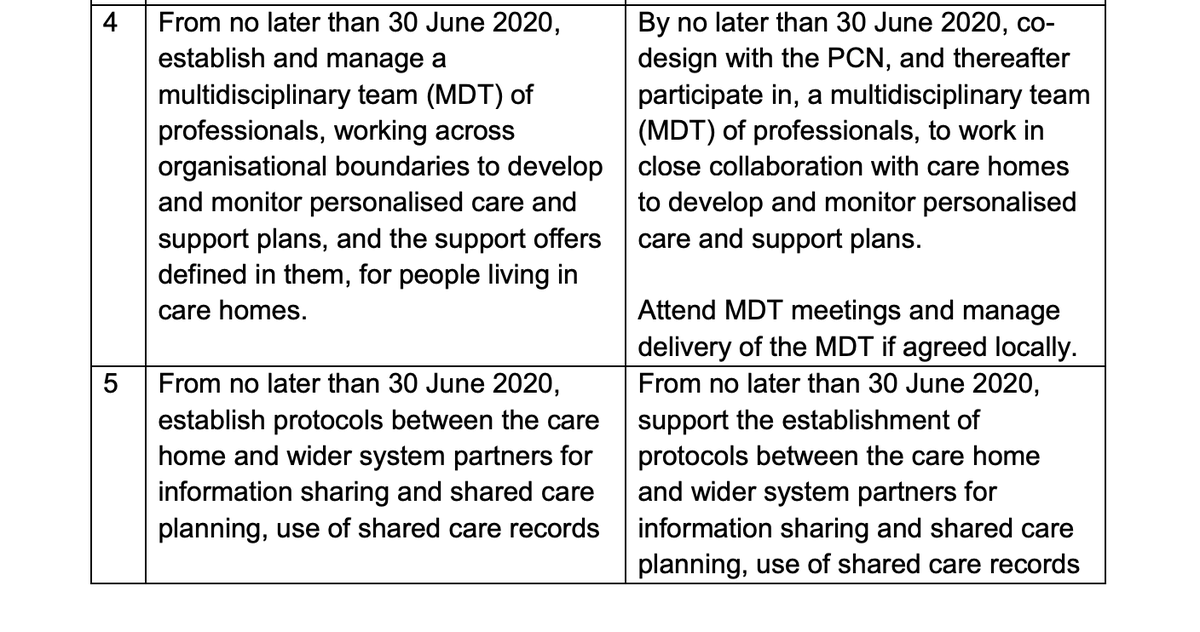
This now becoming hilarious!
I did not realise, as a GP, i can assess
1. persons' care needs,
2. Perform OT Assessments
3. Deliver Physiotherapy sessions.
4. Complete social assessments.
It is truly insulting to my OT, Nursing, Physio & other colleagues - dont like it :(
I did not realise, as a GP, i can assess
1. persons' care needs,
2. Perform OT Assessments
3. Deliver Physiotherapy sessions.
4. Complete social assessments.
It is truly insulting to my OT, Nursing, Physio & other colleagues - dont like it :(
Spec Two - EHCH
All the above tweets about EHCH may give people an impression that I am against EHCH. I am not!
I think GPs are not the right people to lead EHCH programme. NH/RH teams who looks after people 24/7 should be empowered + Funded to lead on it.
All the above tweets about EHCH may give people an impression that I am against EHCH. I am not!
I think GPs are not the right people to lead EHCH programme. NH/RH teams who looks after people 24/7 should be empowered + Funded to lead on it.
Spec Two - EHCH
I would propose: EHCH should be led by Care Homes, co-ordinate MDTs / Care needs, rehabilitation etc.
Invest in Care Homes, train the staff via NHS Leadership academy to deliver EHCH 🙏
Clinicians GPs, Nurses, OT, provide their input based on their expertise.
I would propose: EHCH should be led by Care Homes, co-ordinate MDTs / Care needs, rehabilitation etc.
Invest in Care Homes, train the staff via NHS Leadership academy to deliver EHCH 🙏
Clinicians GPs, Nurses, OT, provide their input based on their expertise.

On the whole this group of metric is doable / achievable and probably wont impact much on the GP workload.
The key challenge would be good quality PH data from ICS.
The key challenge would be good quality PH data from ICS.

