THREAD: Differential diagnosis of tachycardias can be tricky business! Here are some strategies to help keep you between the ditches. Hope you will like and share. #FOAMed #FOAMems #MedEd #CardioTwitter 
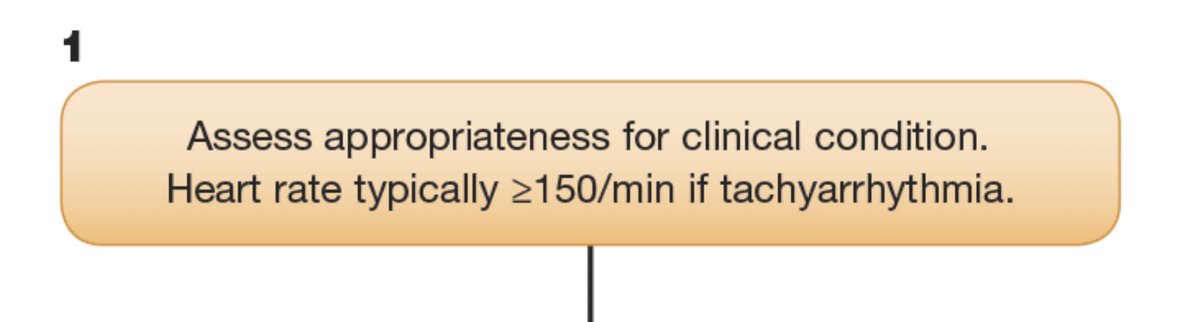
1/ First let's look at the 2015 AHA ECC Guidelines tachycardia algorithm. It's fairly straight forward but there are some important concepts here that deserve some elaboration.

2/ In the first place we're asked to consider appropriateness of tachycardia for the clinical condition. This is really important! We don't want to attack the heart rhythm if it's a compensatory tachycardia! The second part causes a lot of confusion. What is significance of 150?
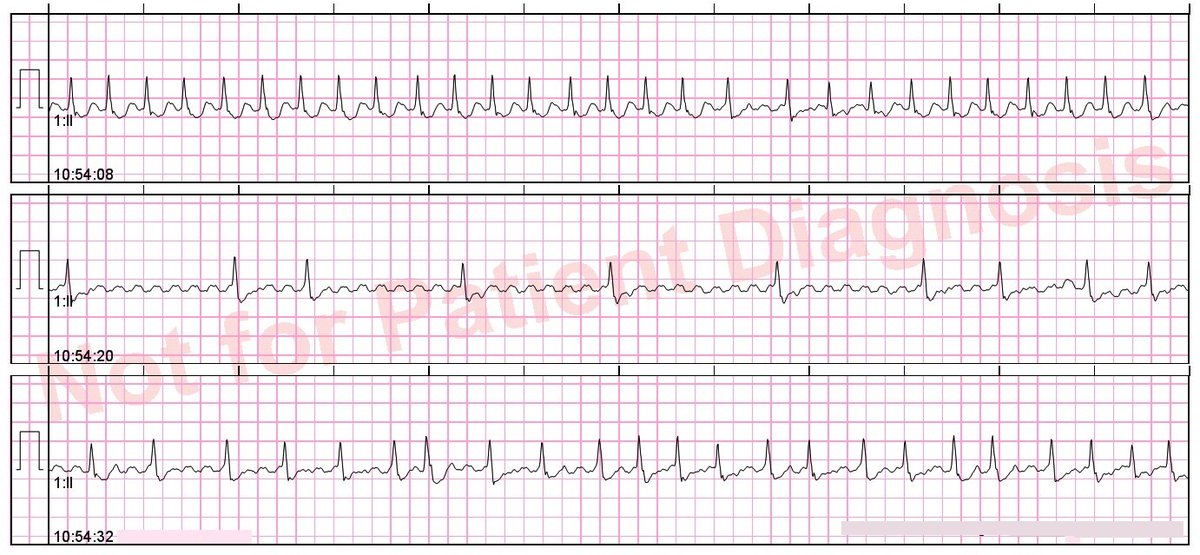
3/ It's a myth that sinus tachycardia can't be > 150. Consider this ECG from a young female who received 6/12/12 of adenosine for "palpitations". She had an elective abortion the day prior and soaked through 8 peri-pads. She was in compensated hypovolemic shock not "SVT".

4/ David Baumrind wrote a nice blog post called "The Trouble with Sinus Tachycardia" that does justice to this important topic. Of note, maximum sinus rate is approximately 220 minus age but can vary 10-15% which is a lot! ems12lead.com/2013/04/30/the…
5/ The next box says "identify and treat underlying cause". This is really important! The Hs and Ts aren't just for PEA and asystole. Consider them for bradycardias and tachycardias also! First and foremost ensure the patient is properly oxygenated. Attach pulse oximetry!

6/ Here's a case that was mistaken for ventricular tachycardia but was almost certainly life-threatening hyperkalemia! The patient died and no autopsy was performed. Note double-counting of heart rate by monitor (Littmann sign).

7/ Next we're asked if there is persistent tachyarrhythmia *causing* various types of instability. This is key decision on caregiver's part. Is today's tachycardia a cause or a consequence? Getting this wrong can be a big mistake and getting it right requires clinical judgment.

8/ If the patient is in shock and you think the tachycardia is *causing* the shock then you should go straight to synchronized cardioversion. If it is a regular narrow complex tachycardia and IV is started you can consider adenosine.

9/ Protocols vary widely when it comes to peri-procedural sedation for synchronized cardioversion. What are you using in your EMS system or ED? Let me know in the comments. Don't forget to push the "synch" button!

10/ If the tachycardia is not causing hemodynamic instability that warrants immediate synchronized cardioversion we're asked to look at the QRS duration. This is where things can start to go off the rails if you're not careful.
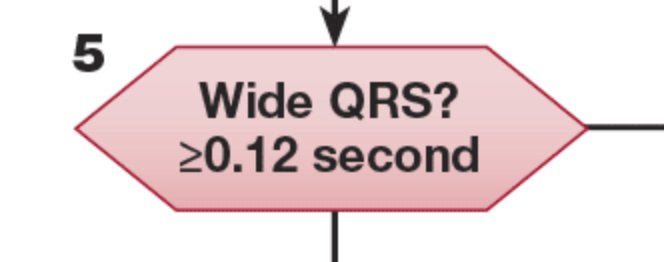
11/ If QRS is "wide" and there is "time to think" it goes without saying we should obtain a 12-lead ECG to document arrhythmia which can be invaluable to "down stream" providers responsible for patient's definitive care. Also, not always easy to tell QRS is wide w/o 12-lead ECG!

12/ We're told we can "consider adenosine" only if regular and monomorphic (solid advice as adenosine can be very dangerous for AF/WPW). Adenosine may terminate SVT w/aberrancy or even certain types of VT! Before we go any further we must confront the issue of SVT w/aberrancy.
13/ Once upon a time in EMS our monitor-defibrillators did not have 12-lead ECG capability so we learned to recognize heart rhythms in a single lead -- typically lead II.

14/ We were good at this! When testing for @NREMT we would be shown single lead rhythm strip for "static cardiology" and given a strip like this, any good paramedic would confidently say "ventricular tachycardia!"

15/ Fast-forward to 2018 and give us the *exact same* heart rhythm on a 12-lead ECG and it stops us right in our tracks. There are many reasons for this including the fact that our computerized interpretive algorithms *suck* at cardiac rhythm analysis!

16/ I am not saying this 12-lead ECG *definitely* shows VT. It could be 2:1 atrial flutter with LBBB, for example. That's not the point. What I have noticed is that many paramedics do not even include VT as part of the differential diagnosis! That's worrisome.
17/ This problem isn't just for "wide and fast" rhythms with LBBB morphology in lead V1. Here's a case of VT with RBBB morphology. The patient received adenosine but not amiodarone. Why? Because the treating paramedic didn't even consider the possibility it was VT.

18/ As a side note, for those of you saying "the right bunny ear is taller than the left bunny ear!" that is an oversimplification of Wellens' critera. By morphology criteria this ECG is perfectly consistent with VT.