#PCN Spec - 4 Personalised Service Model
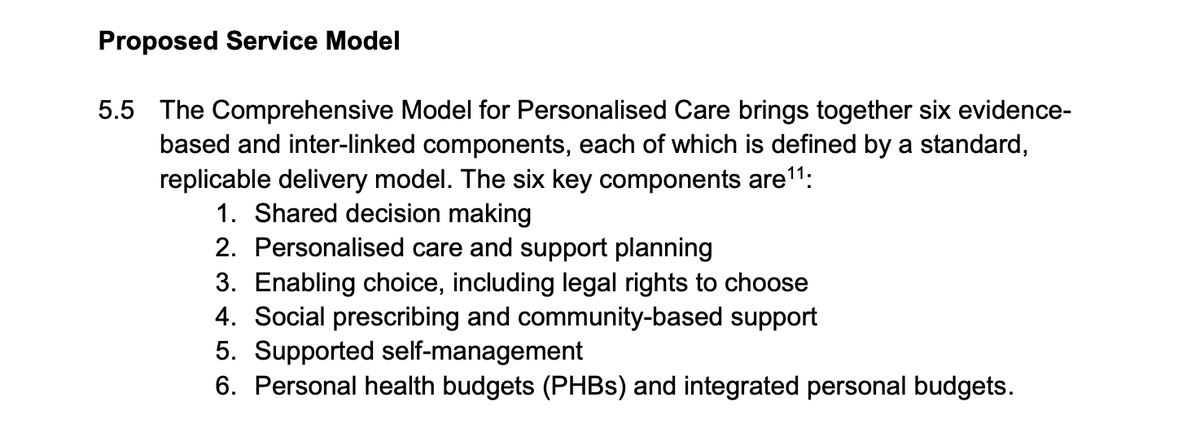
I think on the whole Personalise Service Model specs are reasonable and #PCN is the right vehicle for it.
I have particular concerns on the allocation of personal budgets. CCGs / ICPs / ICSs are interpreting it differently, especially when it comes to funds allocation!
I have particular concerns on the allocation of personal budgets. CCGs / ICPs / ICSs are interpreting it differently, especially when it comes to funds allocation!
1. GP / #PCN do not want another username / login to fill in a form for personal budget to be allocated.
2. The person should make the decision on what is best for it not what is available in the region.
3. The allocation approval process need to be 1-Click.
2. The person should make the decision on what is best for it not what is available in the region.
3. The allocation approval process need to be 1-Click.
These Folks are not well, and they know what their needs are!
👇👇 statement is a get out of jail clause!
NHSE need to mandate CCGs to approve PHB request received via #PCN not cross examine & refer to accountant!
Message: rewrite it!
👇👇 statement is a get out of jail clause!
NHSE need to mandate CCGs to approve PHB request received via #PCN not cross examine & refer to accountant!
Message: rewrite it!

Example: Patient with Inflammatory Arthritis to be allowed to spend his PHB on hydrotherapy sessions for pain relief if local NHS cant provide it, especially if recommended by specialist.

#PCN has put on a lot of emphasis on #SocialPrescribing, but how did you get the figure of 16 - 22 / 1000 pts?

Personally, i dont like the term social prescribing! If it is not medical / clinical - no need to prescribe - Just signpost.
We must resist the temptation of medicalising normal life phenomenons. Life is challenging, complicated & personal. Support not prescribe!
We must resist the temptation of medicalising normal life phenomenons. Life is challenging, complicated & personal. Support not prescribe!
What is this obsession with Clinical Lead for every domain / sub-domain. dont have already 1000+ #PCN CDs?
If each spec has to have its own CD we will end up with 5K+ CDs.
1 session / week = 20K+ sessions / year = £7M @ 350/session - Really!
Can we not work as grown ups?
If each spec has to have its own CD we will end up with 5K+ CDs.
1 session / week = 20K+ sessions / year = £7M @ 350/session - Really!
Can we not work as grown ups?

So now to Spec 4 Metrics.
Number game is never a good game. Can be won easily with no improvement in Quality only increasing the bureaucratic burden!
Suggestion: Re-define the metrics focus on quality not quantity 😊
Number game is never a good game. Can be won easily with no improvement in Quality only increasing the bureaucratic burden!
Suggestion: Re-define the metrics focus on quality not quantity 😊

Finally, it has taken me 4 hours to read the spec, think / reflect and write this twitter thread!
I have done it for myself & not for anyone else. I do not have influence at any level to enforce #PCN spec changes suggested in the above thread😊
I have done it for myself & not for anyone else. I do not have influence at any level to enforce #PCN spec changes suggested in the above thread😊