19/ If your trial of adenosine doesn't work (or if you give it and nothing happens) you're probably dealing with VT and you should consider antiarrhythmic infusion or "expert consultation". Who's an expert? Good question! We don't all have access to EPs at 0300 so "do no harm".
20/ If the QRS is "narrow" (< 120 ms) and the rhythm is regular (kind of a big deal) then we proceed with vagal maneuvers and then adenosine. How do you perform vagal maneuvers? Since I'm dealing with FOAMed types I'm guessing you already know what comes next!

21/ Postural modification of Valsalva can improve conversion rate from 17% to 40%! Source: REVERT Trial - Lancet. 2015;386(10005):1747-1753).
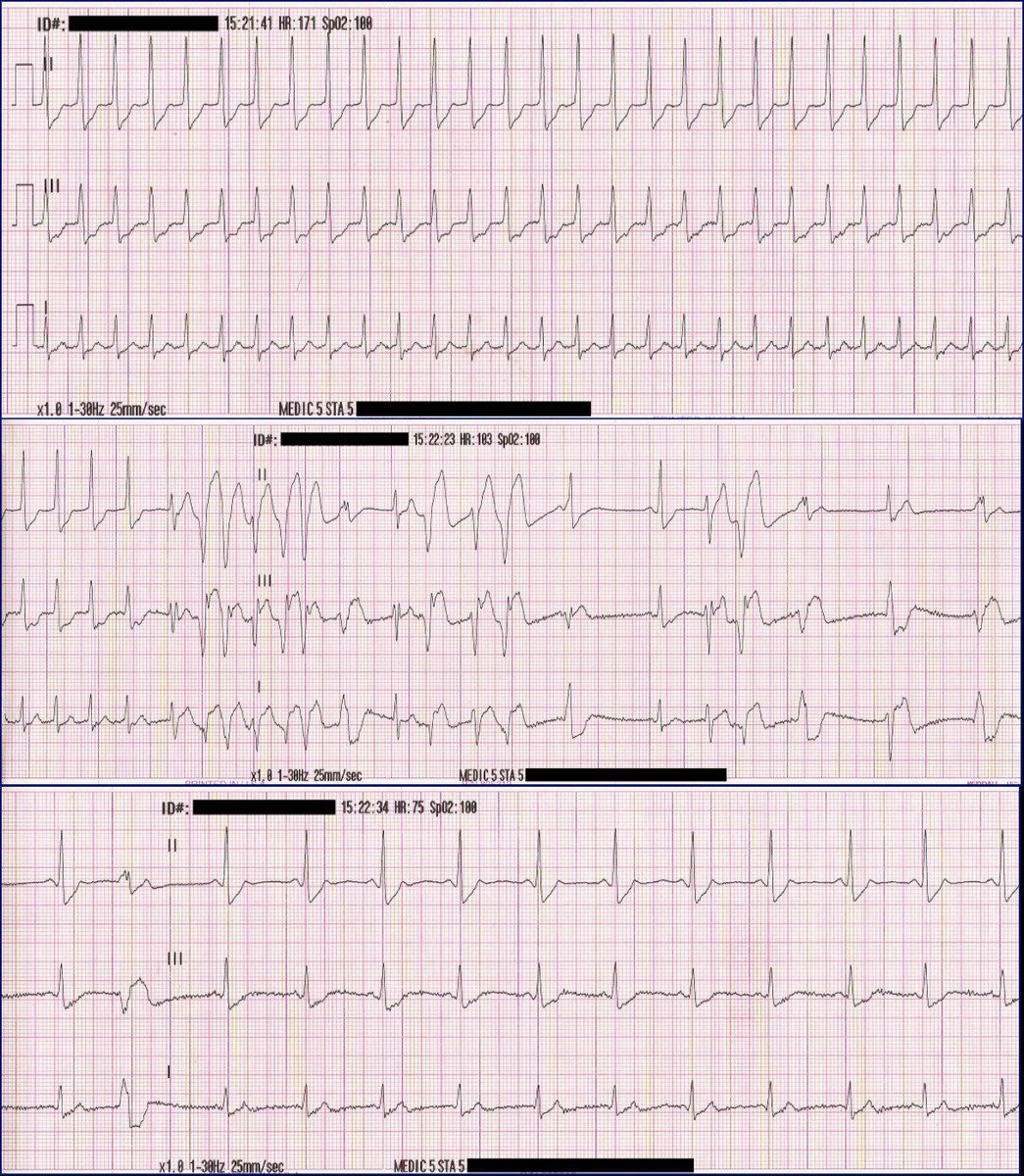
22/ Ready to proceed with adenosine? Remember to push the PRINT button! Sometimes the asystolic pause reveals underlying flutter waves. If that happens, no need for repeat doses. You'll want to switch to a calcium channel blocker for rate control.
23/ Have some compassion when giving adenosine! It doesn't feel so great. Also, patients deserve to know what's happening to them. Keep in mind that carbamazepine and dipyridamole can potentiate adenosine so use caution! Anecdotally, I have had great success with the drug.
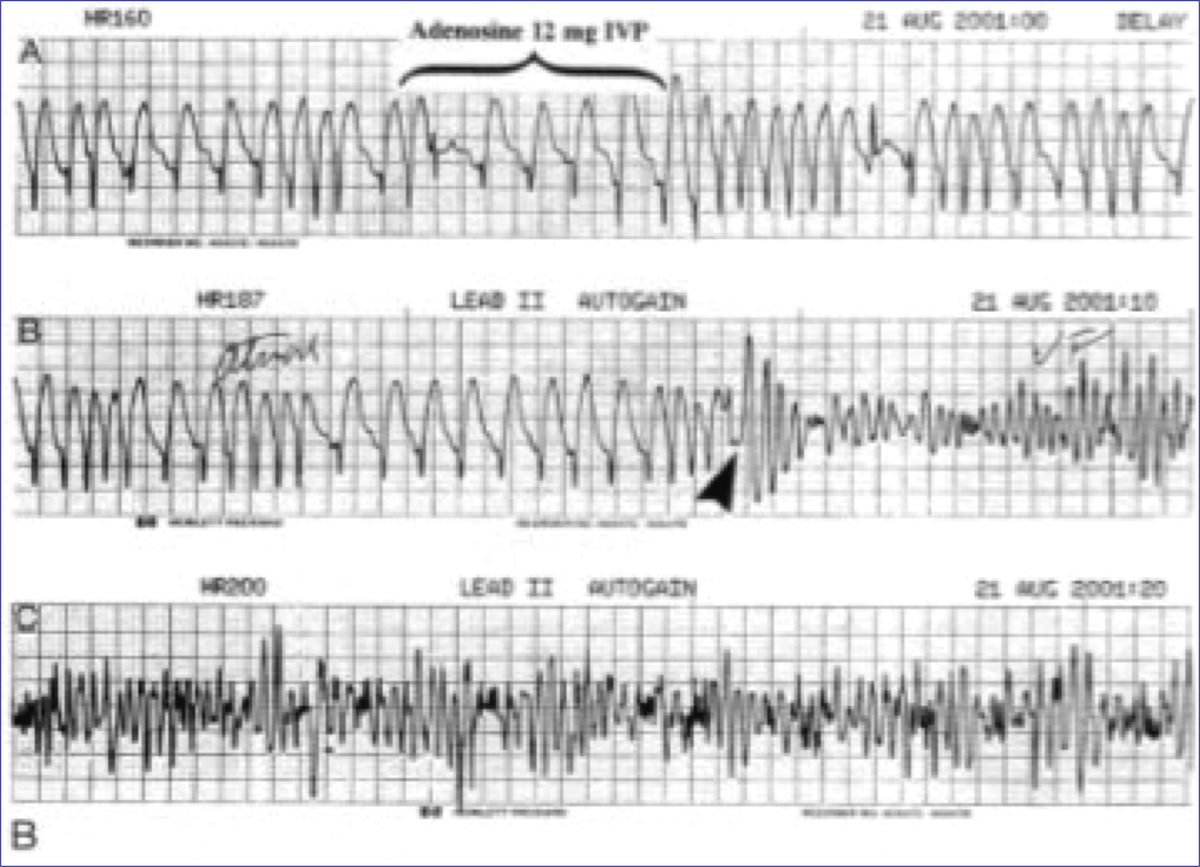
24/ Remember that adenosine is only for regular rhythms! There are several case reports in the medical literature of adenosine precipitating VF in patients with AF/WPW. Here's an example courtesy of @AndrewACNP1.
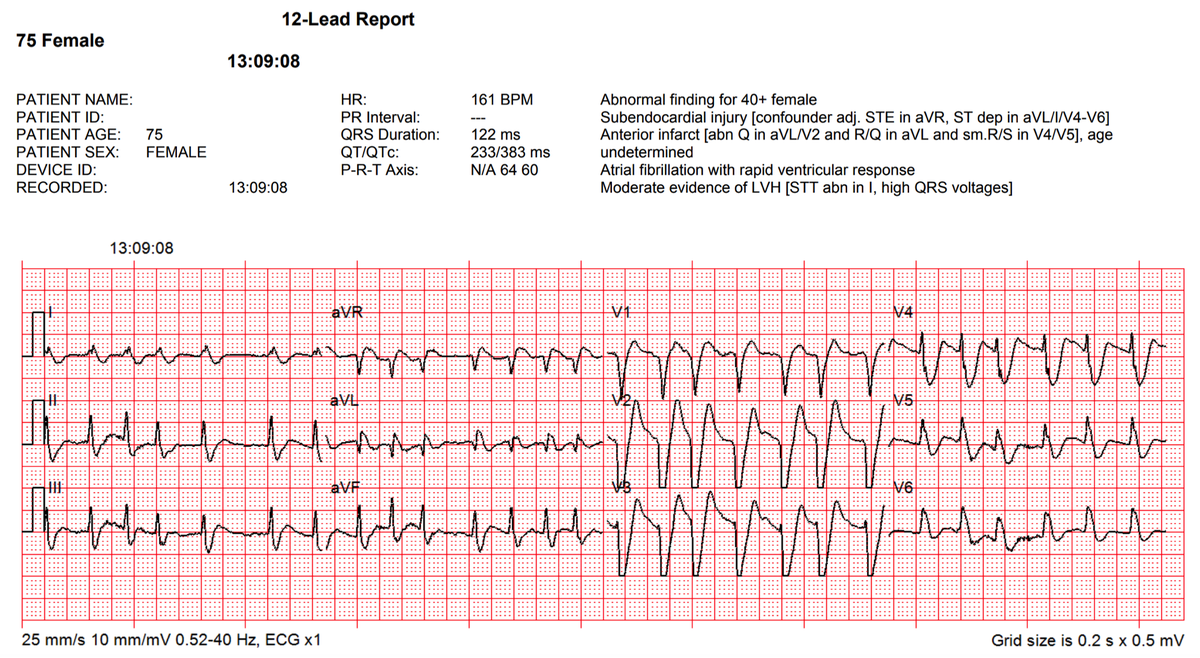
25/ Irregular or polymorphic tachycardias are a special breed. In many cases, irregular but monomorphic wide complex tachycardias can be explained by atrial fibrillation and bundle branch block. We see this a lot in patients who present in decompensated heart failure.
26/ Things get very interesting when heart rhythms are fast, irregular, and polymorhpic! These are scary patients. Differential diagnosis should include poly VT, TdP (torsades), and AF/WPW. In this example patient had prolonged QT in underlying rhythm so diagnosis is TdP.

27/ With AF/WPW there is no "turning of the points" and shortest R-R interval is often 6 small blocks or less. Here we see TdP (top) and AF/WPW (bottom).

28/ As a final thought, new onset VF can have cyclic rate close to 300 before it speeds up. So, new onset VF can mimic TdP. Very frequently I've overheard various providers announce "torsades!" when in fact the patient simply coded. Not a big deal as long as you shock it. /THREAD